

Abstract
Objective
To discuss the difficulties in dealing with infected or exposed ventral hernia mesh, and to illustrate one solution using an autogenous abdominal wall reconstruction technique.
Summary Background Data
The definitive treatment for any infected prosthetic material in the body is removal and substitution. When ventral hernia mesh becomes exposed or infected, its removal requires a solution to prevent a subsequent hernia or evisceration.
Methods
Eleven patients with ventral hernia mesh that was exposed, nonincorporated, with chronic drainage, or associated with a spontaneous enterocutaneous fistula were referred by their initial surgeons after failed local wound care for definitive management. The patients were treated with radical en bloc excision of mesh and scarred fascia followed by immediate abdominal wall reconstruction using bilateral sliding rectus abdominis myofascial advancement flaps.
Results
Four of the 11 patients treated for infected mesh additionally required a bowel resection. Transverse defect size ranged from 8 to 18 cm (average 13 cm). Average procedure duration was 3 hours without bowel repair and 5 hours with bowel repair. Postoperative length of stay was 5 to 7 days without bowel repair and 7 to 9 days with bowel repair. Complications included hernia recurrence in one case and stitch abscesses in two cases. Follow-up ranges from 6 to 54 months (average 24 months).
Conclusions
Removal of infected mesh and autogenous flap reconstruction is a safe, reliable, and one-step surgical solution to the problem of infected abdominal wall mesh.
Prosthetic mesh is widely used in the repair of midline ventral hernias. Mesh ventral hernia repairs have lower hernia recurrence rates than do primary repairs. 1 This lower hernia recurrence rate comes at the price of mesh-related complications such as infection, extrusion, and enterocutaneous fistula formation. 2,3
The treatment of infected mesh is a difficult surgical challenge. Removal of the infected mesh is the clearest manner of dealing with the problem. Avoidance of postoperative evisceration and maintenance of a competent abdominal wall are secondary and important goals of treatment of patients with infected mesh.
Rectus abdominis myofascial flap closure of the large midline defect after mesh excision is one potential surgical solution. This procedure, also known as the “separation of parts” hernia repair, has been reported as having low hernia recurrence rates. 4–10 Despite low reported hernia recurrence rates, this procedure does not seem to be frequently or widely used in ventral hernia repair. We reviewed our consecutive series of 11 patients who presented for management of infected mesh after a previous midline ventral hernia repair to illustrate one possible solution to this difficult surgical complication.
METHODS
Surgical Technique
Patients receive a mechanical and antibiotic bowel preparation as an outpatient the day before surgery. A long midline skin incision is made, generously encompassing scar and open wounds. In selected cases of infraumbilical hernias and infected mesh, a panniculectomy incision is used. 11 The incision purposefully straddles the inflammation, and direct dissection of adherent bowel and mesh is avoided. The abdominal cavity is entered above or below any areas of exposed mesh. The medial borders of the rectus muscle are identified, and a dissecting finger along this medial edge is the guide for cautery dissection through subcutaneous tissue, mesh, and abdominal wall scar. This surgical maneuver along both rectus muscles serves to rapidly open the abdomen. All viscera are dissected off the posterior abdominal wall, while the infected mesh, inflamed tissue, and scar located between the rectus muscles will be removed en bloc. In cases with fistula, single bowel loops entering and leaving the inflamed tissue are often easy to isolate, and appropriate bowel work is performed at this time. Any mesh remnants are dissected free and removed to minimize the amount of residual prosthetic material. Mesh removal is easier in cases when it had been used as a “patch” closure to the edges of the rectus than when it had been used as a wide “overlay.”
The resultant defect of the abdominal wall is reconstructed with bilateral rectus abdominis myofascial advancement flaps. The technique employed is a modification of previously described “separation of parts” repairs in its emphasis on the preservation of skin blood flow (Fig. 1). 12 The key to this procedure is to release the external oblique muscle and aponeurosis from its connection to the anterior rectus fascia from above the rib cage to the iliac crest at a level just lateral to the semilunar line. The approach to the semilunar line is either through tunnels created via the midline incision, or else through two laterally placed transverse skin incisions. Skin is bluntly elevated off the semilunar lines bilaterally. Using Deaver retractors for exposure, the external oblique can be released as in a fasciotomy incision. The external oblique is bluntly separated off the internal oblique to allow the muscles to slide relative to each other.
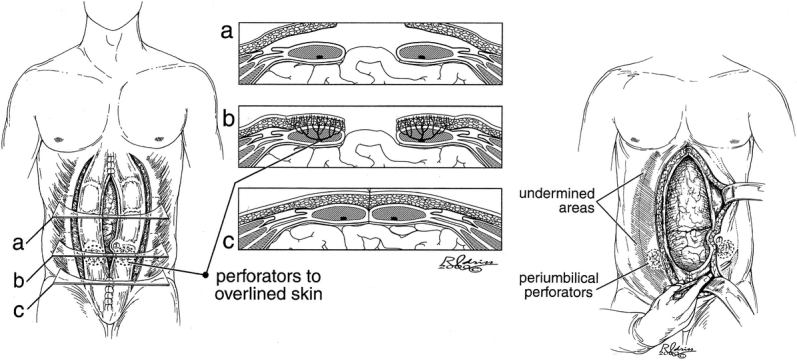
Figure 1. “Separation of parts” procedure with perforator preservation. Reprinted with permission.
The medial rectus muscle and fascia are now debrided of scar. Debridement is complete when the posterior sheath, the rectus muscle edge, and the anterior sheath are clearly visible. No other muscle or fascial release is performed. The fascia is sutured together with interrupted braided nylon figure-of-eight sutures. The medialization of the rectus muscles causes the skin to bunch in the midline. When the procedure is performed correctly, a large amount of medial skin on both wound edges can and should be excised. The skin is closed with dermal absorbable sutures and staples over three drains. One drain is placed along each semilunar line, while the third drain is in the midline. Drains are left in an average of 10 days.
When an overhanging pannus was present and when patients had infraumbilical hernias (four patients), the procedure was performed through a panniculectomy incision. The principle of blunt dissection along the semilunar line with preservation of blood flow between the rectus muscle and skin can likewise be adhered to through this incision.
Mobilization of the patient occurs on the first day. Binders are used for patient comfort only at their request. When bowel function resumes and adequate pain control is achieved, the patient is discharged to home with drains in place without antibiotics (Figs. 2 and 3).

Figure 2. Preoperative view of patient with midline abdominal wound and exposed mesh. A diverting transverse colostomy had been done at an outside hospital for wound control due to a midline colonic fistula through the mesh.

Figure 3. Three-month postoperative view after mesh removal, colostomy takedown, and “separation of parts” hernia repair.
Patient Selection
The patients were referred to a single surgeon (G.A.D.) for management of the abdominal wall. All of the patients had some combination of exposed mesh, enterocutaneous fistula through or around the mesh, and/or chronic drainage. All patients had failed conservative measures by their initial surgeon (e.g., antibiotics, local wound care, and local removal of mesh) before referral.
A retrospective chart review included the surgical history, procedure duration, defect size, length of stay, and postoperative complications, including hernia recurrence and infection. The patients have been followed from 6 to 54 months postoperatively.
RESULTS
Table 1 lists patient demographic data, premorbid conditions, initial surgery, and mesh complication. Three patients presented with mesh extrusion, three presented with enterocutaneous fistula through mesh, and five presented with chronic abscess/infected seroma. Mesh types encountered included both Marlex and Prolene. The interval between previous surgery and the definitive operation ranged from 1 month to 2 years (average 8 months). The defect diameter, as estimated from computed tomography scans, ranged from 8 to 18 cm (average 13 cm). Patient outcomes are presented in Table 2.
Table 1. PATIENT DATA

Table 2. PATIENT OUTCOMES

The follow-up time is currently 6 to 54 months (average 24 months). The one hernia recurrence occurred approximately 1 year after flap hernia repair. Workup consisted of a computed tomography scan showing a small midline hernia sac. The patient was explored and the hernia was closed primarily without the use of mesh; the patient had no further complications at 2 years of follow-up. This same patient was treated for Clostridium difficile colitis at the time of her first surgery.
There were two cases of postoperative stitch abscesses. Small amounts of midline postoperative incision drainage occurred months after the hernia repair. Computed tomography scans did not show a hernia recurrence. Both patients eventually required a surgical exploration and removal of the involved interrupted nylon stitches. The wounds were left open on dressings, and the incisions went on to heal in both patients.
DISCUSSION
The management of chronically exposed or infected mesh after prosthetic repair of incisional hernias has received little focused attention. The definition of the entity is a problem in itself. The patients all had chronic open or draining wounds in association with prosthetic mesh, and all had failed local wound management.
When faced with a mesh extrusion, one must know how and why the mesh was placed. If the mesh was used as an overlay, then local management with mesh excision should not increase the chance for bowel injury, entry into the peritoneum, or a delayed hernia. However, when mesh was used to replace a full-thickness abdominal wall defect, subsequent attempts at local mesh removal expose the patient to all of the above possibilities.
We believe that this study demonstrates the feasibility of a one-step solution to the problem of exposed or infected mesh. The major difference between our technique and previously reported methods of autogenous reconstruction is our focus on the preservation of skin blood flow. Maintenance of skin blood flow in other settings is associated with more reliable wound healing and lower infection rates. 13–15 Our techniques differ in other small aspects from other series of autogenous reconstructions after mesh removal. Though not the focus of the article, Girotto et al. 9 presented seven patients with infected mesh that was removed and reconstructed with sliding rectus flaps. Two patients had postoperative infections. In comparison to Girotto et al., we avoid unilateral releases of the external oblique muscle to ensure muscle balance between the right and left sides of the abdominal wall. Mathes et al. wrote briefly on the utility of the tensor fascia lata flap in cases of removal of infected mesh in a larger series of over 100 abdominal wall reconstructions. 10 We prefer the well-vascularized rectus abdominis muscles to the thinner and less well-vascularized tensor fascia lata. In addition, the tensor fascia lata is difficult to mobilize for supraumbilical defects, and the pedicle turned over at the groin has been known to compress the femoral vein and cause deep venous thrombosis.
A more traditional surgical treatment for infected mesh is mesh removal, bowel work as needed, and placement of a new prosthetic mesh for abdominal wall reconstruction. Placement of permanent mesh in heavily contaminated fields has been found to have infection rates as high as 50% to 90%. 16 Much depends on the quality of the overlying soft tissue. The two stitch abscesses in this series point to the difficulty in working in contaminated fields, and the need to keep foreign material to an absolute minimum.
The increased prevalence of laparoscopic ventral hernia repairs may or may not change the incidence of infected mesh and the ability to deal with the surgical problem. Laparoscopic hernia repairs have lower rates of infection than do open mesh repairs. 17 Series of laparoscopic repairs report impressively low mesh-related complications. 18 However, the laparoscope may not be the ideal instrument for the treatment of infected mesh. Laparoscopic hernia repairs are avoided in purulent cases and require good skin cover over the hernia. Simultaneous bowel surgery for an associated fistula would be difficult with laparoscopic techniques. For these reasons, the laparoscope will not tend to be overly useful in solving the problem of infected mesh.
Footnotes
Correspondence: Dr. Gregory A. Dumanian, Division of Plastic Surgery, 675 N. St. Clair, Suite 19-250, Chicago, IL 60611.
E-mail: gdumania@nmh.org
Accepted for publication August 5, 2002.
References
- 1.Luijendijk RW, Hop WCJ, van den Tol MP, et al. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med. 2000; 343: 392–397. [DOI] [PubMed] [Google Scholar]
- 2.Leber GE, Garb JL, Alexander AI, et al. Long-term complications associated with prosthetic repair of incisional hernias. Arch Surg. 1998; 133: 378–382. [DOI] [PubMed] [Google Scholar]
- 3.White TH, Santos MC, Thompson JS. Factors affecting wound complications associated with prosthetic repair of incisional hernias. Am Surg. 1998; 133: 378–382. [Google Scholar]
- 4.Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990; 86: 519–525. [DOI] [PubMed] [Google Scholar]
- 5.Saulis AS, Dumanian GA. Periumbilical rectus abdominis perforator preservation significantly reduces superficial wound complications in “separation of parts” hernia repairs. Plast Reconstr Surg. 2002; 109: 2275–2280. [DOI] [PubMed] [Google Scholar]
- 6.Fabian TC, Croce MA, Pritchard FE, et al. Planned ventral hernia. Staged management for acute abdominal wall defects. Ann Surg. 1994; 219: 643–649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dibello JN, Moore JH. Sliding myofascial flap of the rectus abdominus muscles for the closure of recurrent ventral hernias. Plast Reconstr Surg. 1996; 98: 464–469. [DOI] [PubMed] [Google Scholar]
- 8.Lucas CE, Ledgerwood AM. Autologous closure of giant abdominal wall defects. Am Surg. 1998; 64: 607–610. [PubMed] [Google Scholar]
- 9.Girotto JA, Redett R, Muehberger T, et al. Closure of chronic abdominal wall defects: a long-term evaluation of the components separation method. Ann Plast Surg. 1999; 42: 385–395. [DOI] [PubMed] [Google Scholar]
- 10.Mathes SJ, Steinwald PM, Foster RD, et al. Complex abdominal wall reconstruction: a comparison of flap and mesh closure. Ann Surg. 2000; 232: 586–594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kohorn EI. Panniculectomy as an integral part of pelvic operation is an underutilized technique in patients with morbid obesity. J Am Coll Surg. 1995; 180: 279–285. [PubMed] [Google Scholar]
- 12.Sukkar SM, Dumanian GA, Szczerba SM, et al. Challenging abdominal wall defects. Am J Surg. 2001; 181: 115–121. [DOI] [PubMed] [Google Scholar]
- 13.Gibbons GW, Wheelock FC, Hoar CS, et al. Predicting success of forefoot amputations in diabetics by noninvasive testing. Arch Surg. 1979; 114: 1034–1037. [DOI] [PubMed] [Google Scholar]
- 14.Feng LF, Price D, Hohn D, et al. Blood flow changes and leukocyte mobilization in infection: A comparison between ischemic and well-perfused skin. Surg Forum. 1983; 34: 603–604. [Google Scholar]
- 15.Chang N, Mathes SJ. Comparison of the effect of bacterial inoculation on musculocutaneous and random pattern flaps. Plast Reconstr Surg. 1982; 70: 1–10. [DOI] [PubMed] [Google Scholar]
- 16.Dayton MT, Buchele BA, Shirazi SS, et al. Use of an absorbable mesh to repair contaminated abdominal wall defects. Arch Surg. 1986; 121: 954–690. [DOI] [PubMed] [Google Scholar]
- 17.Ramshaw BJ, Esartia P, Schwab J, et al. Comparison of laparoscopic and open ventral herniorrhaphy. Am Surg. 1999; 65: 827–832. [PubMed] [Google Scholar]
- 18.Heniford BT, Park A, Ramshaw BJ, et al. Laparoscopic ventral and incisional hernia repair in 407 patients. J Am Coll Surg. 2000; 190: 645–650. [DOI] [PubMed] [Google Scholar]