

Abstract
A 49-year-old woman with a 2-year history of severe dysphagia, claudication of the right arm, and persistent pulsatile back pain presented at our institution. An esophagogram showed 2 marked indentations of the upper esophagus. Computed axial tomography showed a right-sided aortic arch with mirror image branching and an aortic diverticulum; the thoracic aorta distal to the origin of the right subclavian artery was elongated and tortuous, ascending to the base of the neck to form the “2nd arch,” which compressed the right-arm plexus nerve and the upper vertebral column. Through a right thoracotomy, a segment of thoracic aorta around the Kommerell's diverticulum was resected, and the proximal and distal ends of the thoracic aorta were reapproximated. The patient tolerated the procedure well and remained symptom free.
Key words: Aorta; thoracic/abnormalities/surgery; deglutition disorders/etiology; esophageal stenosis/congenital/diagnosis/surgery; heart defects, congenital; tomography, x-ray computed
Right aortic arch is an uncommon anatomic anomaly, which occurs in approximately 0.05% to 0.1% of the population.1 “Mirror-image” right aortic arch is by itself generally asymptomatic, but it is usually associated with cyanotic congenital heart disease.2 In the event that a mirror-image right aortic arch is associated with a retroesophageal left ligamentum arteriosum, there is a vascular ring3 formed anteriorly by the ascending portion of the right aortic arch and the innominate artery, posteriorly by the aortic diverticulum, and laterally by the ligamentum arteriosum. This anomaly is rare, but it may be symptomatic.2–7 We report the case of a patient who was having difficulty swallowing and persistent pulsatile upper-back pain. She had a mirror-image right aortic arch with a retroesophageal left ligamentum arteriosum, and with elongation and tortuosity of the descending thoracic aorta.
Case Report
In May 2003, a 49-year-old, otherwise-healthy woman with a 2-year history of severe dysphagia, claudication of the right arm, and persistent pulsatile back pain was referred to our hospital. Her dysphagia had progressed to the point that she was unable to swallow solid food. To lessen her back pain, she always straightened her back. Her blood pressure was 120/80 mmHg in both arms, and her heart rate was 85 beats/min. A pulsatile mass could be palpated over the sternal notch.
An esophagogram showed 2 marked indentations of the esophagus: one at the T3 level, opposite the aortic arch; and the other one, 6 cm lower, at the level of a Kommerell's diverticulum (Fig. 1A). Computed axial tomography demonstrated a right-sided aortic arch with mirror-image branching and right descending thoracic aorta (Fig. 2A). The Kommerell's diverticulum was clearly demonstrated (Fig. 2B). The aorta was seen at a very high level, even higher than the sternocleidal joints (Fig. 3).
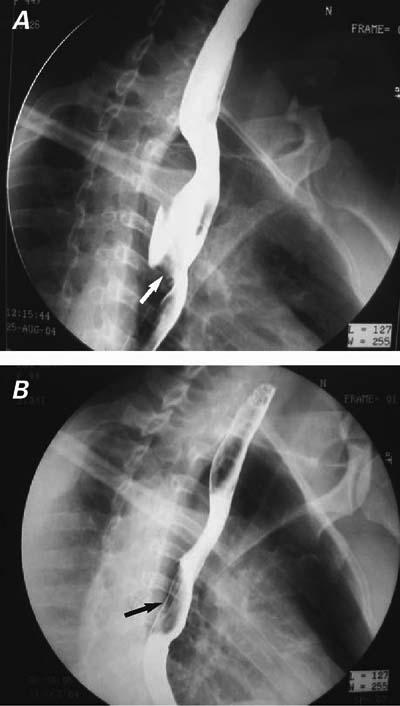
Fig. 1 Esophagograms. A) Note the 2 deep indentations on the esophagus. The upper one was at the T3 level, just opposite the 2nd aortic arch; the lower one (arrow), at the T6 level, was consistent with the course of the Kommerell's diverticulum. B) Postoperatively, the lower indentation has disappeared, and the upper one (arrow) is shallow.
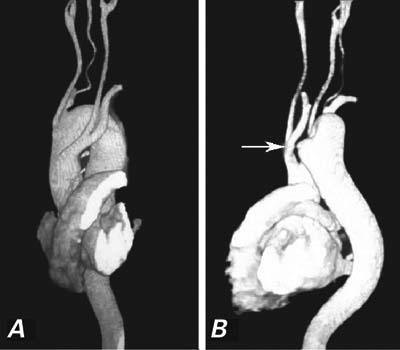
Fig. 2 Computed axial tomography. A) The right-sided aortic arch shows mirror-image branching, and the thoracic aorta descends on the right side. B) The Kommerell's diverticulum is clearly demonstrated (arrow).

Fig. 3 This computed tomographic scan shows that the aortic arch (arrow) is much higher than the sternocleidal joints.
Due to the persistence and worsening of the patient's symptoms, surgery was recommended.
Surgical Technique
The patient, under general anesthesia, was placed in the left lateral decubitus position. A right thoracotomy was performed through the 4th intercostal space. The right phrenic nerve and the superior vena cava were retracted anteriorly. The right vagus nerve descended at the anterior portion of the distal aortic arch. The 1st aortic branch was the left innominate artery, the 2nd was the right carotid artery, and the 3rd was the right subclavian artery. Distal to the origin of the right subclavian artery, the aorta—ascending to the neck at the C7 level, then descending along the vertebra—formed a “2nd” arch. It was clear that the 2nd arch compressed the upper thoracic vertebral column (C7, T1, and T2), the radicular nerve, and the esophagus. A Kommerell's diverticulum was found to take off from the left side of the thoracic aorta at the T6 level and to travel to the left behind the esophagus, pulling the thoracic aorta toward the left to compress the esophagus from the left rear. The diverticulum was about 5 cm in length, ending as a thick, cord-like, fibrous tissue.
After systemic heparinization, a temporary, 24F shunt was established between the ascending aorta and the thoracic aorta, 5 cm distal to the Kommerell's diverticulum. The aorta was cross-clamped just distal to the right subclavian artery and proximal to the distal end of the shunt. A segment of descending aorta (6 cm) that included the Kommerell's diverticulum was resected. The proximal and distal ends of the descending aorta were reapproximated directly, with no tension. The 2nd arch disappeared and the descending aorta was far from the brachial plexus, the upper segment of the thoracic vertebral column, and the esophagus. Because the cross-clamp time was 15 minutes and a temporary shunt was used, we undertook no additional protection of the spinal cord. Blood-product transfusion was unnecessary, because the total amount of blood loss was about 400 mL. After surgery, the patient remained intubated for 4 hours and stayed in the intensive care unit for 16 hours.
Postoperatively, the patient recovered uneventfully. There was no vocal nerve paralysis. She swallowed solid food without symptoms of dysphagia. A postoperative esophagogram showed 1 shallow indentation of the esophagus at the left side (Fig. 1B). The back pain and claudication of the right arm disappeared. She was discharged home on postoperative day 8. Three years later, she remained symptom free.
Discussion
Right aortic arch has been previously classified into 5 types.8 The patient presented here apparently had a type B right aortic arch (Fig. 4). Although she had severe dysphagia and the esophagogram showed 2 indentations of the esophagus, we failed preoperatively to find a complete vascular ring by imaging techniques. During surgery, we found that the upper indentation was due to compression by the tortuous 2nd arch, and the lower indentation due to compression by the Kommerell's diverticulum. The diverticulum passed behind the esophagus and pulled the thoracic aorta toward the left. The esophagus was compressed toward the left anteriorly.
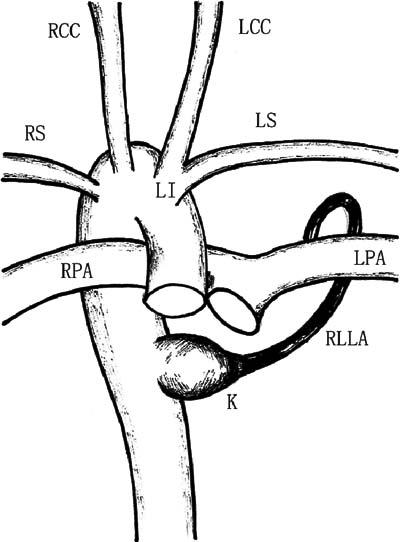
Fig. 4 Diagram of the anomaly. The vascular ring is formed by the ascending aorta, left pulmonary artery (LPA), right pulmonary artery (RPA), Kommerell's diverticulum (K), and retroesophageal left ligamentum arteriosum (RLLA).
LCC = left common carotid artery; LI = left innominate artery; LS = left subclavian artery; RCC = right common carotid artery; RS = right subclavian artery
This is a very unusual anomaly. The true Kommerell's diverticulum in the situation of right aortic arch represents the remnant of a left dorsal aorta.7 Here the interruption of the left arch is upstream of the ductus arteriosus. The left-sided ligamentum arteriosum extends from the Kommerell's diverticulum on the upper descending thoracic aorta, behind the esophagus, and forward to the left pulmonary artery, forming a vascular ring.4 The posterior left portion of the vascular ring is not a vessel, but an atretic ductus arteriosus—the ligamentum arteriosum. In this situation, imaging cannot demonstrate a complete vascular ring, because the ligamentum arteriosum cannot be shown by any imaging technique. In any patient with dysphagia who has a right aortic arch, a complete vascular ring—consisting anteriorly of the ascending portion of the right aortic arch and innominate artery, posteriorly of the aortic diverticulum, and laterally of the ligamentum arteriosum—should be suspected, and operation is recommended.
Elongation and tortuosity of the thoracic aorta related to right aortic arch with retroesophageal left ligamentum arteriosum are even rarer. Degrees of tracheoesophageal symptoms associated with right aortic arch have been well reported, but very few reports have described back pain and claudication of the right arm in the presence of a right aortic arch. In this patient, surgical exploration seemed to indicate that the back pain and claudication of the right arm were due to compression of the plexus nerve and the upper vertebral column by the 2nd arch.
Because our patient's symptoms were multiple, the operation was designed carefully to achieve decompression of the upper vertebral column and the brachial plexus and division of the vascular ring. A segment of thoracic aorta (about 6 cm) around the aortic diverticulum was resected, and the proximal and distal ends of the aorta were anastomosed directly, so that the thoracic aorta would be at considerable distance from the vertebral column and the brachial plexus. Because Kommerell's diverticulum is the key portion of the vascular ring, it was included in the resected segment of thoracic aorta.
Right thoracotomy is the preferred approach for this lesion, because it gives excellent exposure of the ascending aorta through to the descending aorta.
Footnotes
Address for reprints: Jinping Zhao, MD, Department of Cardiothoracic Surgery, Tongji Hospital, 430030 Wuhan, PRC. E-mail: jpzhao@tjh.tjmu.edu.cn
References
- 1.Cina CS, Althani H, Pasenau J, Abouzahr L. Kommerell's diverticulum and right-sided aortic arch: a cohort study and review of the literature. J Vasc Surg 2004;39:131–9. [DOI] [PubMed]
- 2.Cina CS, Arena GO, Bruin G, Clase CM. Kommerell's diverticulum and aneurysmal right-sided aortic arch: a case report and review of the literature. J Vasc Surg 2000;32:1208–14. [DOI] [PubMed]
- 3.Han JJ, Sohn S, Kim HS, Won TH, Ahn JH. A vascular ring: right aortic arch and descending aorta with left ductus arteriosus. Ann Thorac Surg 2001;71:729–31. [DOI] [PubMed]
- 4.Zachary CH, Myers JL, Eggli KD. Vascular ring due to right aortic arch with mirror-image branching and left ligamentum arteriosus: complete preoperative diagnosis by magnetic resonance imaging. Pediatr Cardiol 2001;22:71–3. [DOI] [PubMed]
- 5.Schlesinger AE, Mendeloff E, Sharkey AM, Spray TL. MR of right aortic arch with mirror-image branching and a left ligamentum arteriosum: an unusual cause of a vascular ring. Pediatr Radiol 1995;25:455–7. [DOI] [PubMed]
- 6.Garti IJ, Aygen MM, Vidne B, Levy MJ. Right aortic arch with mirror-image branching causing vascular ring. A new classification of the right aortic arch patterns. Br J Radiol 1973;46:115–9. [DOI] [PubMed]
- 7.Pocar M, Moneta A, Villa E, Donatelli F. Regarding “Kommerell's diverticulum and right-sided aortic arch: a cohort study and review of the literature”. J Vasc Surg 2004;39:1361. [DOI] [PubMed]
- 8.Kirklin JW, Barratt-Boyes BG. Cardiac surgery: morphology, diagnostic criteria, natural history, techniques, results, and indications. New York: Wiley; 1986. p. 1111–28.