

71-year-old woman with sick sinus syndrome and Mobitz Type II atrioventricular block underwent implantation of a DDDR pacemaker (Integrity™ μ DR; St. Jude Medical, Inc.; St. Paul, Minn). The leads were inserted through a percutaneous puncture of the left subclavian vein with use of standard techniques. Both leads were active fixation leads. A predischarge pacemaker check showed normal pacing and sensing thresholds for both leads.
The patient returned about a month later with recurrent dizziness and fatigue. Examination of the pacemaker revealed atrial lead undersensing and noncapture, with a lead impedance of more than 2500 ohms. The ventricular lead was normal. A chest radiograph showed an obvious coil fracture of the atrial lead (Fig. 1), and the ventricular lead also appeared damaged. The patient was taken to the electrophysiology suite, and the leads were removed without difficulty. Examination of the explanted leads revealed advanced coil fracture in the atrial lead and a break in the insulation with some coil damage in the ventricular lead (Fig. 2).
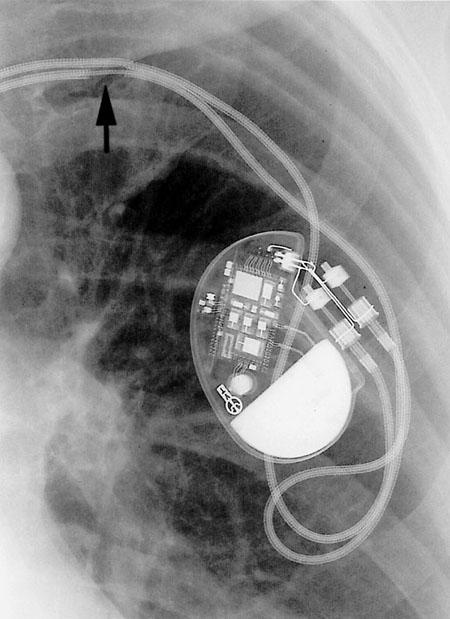
Fig. 1 A chest radiograph shows an obvious coil fracture of the atrial lead (arrow), and the ventricular lead also appears damaged.
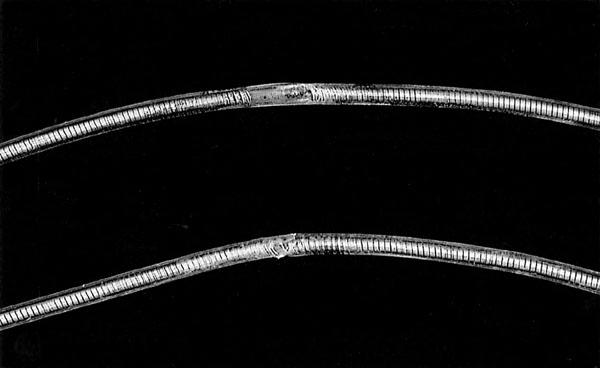
Fig. 2 The explanted leads show evidence of advanced coil fracture in the atrial lead (top) and a break in the insulation with some coil damage in the ventricular lead (bottom).
Comment
Conductor fracture and insulation breaks occur infrequently but are not rare. 1 In their study of 49 explanted compression-damaged leads, Jacobs and colleagues 2 found that all of the leads had been placed by conventional percutaneous subclavian puncture. Meticulous anatomic studies on cadavers 2–4 have shown that leads inserted by standard techniques usually pass through the medial subclavicular musculotendinous complex (MSMC) before entering the vein. The MSMC comprises the subclavius muscle, the costoclavicular ligament, and the costocoracoid ligament. Magney and coworkers 4 dissected consecutive cadavers with pacemakers, defibrillators, and central venous catheters. As a result of their research, they reported a database of 23 leads or catheters, placed by percutaneous subclavian puncture, 22 of which passed through the MSMC. Using these cadaver models, the authors further demonstrated that leads trapped in the MSMC are exposed to unnecessary stress as they move with the clavicle. Their study also showed that the above phenomenon, rather than contact with the bony structures (or friction), was the primary mechanism of lead damage. 4 Our patient had gone hiking and mountain climbing 3 weeks after pacemaker implantation (although she had been advised against it). These activities may have aggravated the mechanical stress on the leads.
It has been suggested that the use of cephalic vein cutdown or a more lateral percutaneous entry into the subclavian or axillary vein would nearly eliminate lead compression or “crush” injury. 5 In our patient, we implanted new leads using a more lateral percutaneous access to the left subclavian vein.
Footnotes
Address for reprints: Ali Massumi, MD, 6624 Fannin St., Suite 2480, Houston, TX 77030
E-mail: Hallgar@hgcardio.com
References
- 1.Kazama S, Nishiyama K, Machii M, Tanaka K, Amano T, Nomura T, et al. Long-term follow up of ventricular endocardial pacing leads. Complications, electrical performance, and longevity of 561 right ventricular leads. Jpn Heart J 1993;34:193–200. [DOI] [PubMed]
- 2.Jacobs DM, Fink AS, Miller RP, Anderson WR, McVenes RD, Lessar JF, et al. Anatomical and morphological evaluation of pacemaker lead compression. Pacing Clin Electrophysiol 1993;16(3 Pt 1):434–44. [DOI] [PubMed]
- 3.Magney JE, Flynn DM, Parsons JA, Staplin DH, Chin-Purcell MV, Milstein S, Hunter DW. Anatomical mechanisms explaining damage to pacemaker leads, defibrillator leads, and failure of central venous catheters adjacent to the sternoclavicular joint. Pacing Clin Electrophysiol 1993;16(3 Pt 1):445–57. [DOI] [PubMed]
- 4.Magney JE, Parsons JA, Flynn DM, Hunter DW. Pacemaker and defibrillator lead entrapment: case studies. Pacing Clin Electrophysiol 1995;18(8):1509–17. [DOI] [PubMed]
- 5.Magney JE, Staplin DH, Flynn DM, Hunter DW. A new approach to percutaneous subclavian venipuncture to avoid lead fracture or central venous catheter occlusion. Pacing Clin Electrophysiol 1993;16(11):2133–42. [DOI] [PubMed]