

Abstract
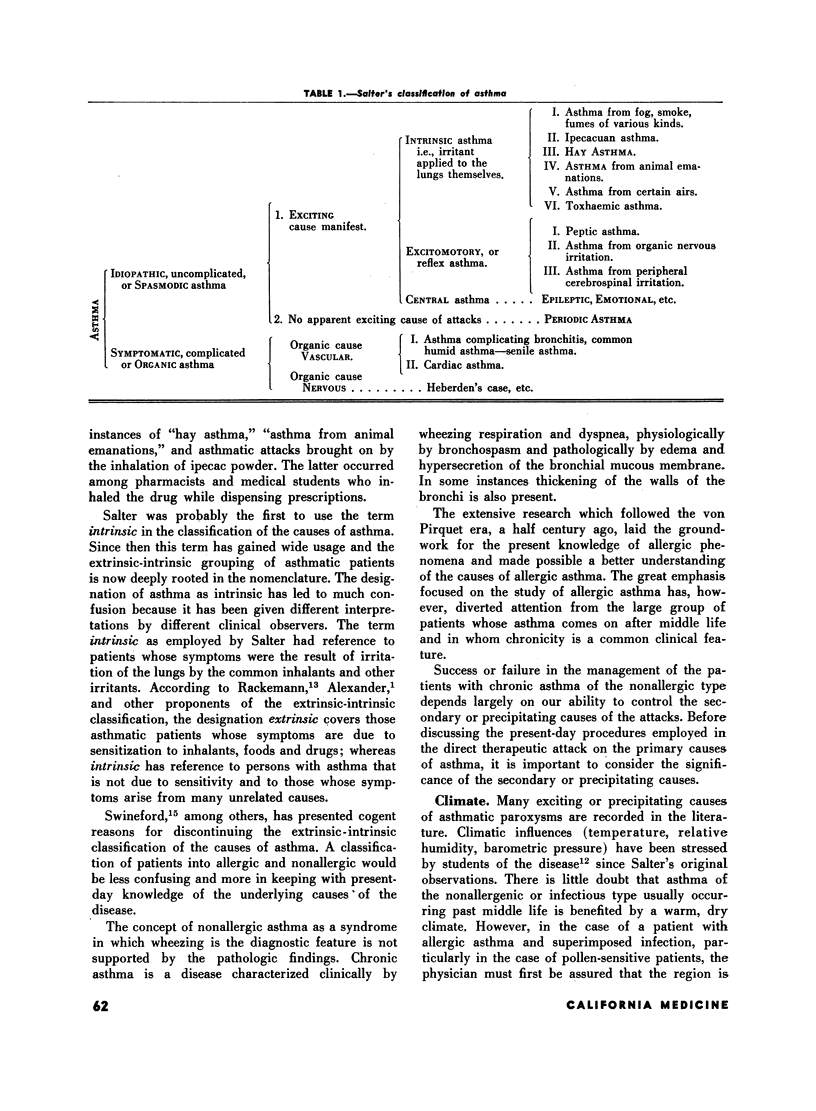
A classification of asthma into allergic and nonallergic has gained support from the more recent studies on the underlying causes of the disease.
The majority of instances of nonallergic asthma occur after middle life and result from recurrent infections of the upper and lower respiratory tract. Status asthmaticus is a frequent complication of infectious asthma.
Chronic and intractable asthma may be present also in a patient with allergic asthma complicated by a superimposed infection of the sinuses, bronchi and lungs.
There are many secondary or precipitating causes that may bring on asthmatic paroxysms. The most important of these are acute respiratory infections, mechanical and chemical irritants, autonomic imbalance, hormonal deficiencies and psychogenic influences. These secondary causes play a more important role in nonallergic asthma because of the greater tendency to chronicity in this form of the disease.
The effective treatment of chronic asthma depends largely on the successful control of the secondary or precipitating causes of the asthmatic attacks.
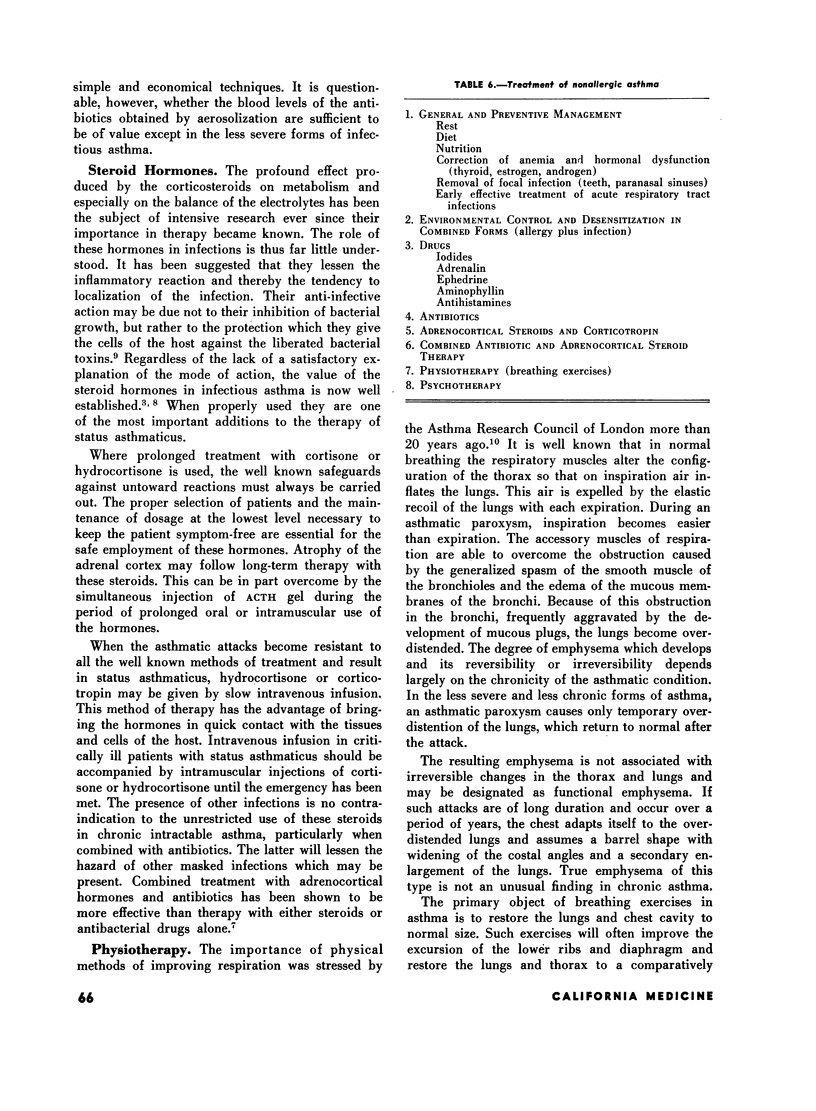
The introduction of the antibiotics and corticosteroids in the treatment of infectious asthma has supplied potent weapons to combat the disease. The use of these therapeutic agents makes possible the control of two of the important pathologic lesions of asthma—bronchial infection and bronchial inflammation.
At present combined antibiotic and cortisone or hydrocortisone therapy of asthma seems to be the most rational method of preventing the disease from becoming chronic and intractable. Their value in infectious asthma is due to their anti-infective and antiflammatory action.
When prolonged treatment is essential, combined therapy also lessens the dangers arising from the presence of masked infections.
Full text
PDF




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BALDWIN H. S., DEGARA P. F., SPIELMAN A. D., DWORETZKY M. ACTH and cortisone in the treatment of asthma. J Allergy. 1955 Jan;26(1):44–53. doi: 10.1016/0021-8707(55)90106-4. [DOI] [PubMed] [Google Scholar]
- FINKE W. Combined antibiotic-cortisone therapy in infectious asthma; the rationale of its early application. N Y State J Med. 1954 Oct 1;54(19):2685–2692. [PubMed] [Google Scholar]
- GELFAND H. H. Prolonged ambulatory use of cortisone and ACTH for bronchial asthma and other allergies. J Allergy. 1953 Nov;24(6):510–521. doi: 10.1016/0021-8707(53)90026-4. [DOI] [PubMed] [Google Scholar]
- SWINEFORD O., Jr Asthma: classification of causes; a recommended classification and a critical review. J Allergy. 1954 Mar;25(2):151–167. doi: 10.1016/0021-8707(54)90154-9. [DOI] [PubMed] [Google Scholar]