

Abstract
Background
International medical graduates are an important component of the Canadian physician workforce. For most international medical graduates, the principal route to obtaining a residency position in Canada is to apply through the second iteration of the Canadian Resident Matching Service (CaRMS) match. In order to help inform the work toward integrating unlicensed international medical graduates into Canada's health professional workforce, our objectives were to describe the demographic and educational characteristics of international medical graduate CaRMS applicants and identify their preferred clinical disciplines and practice locations.
Methods
A 37-item Web-based questionnaire survey was offered to all 659 international medical graduate second-iteration CaRMS 2002 applicants. We collected data on their demographic and educational background and preferred clinical discipline and practice location. Up to 2 follow-up email reminders were sent to nonrespondents.
Results
The survey response rate was 70.3% (463/659). Of the respondents, 71.9% had obtained their medical degree in Asia, the Middle East or Eastern Europe: 36.5% had graduated with a medical degree since 1994, and 17.3% since 1997. Most respondents (74.3%) were aged between 30 and 44 years. More than half (54.6%) had completed their medical education in English. Most (69.3%) had done postgraduate training outside Canada. Before coming to Canada, 42.8% had practised medicine for 1–5 years and 45.6% had practised for 6–20 years. The top 5 choices of clinical discipline in Canada were family medicine/general practice (45.6%), internal medicine (14.9%), surgery (7.3%), obstetrics/gynecology (6.7%) and pediatrics (4.8%). Of those who resided in the 4 Western provinces or Nova Scotia, between 76.8% and 86.7% preferred to stay in their own province, and 60%, 51.4% and 37% of those who resided in Newfoundland, Ontario or Quebec respectively preferred to practise in their own province.
Interpretation
Second-iteration international medical graduate CaRMS applicants are a heterogeneous group of physicians, some with substantial medical training and experience and others at an earlier stage of their medical career.
International medical graduates (IMGs), or physicians who graduated from medical schools outside Canada, constitute 23% of licensed Canadian physicians.1,2,3,4,5 Although the exact number of unlicensed IMGs in Canada is unknown,6,7 the Association of International Physicians and Surgeons of Ontario (AIPSO), which has a membership of 1100 unlicensed IMGs, estimates the actual number in Ontario to be 2000–4000.8 It has been estimated that at least 400 unlicensed IMGs were residing in British Columbia in 20019 and 160 in Alberta.10
Although some IMGs are able to obtain professional work after settling in Canada, many face challenges in establishing their medical practice.7,10,11,12 Different perspectives and values contribute to tension in the discussion of IMG workforce issues.13 There is a need to better understand the contribution that IMGs can make to Canadian medicine.
A survey of IMGs who applied to the second iteration of the Canadian Resident Matching Service (CaRMS) match provided an opportunity to learn about this subgroup of IMGs. In order to help inform the work toward integrating unlicensed IMGs into Canada's health professional workforce, our objectives were to describe the demographic and educational characteristics of IMG CaRMS applicants and identify their preferred clinical disciplines and practice location.
Methods
CaRMS matches applicants who are interested in starting postgraduate year (PGY) 1 medical training in 1 of the 13 English-speaking medical schools in Canada with programs wishing to enroll trainees. Eligible applicants are current or previous graduates from Canadian- or US-accredited medical schools and IMGs who have passed the Medical Council of Canada Evaluating Examination within 5 years of the start date of residency training.14 CaRMS defines IMGs as graduates of a World Health Organization–listed medical school, and not from a Canadian- or US-accredited medical school.15 The first iteration of the match is primarily for medical students graduating from Canadian medical schools in the year of the match, whereas the second iteration is for graduates unmatched in the first match, graduates from previous years and eligible IMGs.16
A Web-based questionnaire was developed for IMGs registered in the second iteration of the CaRMS 2002 match. The questionnaire, in paper format, was piloted with 4 IMGs enrolled in the Alberta IMG Program and took 15 minutes to complete. In addition to demographic data and immigration information, the survey inquired about medical training and practice outside Canada, medical training in Canada, attempts to obtain a medical licence and a residency position in Canada, strategies used to keep abreast of current medical knowledge, type of practice desired in Canada, self-rated preparedness for training and practice, and perceived barriers and opportunities in assessment, training and practice. Only the demographic and educational data and preferred practice location and clinical discipline are presented here.
The questionnaire was posted on the CaRMS Web site during the 4-week period immediately before the second iteration of the 2002 match, because we did not want the applicants to perceive that their responses would in any way compromise their opportunities through the match. The response data were released to the investigators after the results of the match were announced.
IMG registrants were invited to participate in the survey via a notice on the CaRMS Web site. Those wishing to complete the survey could access it using their CaRMS identification number. They were asked to answer the survey only once and to leave any questions blank that they did not wish to answer. One or 2 follow-up email messages were sent to nonrespondents encouraging them to participate in the survey. Before data analysis, a search was undertaken for duplicate responses. Of the 47 duplicate surveys, only the last completed survey was analyzed. In each case, the previous survey or surveys were incomplete or blank, possibly indicating difficulty with the electronic survey submission process. Then, the CaRMS identification number was removed from the responses and replaced by an arbitrary numeric code to maintain confidentiality.
Descriptive data analysis included frequency distributions and percentages.
The study received ethics approval from the Conjoint Health Research Ethics Board, University of Calgary, and the Health Research Ethics Board, University of Alberta, Edmonton.
Results
Of the 659 IMG CaRMS registrants who were invited to participate in the survey, 463 (70.3%) responded. The demographic characteristics of the respondents (Table 1) indicate that 74.3% of the respondents were 30–44 years of age, 52.1% were male and 54.6% resided in Ontario. As shown in Fig. 1, 80.6% lived in a community with a population of over 100 000. Of the respondents, 60.7% immigrated to Canada during the period 1996–2000, and 95.9% of respondents rated themselves as proficient in English and 24.6% in French.
Table 1
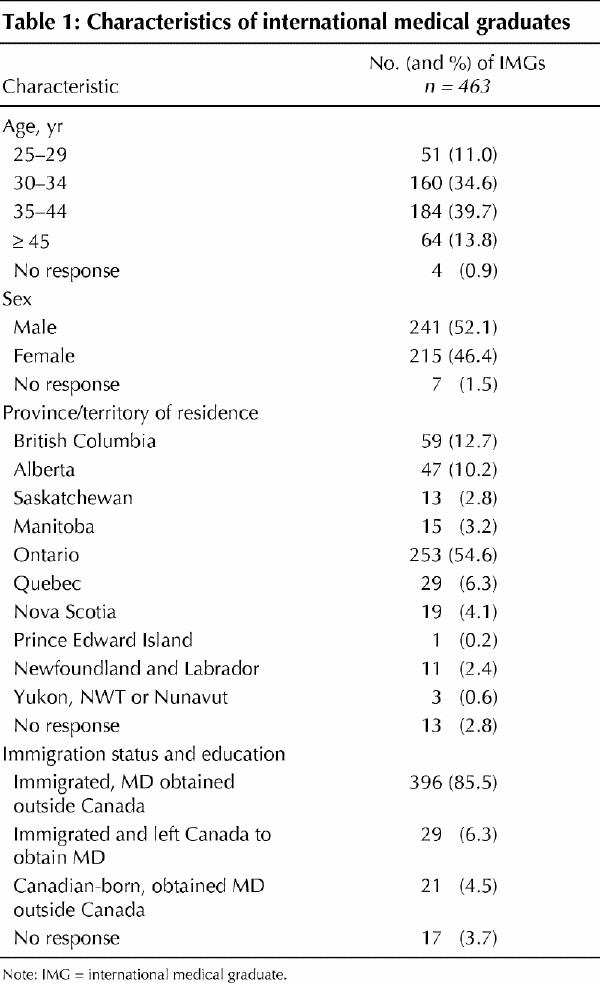
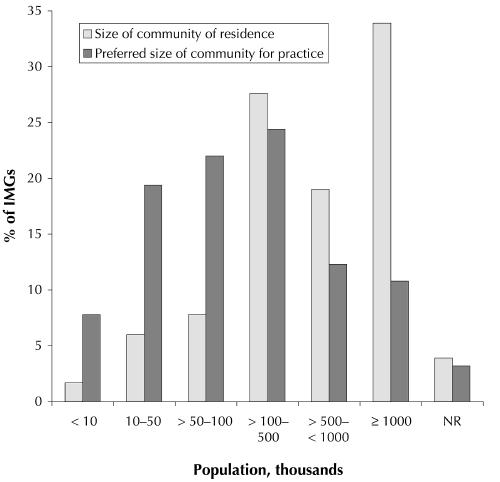
Fig. 1: Size of community of residence and preferred size of community for practice. IMG = international medical graduate, NR = no response.
Although most IMGs obtained their medical degree before coming to Canada, 6.3% immigrated and subsequently left Canada to do their medical studies and 4.5% were Canadian-born IMGs (Table 1). For 71.9% of the respondents, their medical degree was obtained from Asian, Middle Eastern or Eastern European countries (Table 2). It was reported that 36.5% had obtained their undergraduate medical degree since 1994, and 17.3% since 1997. Of the respondents, 54.6% had completed their medical training in English.
Table 2
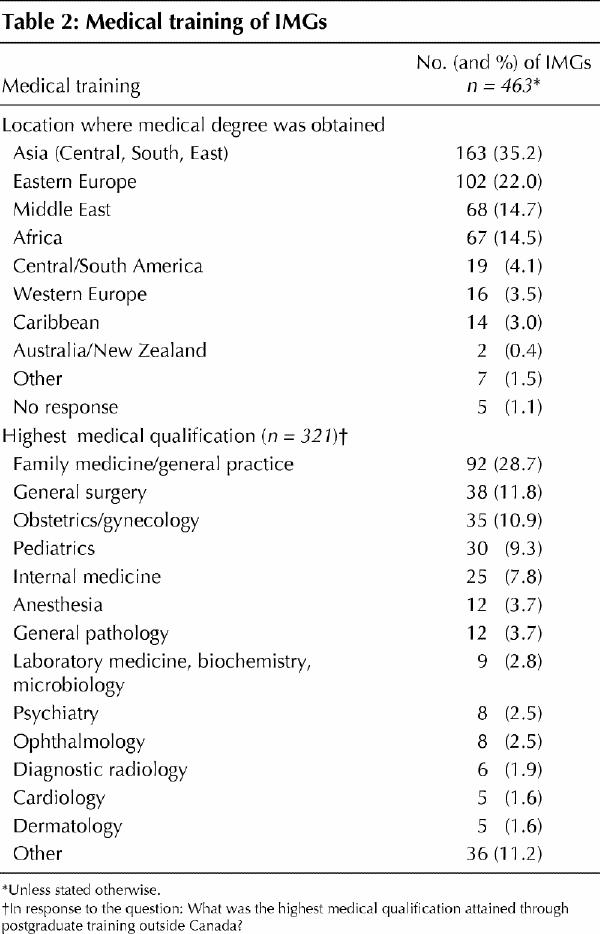
A rotating internship (not necessarily post-MD degree) was completed outside Canada by 86.4% of the respondents; 69.3% of the respondents had completed at least some postgraduate medical training, and 54.4% had obtained a postgraduate certificate or diploma. The highest qualifications attained outside Canada were most frequently in the disciplines of family medicine/general practice, general surgery or obstetrics/gynecology. It was reported that 60.5% of all the respondents had 1–5 years of postgraduate training, 42.8% had practised medicine for 1–5 years and 45.6% had practised for 6–20 years before coming to Canada.
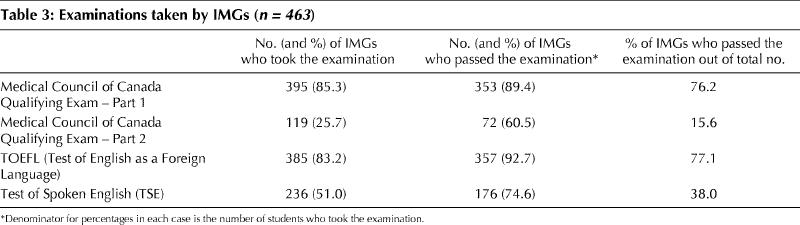
The majority wrote and passed the Medical Council of Canada Qualifying Examination – Part 1 (76.2%), and a minority (15.6%) wrote and passed Part 2 (Table 3). At the time of our study, 14.9% of respondents reported that they were registered in a formal clinical training program in Canada and 7.8% held an active Canadian medical licence.
Table 3
Of the respondents, 67.4% were applying to CaRMs for the first time in 2002, and 34.3% had applied 2 or more times in the past. The first choice of clinical discipline for residency training was family medicine (45.6%) followed by internal medicine (14.9%) (Table 4).
Table 4
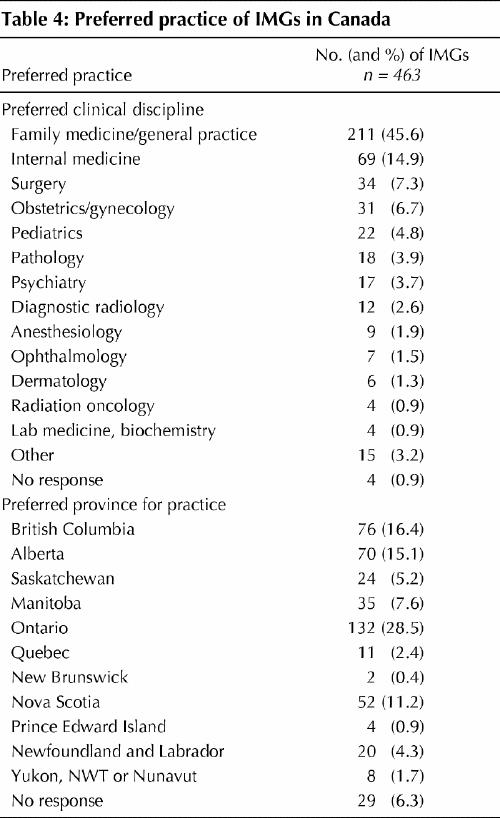
Of those who resided in the 4 Western provinces or Nova Scotia, between 76.8% and 86.7% preferred to stay in their own province, whereas 60%, 51.4% and 37% of those who resided in Newfoundland, Ontario or Quebec, respectively, preferred to practise in their own province.
Of the respondents, 47.5% expressed a preference to practise in a community with a population of over 100 000, and 7.8% preferred a community with a population of less than 10 000 (Fig. 1). A comparison of community size of residence with preferred community size of practice revealed that a substantial proportion (between 42.9% and 72.2%) of those who lived in communities with a population of over 50 000 would actually prefer to practise in smaller communities than those in which they lived. Of those who indicated family medicine as a first choice of clinical discipline, 40.6% preferred to practise in communities with a population of 50 000 or less compared with 17.8% of those who indicated other disciplines.
Interpretation
We studied a subset of IMGs who were actively seeking postgraduate opportunities through CaRMS and identified their educational background, skills and aspirations. The respondents had varied training experience in the practice of medicine. Almost half (228, 49.2%) indicated that their preferred practice location would be in communities with a population of less than 100 000, with 36 (7.8%) preferring rural communities with a population of less than 10 000. Just under half (211, 45.6%) identified family medicine/ general practice as their first choice of discipline.
Of the 659 IMGs in Canada registered for the second iteration of the CaRMS 2002 match, 496 (75.3%) submitted a rank order list for training positions left vacant from the first iteration and 463 (70.3%) participated in the survey. We note that, for several reasons, not everyone who registers with the match chooses to participate. Only those who submit a rank order list can be considered for matching. Based on the 659 IMGs registered for the match and the 496 who submitted a rank order list, we estimate that the number of IMGs ready or prepared to undertake postgraduate training in order to achieve licensure and practice in Canada appears to be in the range of 500–600. Only 83 (16.7%) of the 496 applicants were successful in obtaining a residency position through the second iteration of the 2002 match. It is difficult to know how many would have been successful if more positions and more choices were available.
Opportunities for IMGs to access postgraduate training arise from surplus positions at the PGY-1 level. The number of positions at the PGY-1 entry level is set by the province and is coordinated to meet the needs of the graduating class of the province. Each year as many as 50 students opt to begin postgraduate training in the United States. In addition, some students do not graduate as anticipated, and others choose to delay beginning postgraduate training. The net result of these changes is a surplus of positions at the PGY-1 level. In the 2002 PGY-1 match, there were 53 positions vacant after the second iteration.16 Twenty-one (39.6%) of the second iteration vacancies were in Ontario programs and were not available to IMG applicants, because they are not eligible to apply for second iteration positions in Ontario. An additional 4 (7.5%) were in Quebec, which restricts access to positions in the second iteration to graduates of Canadian medical schools. The remaining positions were in Newfoundland (14, 26.4%), Manitoba (13, 24.5%) and BC (1, 1.9%).
The countries in which the IMG respondents did their medical training tend to be those that are the source of many recent immigrants to Canada.17 Although there is some discussion in the literature about the pros and cons of “culture-matching” between physicians and patients,18 some ethnic communities may be better served by physicians of similar ethnic backgrounds.4,19,20 IMGs bring a rich mix of cultures, skills and attitudes to medicine21 that can benefit both patients and the medical community. Given current physician shortages in Canada and the increasing diversity of the Canadian population, integrating the skills and potential of unlicensed IMGs currently residing in Canada within the context of pan-Canadian workforce planning would appear to make sense.
Our findings should be interpreted within the context of the study limitations. The Web version of the questionnaire was not validated, and the reliability of the self- reported data provided by the IMGs in the questionnaire survey is unknown. In order to influence policy, collusion among IMG respondents is possible, although we believe highly unlikely. In addition, the respondents may have had linguistic difficulties in understanding some of the questions. Given that anonymity was assured during data analysis, the characteristics of the nonrespondents are unknown. Although it is likely that the respondents are representative of all IMG CaRMS applicants, it is unlikely that they are representative of all IMGs in Canada. IMG CaRMS applicants are a highly select and motivated subgroup of IMGs who have been able to fulfill all the necessary requirements in order to apply for a residency training position in Canada.
This study was designed as a first step in describing IMGs in Canada. Much remains to be learned. Attempting to quantify the number of unlicensed IMGs in Canada, and the number who might eventually meet licensure requirements through appropriate postgraduate training and assessment, would be helpful to human resource planning endeavours. Future research should study indicators that are associated with a successful outcome, namely, obtaining a residency position or a practice opportunity; identify barriers that hinder the assimilation of IMGs into the Canadian health care system; and identify supportive measures that would facilitate their training and practice in Canada. Whereas the vast majority of IMGs immigrated to Canada with a medical degree, little is known about the subgroup of IMGs who are Canadians who left Canada to obtain a medical degree in another country; a better understanding of this subgroup is equally important.
Acknowledgments
We thank Gayle Rutherford for conducting the literature review, Sheila McDonagh for project management expertise, Shufen Edmondstone for secretarial assistance and Caroline Schmidtke for follow-up tracking and data management.
Footnotes
This article has been peer reviewed.
Contributors: Dr. Crutcher was the principal investigator and piloted the survey, refined the Web survey tool, supported quantitative and qualitative analysis, interpreted data, drafted the article and incorporated the literature review. Ms. Banner was co-leader with Dr. Crutcher during the conception and design stage. She refined the Web survey tool, managed the Web-based data acquisition process and contributed to data interpretation. Ms. Szafran made contributions to the concept and design and led the quantitative analysis and reporting and the creation of tables and figures. She made a major contribution to drafting the article. Dr. Watanabe contributed to study design and the Web-based survey tool and played a major role in data interpretation and writing of the interpretation section. All authors contributed to critical revisions and gave approval of the final version of the manuscript.
This study was funded by Health Canada (grant no. HCD-654110-60). The views of the authors are personal opinions and do not necessarily reflect the views of the organizations that they represent.
Competing interests: None declared.
Correspondence to: Dr. Rodney A. Crutcher, Department of Family Medicine, University of Calgary, UCMC Sunridge, 3465 26 Ave. NE, Calgary AB T1Y 6L4; fax 403 219-6120; crutcher@ucalgary.ca
References
- 1.Tyrrell L, Dauphinee D. Task force on physician supply in Canada. Canadian Medical Forum Task Force on Physician Supply in Canada; 1999. Available: www.cpsbc.bc.ca/physician/publications/supply.pdf (accessed 2003 Mar 3).
- 2.Watanabe M. Canadian physician workforce: the role of international medical graduates. In: International Medical Graduates National Symposium Proceedings; 2002 Apr 30–May 1; Calgary (AB). Ottawa: Health Canada; 2002. Cat no H21-211/2002F. p. 178-202.
- 3.The College of Family Physicians of Canada. Primary care and family medicine in Canada: a prescription for renewal. The College; 2000. Available: www.cfpc.ca/_cgi/toprint.asp?fn=/communications/prescription.asp (accessed 2003 Mar 3).
- 4.Barer ML, Stoddart GL. Toward integrated medical resource policies for Canada. 4. Graduates of foreign medical schools. CMAJ 1992;146(9):1549-54. [PMC free article] [PubMed]
- 5.Buske L. Canada's cosmopolitan medical profession. CMAJ 2002;166 (10):1320. [PMC free article] [PubMed]
- 6.Crutcher R. The Alberta International Medical Graduate Program: educational challenges and reflections. Section of Teachers of Family Medicine Newsl Mississauga (ON): The College of Family Physicians of Canada; 2001. Available: www.cfpc.ca/archive/educat/sot/vol9num2.asp#the (accessed 2003 Mar 3).
- 7.Health Human Resources Strategies Division, Health Canada. Immigration and settlement of international medical graduates. In: International Medical Graduates National Symposium Proceedings; 2002 Apr 30–May 1; Calgary (AB). Ottawa: Health Canada; 2002. Cat no H21-211/2002F. p. 153-77.
- 8.Association of International Physicians & Surgeons of Ontario (AIPSO). Integrating Canada's internationally-trained physicians. Towards a coherent, equitable and effective national system for the integration of internationally-trained physicians. Toronto: The Association; April 2002. Available: www.aipso.ca (accessed 2003 Apr 11).
- 9.Andrew R. Teaching international medical graduates in family medicine residency programs [commentary]. Section of Teachers of Family Medicine Newsl Mississauga (ON): The College of Family Physicians of Canada; 2001. Available: www.cfpc.ca/archive/educat/sot/vol9num2.asp (accessed 2003 Mar 03).
- 10.Cave AJ. Unlicensed international medical graduates (IMGs) survey 2000. Report to Alberta Health and Wellness. Edmonton (AB): Department of Family Medicine, University of Alberta; 2002.
- 11.Kvern B. Special feature: international medical graduates — issues related to family medicine education. Teaching international medical graduates in family medicine residency programs. Section of Teachers of Family Medicine Newsl Mississauga (ON): The College of Family Physicians of Canada; 2001. Available: www.cfpc.ca/archive/educat/sot/vol9num2.asp (accessed 2003 Mar 3).
- 12.Nasmith L. Programs for international medical graduates. Can Fam Physician 1993; 39:2549-53. [PMC free article] [PubMed]
- 13.Mick SS, Lee SY, Wodchis WP. Variations in geographical distribution of foreign and domestically trained physicians in the United States: ‘safety nets’ or ‘surplus exacerbation’? Soc Sci Med 2000;50(2):185-202. [DOI] [PubMed]
- 14.Canadian Resident Matching Service (CaRMS). Unfilled positions after second iteration, 2002 match. Available: www.carms.ca/stats/stats_index.htm (accessed 2003 Mar 13). (Note: To access this page, select Statistics from the 2002 match.)
- 15.Canadian Resident Matching Service (CaRMS). Students and graduates of international medical schools. 2002. Available: www.carms.ca/procedure/inter_index.htm (accessed 2003 Mar 3).
- 16.Banner S. Canadian Resident Matching Service: international medical graduates and the match. International Medical Graduates National Symposium Proceedings; 2002 Apr 30–May 1; Calgary (AB). Ottawa: Health Canada; 2002. Cat no H21-211/2002F. p. 89-93.
- 17.Facts and figures 2001: immigration overview. Ottawa: Citizenship and Immigration Canada; 2002. Available: www.cic.gc.ca/english/pdf/pub/facts2001.pdf (accessed 2003 Mar 3).
- 18.Blair L. Foreign doctors. Wasted resources? Can Fam Physician 1994;40:831-4. [PMC free article] [PubMed]
- 19.Koehn NN, Fryer GE, Phillips RL, Miller JB, Green LA. The increase in international medical graduates in family practice residency programs. Fam Med 2002;34(6):429-35. [PubMed]
- 20.Pugno PA, McPherson DS. The role of international medical graduates in family practice residencies. Fam Med 2002;34(6):468-9. [PubMed]
- 21.Lucas S. Medical migration – response. Lancet 2000;356:1197. [DOI] [PubMed]