

Abstract
Background
Controversy exists about whether abortion or childbirth is associated with greater psychological risks. We compared psychiatric admission rates of women in time periods from 90 days to 4 years after either abortion or childbirth.
Methods
We used California Medicaid (Medi-Cal) records of women aged 13–49 years at the time of either abortion or childbirth during 1989. Only women who had no psychiatric admissions or pregnancy events during the year before the target pregnancy event were included (n = 56 741). Psychiatric admissions were examined using logistic regression analyses, controlling for age and months of eligibility for Medi-Cal services.
Results
Overall, women who had had an abortion had a significantly higher relative risk of psychiatric admission compared with women who had delivered for every time period examined. Significant differences by major diagnostic categories were found for adjustment reactions (odds ratio [OR] 2.1, 95% confidence interval [CI] 1.1–4.1), single-episode (OR 1.9, 95% CI 1.3–2.9) and recurrent depressive psychosis (OR 2.1, 95% CI 1.3–3.5), and bipolar disorder (OR 3.0, 95% CI 1.5–6.0). Significant differences were also observed when the results were stratified by age.
Interpretation
Subsequent psychiatric admissions are more common among low-income women who have an induced abortion than among those who carry a pregnancy to term, both in the short and longer term.
Researchers who study women's psychological adjustment to abortion have faced a number of major methodological problems. Most published studies contain little or no objective information about women's psychological state before conception and are also limited in their follow-up to an evaluation a few months, weeks or even hours after an abortion.1,2
The importance of longer-term evaluation has been underscored by several recent studies showing delayed reactions to abortion among a minority of women.3,4,5 Major and colleagues,3 for example, carried out an investigation analyzing the psychological state of women 1 hour before abortion and 1 hour, 1 month and 2 years post abortion. In the post-abortion interviews, they found that depression, negative emotions and dissatisfaction with the abortion decision increased with time.
Other problems faced by researchers in this field are high attrition rates among women between the time of their abortion and subsequent interviews and concealment of past abortions. Fifty percent to 60% attrition or concealment rates are common.3,6,7
The problems of concealment, nonparticipation, insufficient time for follow-up and lack of information about previous psychological condition can be circumvented by means of record-based investigations. Unfortunately, very little research of this type has been conducted. The one important and widely cited exception is a record-based study by David and colleagues.8 They used a Danish registry system to examine psychiatric admissions for 3 months post partum and post abortion for all residents under the age of 50 years and found that the overall rate of psychiatric admission was 18.4 per 10 000 population for women who had had an abortion and 12.0 per 10 000 population for women who had given birth.
The goal of the present investigation was to further previous record-based research by examining psychiatric admissions relative to previous pregnancy outcome over a longer period of time, while controlling for previous psychiatric history, socioeconomic status, age and months of eligibility for state-funded medical care. In addition, the present study examined specific diagnoses among women admitted for psychiatric treatment, because the literature shows that the psychiatric illnesses most likely to be associated with previous abortion are psychotic, neurotic and affective in type.5,9,10,11 Women who have had an abortion also have significantly higher depression scores compared with women who carry unintended pregnancies to term.12 Additional research has shown that a small percentage of women (from 1.4%3 to 18.8%13 ) experience abortion as a traumatic event resulting in the symptoms of post-traumatic stress disorder.14
Methods
The California Department of Health Services (DHS) identified 249 625 women who had received funding for either an abortion or delivery in calendar year 1989 under the government-funded medical insurance program for low-income individuals known as Medi-Cal. In that year, pregnant women were eligible if their family income was less than 185% of the federally defined poverty level. About 27% of all abortions and 34% of all inpatient deliveries in California in 1989 were funded by Medi-Cal.15,16 Of this population, 194 694 (104 078 who had a delivery, 89 716 who had 1 or more abortions) were citizens whose beneficiary identification codes could be linked to valid social security numbers and at least 1 pregnancy event. All Medi-Cal “short paid claim” records for these women were obtained for 6 fiscal years beginning in July 1988 and extending through June 1994. Because the last target pregnancy date was Dec. 31, 1989, the maximum time period we could examine subsequent to all target pregnancies was 4.5 years. Encrypted social security numbers were provided for patient identification. Marital status information was not provided.
Screening for aberrant and missing data resulted in the elimination of 56 028 cases (21 494 who did not have abortions, 34 534 who did have abortions) for the following reasons: (1) costs associated with the target pregnancy event were below US$100 (suggesting that only counselling for a possible procedure was received); (2) the abortion was identified as illegal or unknown (clinical modification of the International Classification of Diseases, 9th revision17 [ICD-9-CM] codes 636 and 637); (3) the reported age of the individual was below 13 years or above 49 years at the time of their first pregnancy event; (4) the first pregnancy event occurred after 1989; (5) complete information for months of Medi-Cal eligibility was not available; or (6) the age recorded for an individual woman in the medical records could not be reasonably verified by reference to multiple records. The latter provision was employed to identify cases of either insurance fraud or data entry errors.
The cleaned data set left 138 666 cases for examination. Three additional criteria were then applied to arrive at the final study population. To avoid confounding effects, women who carried a pregnancy to term but had a known subsequent abortion were excluded. In addition, to ensure that we could control for at least 1 year of previous psychiatric and obstetric history, we selected only the cases of women who had their first known abortion or delivery between July 1 and Dec. 31, 1989. All cases where women had inpatient psychiatric treatment during the year before the target event (n = 108: 58 women who did have abortions, 50 women who did not have abortions) were then eliminated.
From the final population (n = 56 741), all women whose first known pregnancy in the target time period ended in abortion were selected as our case population (n = 15 299). All women whose pregnancy ended in delivery of a live birth and who had no known subsequent abortions were selected as the control group (n = 41 442).
Procedure codes relating to inpatient psychiatric claims (ICD-9 3-digit codes from 290–316) were extracted from the Medi-Cal claims file and matched by encrypted social security numbers to those women. Both age (r = 0.011, p < 0.008) and months of Medi-Cal eligibility (r = 0.054, p < 0.0001) were correlated with psychiatric admission and were, thus, used as covariates in every analysis.
Logistic regression analyses were carried out using psychiatric admission within 90 days, 180 days, 1 year (cumulatively) and during the second, third and fourth years (individually) after the first pregnancy event. Odds ratios and the total rate of admissions per 100 000 women were calculated for both the case and control groups. Admission rates were calculated after statistically removing the effects of age and months of eligibility during each time period specified. Univariate analyses were carried out in order to obtain the adjusted figures per 100 000 population. The results were further refined by stratification by age at the time of the first pregnancy event.
Analyses were also carried out by major ICD-9 diagnostic categories. We grouped these as schizophrenic disorders (code 295), single-episode (296.2) and recurrent (296.3) depressive psychosis, bipolar disorder (296.4–296.8), nonorganic psychoses (298), neurotic disorders (300), adjustment reactions (309), depressive disorder not classified elsewhere (311) and all other psychiatric codes. The codes for the first psychiatric admissions were used for these analyses. Only first-time admissions throughout the 4 years after the target pregnancy date were examined.
Results
The mean age of the women who delivered was 25.5 (standard deviation [SD] 5.8) years at the time of birth; the mean age of women who had an abortion was 24.8 (SD 6.1) years at the time of abortion. The mean number of months eligible for Medi-Cal assistance within the 4 years after the target pregnancy event was 27.3 (SD 18.4) months among women who delivered and 31.4 (SD 17.6) months among women who had an abortion.
Thirty-one women had their first admission for psychiatric treatment within the first 90 days, 56 were admitted within the first 180 days, 104 were admitted within the first year, 84 were admitted during the second year, 110 were admitted during the third year and 136 were admitted during the fourth year after the first pregnancy event. In total, 434 different women were admitted at least once for inpatient psychiatric treatment within 4 years after their first known abortion or delivery.
The raw totals and adjusted psychiatric admission rates for the 2 groups are presented in Tables 1 and 2, as well as adjusted odds ratios with 95% confidence intervals. As seen in Table 1, women who had abortions had a significantly higher inpatient admission rate than women who delivered during each time period analyzed. The highest odds ratio was found for the first 90 days after the pregnancy event, with women who had had an abortion being 2.6 times more likely to be admitted for psychiatric treatment than women who had delivered. The odds ratios tended to decrease over time.
Table 1
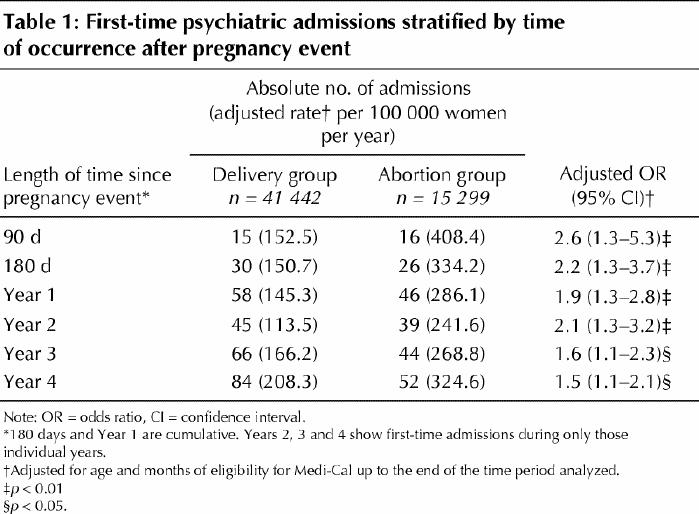
Table 2
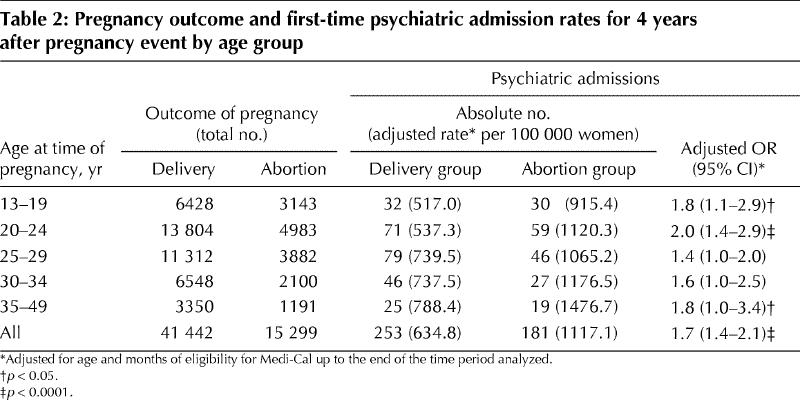
Table 2 shows psychiatric admission rates over the 4-year period stratified by age at the time of the first pregnancy event. Higher rates for psychiatric admissions among women who had abortions were observed relative to all age groups, but significant differences at the 95% confidence limit were only demonstrated among women aged 13–19 years, 20–24 years and 35–49 years.
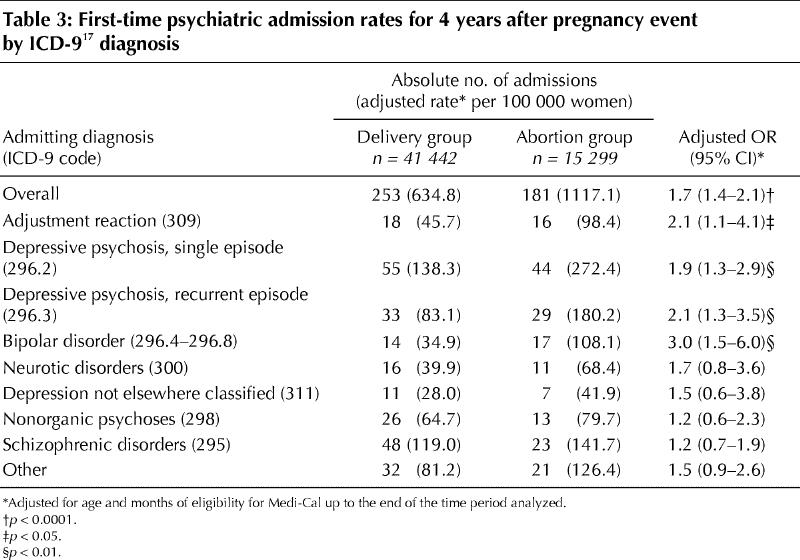
Regarding specific diagnoses, Table 3 shows that women who had an abortion had significantly higher rates of admission among the categories of adjustment reaction (odds ratio [OR] 2.1, 95% confidence interval [CI] 1.1–4.1), single-episode depressive psychosis (OR 1.9, 95% CI 1.3–2.9), recurrent depressive psychosis (OR 2.1, 95% CI 1.3–3.5) and bipolar disorder (OR 3.0, 95% CI 1.5–6.0). The most common diagnosis for psychiatric admission to hospital was single-episode depressive psychosis, which made up 21.7% of admissions for women who did not have an abortion and 24.3% of admissions for women who had an abortion.
Table 3
Interpretation
The present study revealed that psychiatric admission rates subsequent to the target pregnancy event were significantly higher for women who had had an abortion compared with women who had delivered during every time period examined. The greatest difference in admission rates occurred in the first 90 days. This was a counterintuitive result, because one would expect women who experience postpartum depression to be at greatest risk of admission within the first 90 days of delivery, whereas women who have an abortion would seem most likely to experience their highest levels of relief soon after the abortion.3
The differences in admission rates based on diagnoses (Table 3) are relatively consistent with those previously described.5,9,10,11,12,13,14 The observed associations may be the result of less social support for women who have an abortion compared with women who deliver,18,19 reactions to abortion itself12,13,14,20 or common risk factors among mentally ill women and those who have abortions that have not yet been identified.
This investigation adds to the work of David and colleagues8 by revealing differences over a longer period of time. In addition, David and colleagues did not control for socioeconomic status, which may be an important variable in both post-abortion and postpartum adjustments. Our data controls for socioeconomic status by using only women from the lowest socioeconomic group in the United States. This strength, however, also limits our ability to draw any conclusions from these findings regarding women of other socioeconomic groups.
Unfortunately, we were unable to examine or control for the potential effect of marital status. David and colleagues8 found that the greatest disparity in admission rates was among separated, widowed or divorced women. This suggests that social support following an abortion may be a significant mediator of adjustment.
The greatest limitation of this study is lack of access to complete medical histories. Both psychiatric admissions and pregnancy events that occurred more than 1 year before the period examined are unknown. Because our own findings reveal that observed differences persist beyond 1 year, the inclusion of women in our childbirth group who actually had a history of abortion is likely to have diluted the observed differences. Differences in earlier mental health history, more than a year before the pregnancy, may also have influenced the results. Even during the course of the years for which data were available, information gaps are also created by lapses of eligibility for Medi-Cal. These shortcomings could be eliminated, however, by using national, centralized medical records, such as those in Finland and Denmark, which contain complete records of obstetric and psychiatric treatments.
Additional research, using data that encompass complete medical histories, is strongly recommended. Clinicians who are alert to a patient's history of pregnancy loss may be better able to identify women who would benefit from a referral for counselling.
β See related article page 1257
Footnotes
This article has been peer reviewed.
Contributors: Dr. Reardon contributed to study conception and design; data acquisition, preparation, analysis and interpretation; and manuscript preparation. Mr. Coulge contributed to data preparation, analysis and interpretation and critical revision of the manuscript for important intellectual content. Drs. Rue, Shuping and Ney contributed to data analysis and interpretation and critical revision of the manuscript for important intellectual content. Dr. Coleman contributed to data preparation, analysis and interpretation and critical revision of the manuscript for important intellectual content.
Competing interests: None declared.
Correspondence to: Dr. David C. Reardon, Elliot Institute, PO Box 7348, Springfield IL 62791-7348, USA; fax 217 525-8212; dreardon@mine4ever.net
References
- 1.Wilmoth GH, de Alterlis M. Prevalence of psychological risks following legal abortion in the U.S.: limits of the evidence. J Soc Issues 1992;48(3):37-66.
- 2.Rogers J, Phifer J, Nelson J. Psychological impact of abortion: methodological and outcomes summary of empirical research between 1966 and 1988. Health Care Women Int 1989;10:347-76. [DOI] [PubMed]
- 3.Major B, Cozzarelli C, Cooper ML, Zubek J, Richards C, Wilhite M, et al. Psychological responses of women after first-trimester abortion. Arch Gen Psychiatry 2000;57(8):777-84. [DOI] [PubMed]
- 4.Miller WB, Pasta DJ, Dean CL. Testing a model of the psychological consequences of abortion. In: Beckman LJ, Harvey SM, editors. The new civil war: the psychology, culture, and politics of abortion. Washington: American Psychological Association; 1998. p. 235-67.
- 5.Söderberg H, Janzon L, Sjöberg NO. Emotional distress following induced abortion: a study of its incidence and determinants among abortees in Malmo, Sweden. Eur J Obstet Gynecol Reprod Biol 1998;79(2):173-8. [DOI] [PubMed]
- 6.Jones EF, Forrest JD. Underreporting of abortion in surveys of U.S. women: 1976 to 1988. Demography 1992;29(1):113-26. [PubMed]
- 7.Söderberg H, Andersson C, Janzon L, Sjöberg NO. Selection bias in a study on how women experienced induced abortion. Eur J Obstet Gynecol Reprod Biol 1998; 77(1):67-70. [DOI] [PubMed]
- 8.David H, Rasmussen N, Holst E. Post-abortion and postpartum psychotic reactions. Fam Plann Perspect 1981;13(1):32-4. [PubMed]
- 9.Zolese G, Blacker CVR. The psychological complications of therapeutic abortion. Br J Psychiatry 1992;160:742-9. [DOI] [PubMed]
- 10.Bradley CF. Abortion and subsequent pregnancy. Can J Psychiatry 1984; 29 (6): 494-8. [DOI] [PubMed]
- 11.Uruhart DR, Templeton AA. Psychiatric morbidity and acceptability following medical and surgical methods of induced abortion. Br J Obstet Gynecol 1991;98(4):396-9. [DOI] [PubMed]
- 12.Reardon DC, Cougle JR. Depression and unintended pregnancy in the National Longitudinal Survey of Youth: a cohort study. BMJ 2002;324:151-2. [DOI] [PMC free article] [PubMed]
- 13.Barnard CA. The long term psychological effects of abortion. Portsmouth (NH): Institute for Pregnancy Loss; 1990.
- 14.Speckhard A, Rue VM. Postabortion syndrome: an emerging public health concern. J Soc Issues 1992;48:95-120.
- 15.Medical Care Statistics Section. Medi-Cal funded induced abortions, 1989. Sacramento (CA): California Department of Health Services; 1991.
- 16.Medical Care Statistics Section. Medi-Cal funded deliveries, 1989. Sacramento (CA): California Department of Health Services; 1991.
- 17.International classification of diseases, 9th revision (clinical modification). 5th ed. Washington: US Department of Health and Human Services; 1996. Cat no 86-72897.
- 18.Major B, Cozzarelli C, Sciacchitano AM, Cooper ML, Testa M. Perceived social support, self-efficacy and adjustment to abortion. J Pers Soc Psychol 1990;59(3):452-63. [DOI] [PubMed]
- 19.Major B, Zubek JM, Cooper ML, Cozzarelli C, Richards C. Mixed messages: implications of social conflict and social support within close relationships for adjustment to a stressful life event. J Pers Soc Psychol 1997;72(6):1349-63. [DOI] [PubMed]
- 20.Morgan CM, Evans M, Peter JR, Currie C. Mental health may deteriorate as a direct effect of induced abortion. BMJ 1997;314:902. [PMC free article] [PubMed]