

Abstract
We used National Performance Evaluation Survey data to estimate the prevalence and associated factors of edentulism among noninstitutionalized adults aged 35 years and older in Mexico. Statistically, the variables positively associated with edentulism were older age (odds ratio [OR]=1.08) and female gender (OR=1.79). Nonsmoking status (OR=0.70) and having a higher wealth index score (OR=0.72) were negatively associated. This information constitutes the first large-scale evaluation in Mexico for one of the World Health Organization’s priority oral health problems.
The World Health Organization (WHO) considers edentulism (complete absence of natural teeth) a poor public health outcome that substantially affects oral and general health status, as well as quality of life. It is an important but often-overlooked public health issue, especially for the elderly.1,2 Oral health status plays an important role in the nutrition of adults and older people.3 Tooth loss has been associated with changes in food taste and food preferences and nutritional deficiency.3,4 Little oral health epidemiological information is available for the Mexican populations: specifically, no information is available on prevalence of edentulism in adults and the elderly. The objective of this study was to determine the prevalence and associated factors of edentulism among a large-scale sample of noninstitutionalized people aged 35 years and older in Mexico.
METHODS
The National Performance Evaluation Survey 2002–2003 (a countrywide evaluation of health services in Mexico) was part of the technical collaboration between the Ministry of Health of Mexico and WHO, which used the survey instrument and sampling strategies developed by WHO for the World Health Survey. The National Institute of Public Health and the Ministry of Health of Mexico General Directorate of Performance Evaluation undertook the survey. The National Performance Evaluation Survey provides policymakers with reliable and internationally comparable baseline information on a variety of health indicators, including general population health measures and the effectiveness of health systems.
The National Performance Evaluation Survey was conducted between November 2002 and April 2003 and collected information from 38 746 households in 32 states in Mexico, with a mean of 1250 households per state, although only 20 Mexican states collected dental data. The sampling frame was probabilistic, stratified, used a multistage cluster design and was calculated to provide representative information at both the state level and by urban and rural areas.5
The survey comprised a face-to-face interview divided into household and individual questionnaires. (Both questionnaires and a discussion of general methodological issues are available on WHO’s Web page: http://www3.who.int/whs/P/instrumentandrel8293.html.) The household survey includes general topics, such as physical characteristics of the household and ownership of consumer goods, which were combined in the polychoric principal components analyses to construct a wealth index.6
The dependent variable in our analyses was self-reported edentulism (individuals who stated that they had lost all of their natural teeth). Weighted analyses were conducted in Stata software 8.2 (StataCorp LP, College Station, Tex) with the module svy Bivariate and multivariate logistic regression analyses were undertaken. To avoid multicollinearity in the variables included in the final model, the variance inflation factor test was performed. Finally, the Box-Tidwell test was performed to evaluate whether continuous variables in the final model were related to the logit of the dependent variable lineally. The multivariate logistic regression model incorporated all variables available (socio-demographic and socioeconomic) that were thought to be related to edentulism and associated at the bivariate analysis level with P < .25 to control for possible confusion.
RESULTS
National Performance Evaluation Survey data on dental conditions were available only for subjects aged 18 years and older, representing a total of 24 159 households. In the current round of analyses, only survey respondents who were aged older than 35 years (n = 13 966) were included, representing 29 853 607 adult country inhabitants. All results presented are weighted. The mean age was 50.95 ± 12.98 SD (ranging from 35 to 98 years old), with 57.9% women (n = 17 296 022) and 42.1% men (n = 12 557 585). Overall prevalence of edentulism in this adult population was 10.2%; when the WHO’s “age index” for prevalence of edentulism was used, the proportion for the elderly ( > 65 years old) was 30.6% and for the younger adults (35–44 years old) was 2.4%. Figure 1 ▶ shows the geographic distribution of edentulism in Mexico, with prevalence ranging from 5.0% in Tlaxcala (central Mexico) to 16.7% in Michoacán (western Mexico). Table 1 ▶ presents descriptive results for the study population.
FIGURE 1—
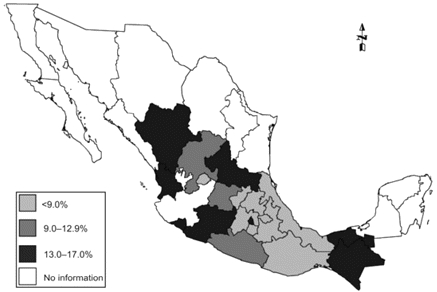
Geographic distribution of edentulism in 20 of 32 states of Mexico, as a weighted percentage of the population.
TABLE 1—
Household and Individual Characteristics of the Population (n = 29 853 607) Associated With Edentulism in the Bivariate Logistic Regression Analyses
| n | % Weighted | OR (95% CI) | |
| Age | 13 966 | 100 | 1.08 (1.07, 1.09)*** |
| Gender | |||
| Men | 5975 | 42.1 | 1.00 |
| Women | 7991 | 57.9 | 1.48 (1.27, 1.73)*** |
| Smoking | |||
| Never | 10 872 | 77.3 | 1.00 |
| Sometimes | 1964 | 15.4 | 1.09 (0.82, 1.46) |
| Daily 1–5 times | 614 | 4.2 | 1.02 (0.71, 1.46) |
| Daily > 5 times | 516 | 3.1 | 1.53 (1.04, 2.23)* |
| Years smoking daily | |||
| < 10 | 251 | 24.1 | 1.00 |
| 11–20 | 334 | 29.3 | 1.96 (0.79, 4.87) |
| 21–30 | 247 | 24.2 | 2.52 (1.05, 6.06)* |
| > 30 | 298 | 22.4 | 4.34 (2.05, 9.19)*** |
| Diabetes | |||
| No | 12 782 | 91.6 | 1.00 |
| Yes | 1184 | 8.4 | 1.82 (1.39, 2.38)*** |
| Preventive attitude | |||
| No | 8944 | 61.8 | 1.00 |
| Yes | 5022 | 38.2 | 0.59 (0.48, 0.72)*** |
| Health insurance | |||
| Without insurance | 8426 | 61.2 | 1.00 |
| With insurance | 5510 | 38.8 | 1.31 (1.08, 1.59)** |
| Schooling | |||
| Elementary incomplete | 3151 | 21.1 | 1.00 |
| Elementary complete | 6834 | 48.9 | 0.47 (0.38, 0.59)*** |
| Middle complete | 1911 | 14.7 | 0.31 (0.21, 0.45)*** |
| High school | 1176 | 9.0 | 0.24 (0.14, 0.41)*** |
| College | 894 | 6.2 | 0.32 (0.22, 0.49)*** |
| Marital status | |||
| Married | 8867 | 67.2 | 1.00 |
| Single | 997 | 6.0 | 1.15 (0.85, 1.56) |
| Divorced | 1011 | 6.2 | 1.49 (1.06, 2.08)* |
| Widowed | 2023 | 11.2 | 3.88 (3.05, 4.95)*** |
| Cohabitant | 1068 | 9.3 | 0.78 (0.48, 1.25) |
| Occupation | |||
| Government employee | 1243 | 7.7 | 1.00 |
| Nongovernment employee | 1349 | 10.3 | 1.13 (0.73, 1.74) |
| Self-employed | 4079 | 29.3 | 1.85 (1.22, 2.79)** |
| Does not work/voluntary worker | 7295 | 52.7 | 3.87 (2.64, 5.68)*** |
| Residence | |||
| Rural | 4128 | 26.6 | 1.00 |
| Urban | 9831 | 73.3 | 1.06 (0.81, 1.40) |
| Indian ethnic status | |||
| No | 13 054 | 92.5 | 1.00 |
| Yes | 801 | 7.5 | 0.75 (0.51, 1.12) |
| Wealth index | |||
| 1 (poorest) | 3734 | 28.4 | 1.22 (0.93, 1.59) |
| 2 | 3509 | 24.1 | 1.41 (1.12, 1.78)** |
| 3 | 3440 | 24.0 | 0.92 (0.64, 1.31) |
| 4 (highest) | 3036 | 23.5 | 1.00 |
Note. OR = odds ratio; CI = confidence interval.
* P < .05; **P < .01; ***P < .001.
In the bivariate analyses (Table 1 ▶), we observed that age, gender, smoking, diabetes, health insurance status, marital status, occupation, and wealth index were positively associated with edentulism, whereas preventive attitude and higher level of schooling were negatively associated with edentulism. The multivariate logistic regression model (Table 2 ▶) adjusted for schooling and Indian ethnic status showed that for each year of age increase, the odds of being edentulous increased 8% (95% confidence interval [CI]=1.07, 1.09), with women being 1.79 times more likely (95% CI=1.50, 2.13) to be edentulous, but nonsmokers (odds ratio [OR]=0.70; 95% CI=0.54, 0.90) and better-off people (higher wealth index) (OR=0.72; 95% CI=0.53, 0.98) being less likely to lose all of their natural teeth. No plausible interaction terms were significant. There was no effect when differentiating urban and rural areas.
TABLE 2—
Multivariate Logistic Regression Model for Edentulism in Mexican Adults
| Adjusted OR (95% CI) | |
| Years of age | 1.08 (1.07, 1.09)*** |
| Gender | |
| Men | 1.00 |
| Women | 1.79 (1.50, 2.13)*** |
| Smoking | |
| Sometimes, daily | 1.00 |
| No, never | 0.70 (0.54, 0.90)** |
| Wealth index | |
| First, second, or third quartile | 1.00 |
| Fourth quartile | 0.72 (0.53, 0.98)* |
Note. OR = odds ratio; CI = confidence interval. Box–Tidwell for age: P = .075. Hosmer–Lemeshow goodness-of-fit: χ28 = 7.06; P = .5304.
* P < .05; **P < .01; ***P < .001.
DISCUSSION
The importance of preserving teeth in good condition not only may be restricted to quality of life in the elderly1,2 but also may be an indicator of general health because edentulism is associated with systemic, chronic diseases.7–9 Our study provided large-scale data for the first time in Mexico on one of the priority oral health indicators proposed by WHO. Most of the studies performed in other countries have included only people aged 60 years and older.
The prevalence observed in our study for the elderly (30.6%) can be contrasted with reports from other countries; both similarities and disparities occur. Our findings fall within the range derived from a telephone survey in the United States10: in 1997, the prevalence ranged from 13.9% (in Hawaii) to 47.9% (in West Virginia), and in 2002, it ranged from 13% (in Hawaii and California) to 42% (in Kentucky).11 The Mexican prevalence is also similar to that observed in Australians (also obtained through self-report in a telephone survey)1 but much higher than the 7.0% reported in Japanese adults.12 As in the other studies, our results were based on self-reports that, although not verified by dental personnel, have been shown to have high correlation with clinical examinations in these age groups.13 It can be safely assumed that the lay public knows when no teeth are present.
As previously reported, age is strongly associated with edentulism1,14; this finding is not surprising, because the cumulative effects of dental caries and periodontal diseases,15,16 as well as treatment decisions associated with these 2 main reasons for tooth loss, increase with age. Differential treatment choices across the socioeconomic continuum, such as endodontic treatment versus tooth extraction, also may play a role in the overall tooth loss phenomenon. As reported by other authors, women are more likely to be edentulous than are men.1 Because cigarette smoking is a risk factor for adult periodontitis and tooth loss,10 the higher prevalence of edentulism among smokers may be directly related to the adverse effects of smoking on periodontal health. This association also has been observed in other studies.10,17 The periodontal status of former smokers ranks between that of never smokers and current smokers, suggesting that smoking causes changes in the periodontium but that the deterioration may not continue after tobacco use cessation.18
As in other countries, we found that edentulism is closely associated with socioeconomic variables. Epidemiological studies show that persons of low social class or low income and individuals with few years of schooling are more likely to be edentulous than are persons of higher social class, income, and educational attainment.14
Our study had certain limitations that emphasize a cautious interpretation of results. A cross-sectional study measures associations at 1 point in time, introducing the problem of temporal ambiguity and the inability to establish causal relationships. Furthermore, this study cannot be considered truly nationally representative because 12 of 32 states (mostly northern states) were excluded because of survey logistics. Contrast of results with other countries is limited by necessity because studies in comparable settings in emerging economies are not available.
This baseline information constitutes the first national evaluation in Mexico for one of the priority WHO oral health problems. The observed prevalence of edentulism was moderate to low in the adult and elderly groups (compared with other reports in non-Mexican populations). This important oral health condition was strongly linked to birth cohorts and possibly associated with increasing age. This study of noninstitutionalized adults found a significant relation between sociodemographic variables (e.g., age and gender) and edentulism, with socioeconomic status (as measured by the wealth index) playing a role in the prevalence of edentulism. Nonsmoking status had an effect on edentulism, separate from socioeconomic and sociodemographic factors. Future studies should examine risk factors for tooth loss to effect changes in health systems and increase tooth longevity.
Peer Reviewed
Contributors C. E. Medina-Solís and R. Pérez-Núñez were responsible for the study concept and design, supervised all aspects of the study, and were responsible for the integrity of the data and the accuracy of the data analysis and interpretation. G. Maupomé and J. F. Casanova-Rosado assisted with the analyses and interpretation of data.
Human Participant Protection No protocol approval was needed for this study because secondary data were used from a previously approved protocol by the World Health Organization and National Institute of Public Health’s ethical and research committees.
References
- 1.Adams C, Slack-Smith LM, Larson A, O’Grady MJ. Edentulism and associated factors in people 60 years and over from rural and remote Western Australia. Aust Dent J. 2003;48:10–14. [DOI] [PubMed] [Google Scholar]
- 2.Steele JG, Sanders AE, Slade GD, et al. How do age and tooth loss affect oral health impacts and quality of life? A study comparing two national samples. Community Dent Oral Epidemiol. 2004;32:107–114. [DOI] [PubMed] [Google Scholar]
- 3.Marcenes W, Steele JG, Sheiham A, Walls AW. The relationship between dental status, food selection, nutrient intake, nutritional status, and body mass index in older people. Cad Saude Publica. 2003;19:809–816. [DOI] [PubMed] [Google Scholar]
- 4.Lee JS, Weyant RJ, Corby P, et al. Edentulism and nutritional status in a biracial sample of well-functioning, community-dwelling elderly: the health, aging, and body composition study. Am J Clin Nutr. 2004;79:295–302. [DOI] [PubMed] [Google Scholar]
- 5.Palma-Coca O, Olaiz-Fernández G. Metodología de la Encuesta Nacional de Evaluación del Desempeño [Methods of the Mexican National Performance Assessment Survey]. Salud Publica Mex. 2005;47(suppl 1): S66–S74. [PubMed] [Google Scholar]
- 6.Kolenikov S, Angeles G. The Use of Discrete Data in Principal Component Analysis With Applications to Socio-Economic Indices. Working Paper WP-04-85. Chapel Hill, NC: CPC MEASURE; 2004.
- 7.Abnet CC, Qiao YL, Mark SD, Dong ZW, Taylor PR, Dawsey SM. Prospective study of tooth loss and incident esophageal and gastric cancers in China. Cancer Causes Control. 2001;12:847–854. [DOI] [PubMed] [Google Scholar]
- 8.Frisk F, Hakeberg M, Ahlqwist M, Bengtsson C. Endodontic variables and coronary heart disease. Acta Odontol Scand. 2003;61:257–262. [DOI] [PubMed] [Google Scholar]
- 9.Taguchi A, Sanada M, Suei Y, et al. Tooth loss is associated with an increased risk of hypertension in post-menopausal women. Hypertension. 2004;43:1297–1300. [DOI] [PubMed] [Google Scholar]
- 10.Centers for Disease Control and Prevention (CDC). Total tooth loss among persons aged >65 years—selected states, 1995–1997. MMWR Morb Mortal Wkly Rep. 1999;48:206–210. [PubMed] [Google Scholar]
- 11.Centers for Disease Control and Prevention (CDC). Public health and aging: retention of natural teeth among older adults—United States, 2002. MMWR Morb Mortal Wkly Rep. 2003;52:1226–1229. [PubMed] [Google Scholar]
- 12.Ikebe K, Nokubi T, Ettinger RL, et al. Dental status and satisfaction with oral function in a sample of community-dwelling elderly people in Japan. Spec Care Dentist. 2002;22:33–40. [DOI] [PubMed] [Google Scholar]
- 13.Douglass CW, Berlin J, Tennstedt S. The validity of self-reported oral health status in the elderly. J Public Health Dent. 1991;51:220–222. [DOI] [PubMed] [Google Scholar]
- 14.Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2005;33:81–92. [DOI] [PubMed] [Google Scholar]
- 15.Casanova-Rosado AJ, Medina-Solís CE, Casanova-Rosado JF, Vallejos-Sánchez AA, Maupomé G, Ávila-Burgos L. Dental caries and associated factor in Mexican schoolchildren aged 6–13 years. Acta Odontol Scand. 2005;63:245–251. [DOI] [PubMed] [Google Scholar]
- 16.Susin C, Dalla Vecchia CF, Oppermann RV, Haugejorden O, Albandar JM. Periodontal attachment loss in an urban population of Brazilian adults: effect of demographic, behavioral, and environmental risk indicators. J Periodontol. 2004;75:1033–1041. [DOI] [PubMed] [Google Scholar]
- 17.Suominen-Taipale AL, Alanen P, Helenius H, Nordblad A, Uutela A. Edentulism among Finnish adults of working age, 1978–1997. Community Dent Oral Epidemiol. 1999;27:353–365. [DOI] [PubMed] [Google Scholar]
- 18.Johnson GK, Slach NA. Impact of tobacco use on periodontal status. J Dent Educ. 2001;65:313–321. [PubMed] [Google Scholar]