

Abstract
Many patients with unilateral or bilateral testicular, epididymal, or scrotal pain as their sole presenting symptom receive a diagnosis of “chronic epididymitis.” This common clinical entity is diagnosed and treated by practicing urologists but essentially ignored by academic urologists. This article defines chronic epididymitis, reviews current knowledge regarding its etiology, and describes appropriate physical examination and clinical testing for patients with the condition. The recently developed Chronic Epididymitis Symptom Index is presented, which can be used for baseline evaluation and follow-up of patients with chronic epididymitis, both in clinical practice and in research treatment trials. Treatment options, from watchful waiting to medical therapy to epididymectomy, are reviewed.
Key words: Epididymitis, Scrotal pain, Testicular pain, Epididymectomy
Practitioners of general urology see numerous patients with unilateral or bilateral testicular, epididymal, or scrotal pain as their sole presenting symptom. Many, if not most, of these patients eventually receive a diagnosis of “chronic epididymitis.” Although every urologist sees such patients, and the majority agree that it is a common urologic office diagnosis, prevalence and incidence studies of chronic epididymitis are unavailable. Until recently, there have been no clearly described definitions, no generally accepted classification system, and no suggested diagnostic criteria associated with this clinical condition. Anecdotally, treatment consists of administration of antibiotics and anti-inflammatory agents and, if that fails, occasionally epididymectomy. Studies describing the results of therapy are sadly lacking in the literature. The natural history of this condition has never been prospectively explored, so urologists are unaware of what eventually happens to these patients.
Clinical Presentation
Men diagnosed with chronic epididymitis generally present with either unilateral or bilateral scrotal pain that can be localized to either a normal- or abnormal-feeling epididymis. Many patients with chronic epididymitis also have associated testicular pain. Chronic testicular pain, or “chronic orchalgia,” has been defined as “intermittent or constant testicular pain three months or longer in duration that significantly interferes with the daily activities of the patient so as to prompt him to seek medical attention.”1 In many cases, however, the patient will present with epididymal pain and discomfort only, particularly in the chronic stage of the condition.
Every urologist will have his or her own anecdotal recollection of the presentation and natural history of chronic epididymitis. Each urologist’s experience may be different because of the patient population he or she serves or the clinical definitions associated with chronic scrotal pain learned during his or her residency training. Most urologists will agree that chronic epididymitis can be unilateral or bilateral; can range from mild, intermittent discomfort to severe, constant pain; can be exacerbated by certain activities, including ejaculation; can be associated with a normal-feeling or enlarged indurated epididymis; and appears to wax and wane over time. However, to our knowledge, until recently, there has been no prospective attempt to describe the presentation of these patients.
The Patient with Chronic Epididymitis: A Prospective Study
Our research group recently published a report2 on a series of 50 consecutive men presenting to our outpatient urology clinic with a diagnosis of chronic epididymitis based on a predetermined definition of the condition (see below). We compared demographic data, presenting complaints, quality of life, and other data for these 50 chronic epididymitis patients with those of 20 normal controls with no history of testicular, scrotal, or epididymal pain.
Definition of Chronic Epididymitis
From our review of the sparse literature on the subject,3 relying heavily on standard urology textbooks,4,5 we defined chronic epididymitis as “symptoms of discomfort and/or pain at least 3 months in duration in the scrotum, testicle, or epididymis, localized to one or each epididymis on clinical examination.”
The average age (± standard deviation) of a patient presenting to our urology clinic with chronic epididymitis was 49 ± 15 years (range, 21–83 years). The patients had an average symptom duration of 4.9 ± 7 years (range, 0.25–29 years). Sixty-four percent of patients had pain in the scrotum often, usually, or always. At the time the subjects were surveyed, the average pain score was 4.7 ± 2.1 on a scale of 0 (no pain) to 10 (pain as bad as imaginable). Pain was localized to the right side in 44%, to the left side in 34%, and bilateral in 22% of the cases. The symptom complex associated with this moderate to severe discomfort or pain seemed to have a significant impact on patient quality of life. Patients thought about the condition frequently, it affected their daily activities, and they were not satisfied with their quality of life.
In a comprehensive demographic analysis, compared with control patients, men diagnosed with chronic epididymitis had more sexual partners, used sexually transmitted disease protection less often, and had a higher incidence of past sexually transmitted disease. Patients with chronic epididymitis had more general self-reported musculoskeletal, neurologic, and infectious and/or inflammatory medical problems, including a history of urinary tract infections, than did men without this condition. Depression appeared to be a major problem in patients presenting with chronic epididymitis. Surprisingly, a history of vasectomy did not have a major association with a diagnosis of this condition (see Etiology, below), but that could be because this was a small, case-control study.
Epidemiology
It is surprising that no effort has been made to determine the incidence or prevalence of this common and important, but neglected, urologic diagnosis. Anecdotally, it seems that chronic epididymitis is diagnosed and treated often, and this condition certainly has a significant effect on patient quality of life. Although never studied, the socioeconomic impact of chronic epididymitis must be significant, because the men affected, on average, are in the most productive years of their lives. It would seem reasonably simple to undertake retrospective physician chart reviews or examine comprehensive billing data to determine the actual incidence of this condition.
The only epidemiologic information that we could find was from a study published in 1966, in which epididymitis was determined to be the most common disease for which patients were admitted to the urology service at most army medical institutions. 6 Of 610 patients hospitalized in this armed forces clinical series, at least 89 (14.8%) received a diagnosis of chronic or recurrent epididymitis.
Etiology
No comprehensive attempt has been made by past researchers to determine the etiology and pathogenesis of chronic epididymitis. Based on experience and our review of the literature, we would suggest that the etiology of this condition can be associated with inflammatory, infectious, or obstructive factors; however, in many cases, no etiology can be identified. There is some evidence that chronic epididymitis may be infective (eg, chlamydia7) and, although there are no studies to confirm this, there seems to be a postinfective chronic epididymitis (ie, after an episode of acute bacterial epididymitis, the inflammation and discomfort persist). Granulomatous epididymitis (eg, tuberculous or bacillus Calmette-Guérin) has been well described.8,9 Drug-induced epididymitis (eg, amiodarone) is also a well-recognized entity,10 as is chronic epididymitis associated with other generalized diseases (eg, Behçet’s disease).11 However, many patients present with an inflammatory type of epididymitis (pain and/or discomfort associated with inflammatory swelling and/or induration of the epididymis) for which no identifiable etiology is apparent.
Chronic epididymitis can be associated with obstruction distal to the epididymis (eg, vas deferens). It has been well described as occurring after vasectomy12,13 and can also be seen in patients with congenital abnormalities of the lower urinary tract.
Many patients, however, present with chronic pain and/or discomfort of varying intensity associated with a normal epididymis that can sometimes be exquisitely tender on palpation. Often, these patients have no identifiable etiology for the pain (although it is tempting to believe that these patients may have a neuropathic type of epididymal pain).
Based on our review of the literature3 and our prospective, case-control study,2 we developed a classification system for chronic epididymitis that could prove useful for future clinical studies. The classification system could also be helpful in defining patients in clinical practice and in making treatment decisions. Our proposed definition and classification of chronic epididymitis is presented in Table 1.
Table 1.
Definition and Classification of Chronic Epididymitis
| Definition: A 3-month or longer history of symptoms of discomfort/pain in the scrotum/testicle or epididymis that are localized to one or both epididymides on clinical examination. |
| Classification: |
|
Clinical Evaluation
Compared with the vast literature on the diagnosis and clinical evaluation of the patient presenting with acute epididymitis,14 information on the diagnosis and evaluation of the patient presenting with chronic epididymitis is extremely sparse.
History
It seems reasonable to begin with the clinical definition presented in Table 1 and proceed through a clinical evaluation to classify the patient into one of the categories also described in Table 1. Patient history taking should include a determination of the location, severity, and frequency of pain; associated symptoms; exacerbating factors; and impact of the condition on the patient’s quality of life. Past medical history and systems review should include medications taken, past surgical history (particularly scrotal surgery, such as vasectomy), other urologic history (eg, stones, urinary tract infections), sexual history (including type of contraceptive used and history of sexually transmitted diseases), and other associated medical conditions.
Chronic Epididymitis Symptom Index
There are a number of urologic conditions for which assessment of symptoms is the only reasonable way to stratify patients as to severity and to follow them over time. Validated symptom indices have proved invaluable for these conditions, not only in clinical treatment trials but also in clinical practice. These conditions include benign prostatic hyperplasia, chronic prostatitis, erectile dysfunction, and interstitial cystitis.
During our prospective evaluation of the chronic epididymitis case-control study previously described,2 we developed and validated a symptom index that can serve a similar purpose for the baseline evaluation and follow-up of patients with chronic epididymitis, both in clinical practice and research treatment trials. This index, the Chronic Epididymitis Symptom Index (CESI), is presented as Figure 1.
Figure 1.

The Chronic Epididymitis Symptom Index (CESI).
In the CESI, the frequency of pain and/or discomfort is rated from 0 to 5, and the severity of pain and/or discomfort is rated from 0 to 10. From these items, a chronic epididymitis pain subscore (range, 0–15) is derived. The impact/quality-of-life questions validated for patients with chronic prostatitis in the National Institutes of Health Chronic Prostatitis Symptom Index (NIH-CPSI)15 appear to accurately demonstrate the significant impact that specific epididymitis symptoms have on patients with chronic epididymitis. Thus, a chronic epididymitis quality-of-life/impact domain (score ranging from 0 to 12) was created based on the NIH-CPSI. By combining these 2 domains, a total CESI score (range, 0–27) can be determined.
The average CESI pain subscore in patients with chronic epididymitis in the case-control study was 6.9 ± 3.0, the average CESI quality-of-life/impact subscore was 6.9 ± 3.2, and the total CESI score in those presenting to our outpatient clinic with a diagnosis of chronic epididymitis was 13.8 ± 6.4. The asymptomatic control group had a CESI score of zero.2
Physical Examination
During physical examination, attention should be focused on the lower abdomen, external genitalia, and prostate. Careful examination of the scrotum and its contents will determine the location of pain and any association with induration, inflammation, or masses within the spermatic cord, epididymis, and/or testicle. If the condition is unilateral, it is best to examine the unaffected side first.
Other Tests
A urinalysis and midstream urine sample for culture are appropriate basic examinations. In patients who complain of urethral discharge, urethral symptoms, or penile pain, a urethral swab for bacterial culture and chlamydia is indicated. If patients present with prostatitis-like symptoms (eg, perineal pain/discomfort), consideration may be given to proceeding with lower urinary tract localization studies, such as the Meares-Stamey four-glass test16 or the simpler pre- and post-massage test.17 Doppler ultrasound has shown some efficacy in the differentiation of acute epididymitis from torsion of the testicle. However, its utility in chronic epididymitis is relegated to determining vascularity and echogenic heterogeneity in an indurated epididymis; ruling out an epididymal mass in a large, painful epididymis; or determining whether the patient has associated epididymal cysts (Figure 2). Other investigations and radiologic evaluations should be directed by specific findings on history taking and physical examination.
FIgure 2.
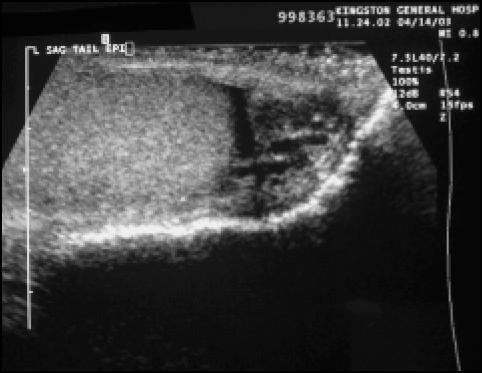
An enlarged heterogeneous (mixed echogenicity) epididymis in a young man with an indurated painful epididymis of 8-month duration (sagittal view of lower pole of testicle [left] and tail of epididymis [right]).
Treatment
Conservative Therapy
Many urologists suggest watchful waiting for patients in whom symptoms are mild and/or transitory. Empathy and reassurance (particularly that the pain and/or induration of the epididymis does not represent a cancer) is all some patients require. If future studies determine the natural history of this condition, we may be able to reassure some patients that it is a condition that “burns out” over time. Scrotal support, local heat therapy, and avoidance of aggravating activities may also be useful suggestions.
Medical Therapy
Medical treatment regimens for patients with chronic epididymitis are essentially nonexistent. Published studies examining other potential treatment modalities are also sparse and usually describe surgical outcomes (epididymectomy) in these patients. The most common previous therapies recollected by the patients in our published case-control study2 were antibiotics (74%), anti-inflammatory agents (36%), phytotherapy (16%), anxiolytics (12%), narcotic analgesics (10%), acupuncture (8%), and injection therapy (steroid or anesthetic) (6%). At the time of the survey, about one fourth (26%) of the patients were taking some type of pain medication. This small series probably represents the most common therapies employed by primary care physicians. It is probable that urologists use a similar medical treatment plan but also consider epididymectomy if the case is refractory to medical therapy. To our knowledge, there are no good prospective studies evaluating these therapies in patients with chronic epididymitis.
Surgical Therapy
There are more data related to the potential benefits of epididymectomy in patients with chronic epididymitis and epididymo-orchitis. In the 89 patients identified with chronic or recurrent epididymitis in Mittemeyer and colleagues’ armed forces study,6 61 underwent epididymectomy and eventually returned to active duty. Davis and colleagues1 reported a clinical series of patients with chronic orchalgia, although many appeared to have at least an associated diagnosis of chronic epididymitis. Thirty-one patients underwent surgical therapy (orchidectomy [n = 24], epididymectomy [n = 10], orchidopexy [n = 5], or hydrocelectomy [n = 1]) and, based on this experience, the authors recommended inguinal orchidectomy as the procedure of choice for testicular pain when conservative measures were unsuccessful. In this study, only 1 of the 10 patients treated with epididymectomy had significant pain relief.
In a series reported by Chen and Ball,12 epididymectomy successfully ameliorated pain symptoms in 5 of 10 patients with postvasectomy epididymal pain, 6 of 7 with epididymoorchitis, and 4 of 7 with epididymal pain associated with an epididymal cyst. Padmore and colleagues18 described a series of 27 men who underwent epididymectomy after empiric long-term and repeated courses of antibiotics and/or anti-inflammatory agents had failed, and reported patient satisfaction to be extremely high in the epididymal cyst group compared with the epididymitis/epididymalgia group (92% vs 43%).
West and colleagues13 performed 19 epididymectomies (bilateral [n = 3] and unilateral [n = 13]) in 16 patients who suffered pain after vasectomy. Of the 16 patients, 14 were reported to have excellent initial symptomatic benefit from epididymectomy. Long-term follow-up in 10 patients suggested that the benefits were durable. Poor outcome was predicted in patients with atypical symptoms, including testicular or groin pain, erectile dysfunction, and normal appearance of the epididymis on ultrasound.
Conclusion
Chronic epididymitis is a common clinical entity diagnosed and treated by practicing urologists but essentially ignored by academic urologists. It is important for the urologic community to determine the incidence and prevalence, further describe the demographic associations, and determine the socioeconomic costs associated with this condition. It would be helpful to calculate the etiology and pathogenesis of this condition by applying the same scientific rigor that is presently being employed in the evaluation of the etiology and pathogenesis of prostatitis and interstitial cystitis.
Finally, practicing urologists would benefit greatly from prospective treatment trials, evaluating the most common treatments employed (antibiotics, anti-inflammatory agents, and surgery) for this condition. A start has been made with the development of a definition of the syndrome, a classification system that may prove useful in clinical practice, and a symptom index that can be employed not only in clinical practice but also in prospective treatment trials.
Main Points.
Chronic epididymitis can be defined as symptoms of discomfort and/or pain at least 3 months in duration in the scrotum, testicle, or epididymis localized to one or each epididymis on clinical examination.
No effort has been made to determine the incidence or prevalence of this common condition; however, it must have significant socioeconomic impact, because the men affected, on average, are in the most productive years of their lives.
The etiology of chronic epididymitis can be associated with inflammatory, infectious, or obstructive factors but, in many cases, no identifiable etiology can be identified.
The Chronic Epididymitis Symptom Index, developed for a recent, prospective, case-control study, is a validated symptom index that can serve in baseline evaluation and follow-up of patients with chronic epididymitis, both in clinical practice and research treatment trials.
Many urologists suggest watchful waiting for patients in whom symptoms are mild and/or transitory. Judging from the case-control study (see above point), the most common medical therapies for chronic epididymitis are antibiotics and anti-inflammatory agents; less common are phytotherapy, anxiolytics, narcotic analgesics, acupuncture, and injection therapy.
Several studies report varying results with epididymectomy for patients with epididymitis in whom conservative and medical therapies have failed. In one study of 16 patients who suffered pain after vasectomy, 14 were reported to have excellent initial symptomatic benefit from epididymectomy.
References
- 1.Davis BE, Noble KJ, Weigel JW. Analysis and management of chronic testicular pain. J Urol. 1990;143:936–939. doi: 10.1016/s0022-5347(17)40143-1. [DOI] [PubMed] [Google Scholar]
- 2.Nickel JC, Siemens DR, Nickel KR, Downey J. The patient with chronic epididymitis: characterization of an enigmatic syndrome. J Urol. 2002;168:2132–2133. [PubMed] [Google Scholar]
- 3.Nickel JC, Beiko DT. Prostatitis, orchitis, and epididymitis. In: Schrier RW, editor. Diseases of the Kidney. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2001. pp. 1–17. [Google Scholar]
- 4.Krieger JN. Epididymitis, orchitis, and related conditions. Sex Transm Dis. 1984;11:173–181. doi: 10.1097/00007435-198407000-00012. [DOI] [PubMed] [Google Scholar]
- 5.Meares ED., Jr. Prostatitis, orchitis and epididymitis—acute and chronic. In: Schrier RW, Gottschalk CW, editors. Diseases of the Kidney. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 1996. pp. 653–667. [Google Scholar]
- 6.Mittemeyer BT, Lennox KW, Borski AA. Epididymitis: a review of 610 cases. J Urol. 1966;95:390–392. doi: 10.1016/S0022-5347(17)63468-2. [DOI] [PubMed] [Google Scholar]
- 7.Ostaszewska I, Zdrodowska-Stefanow B, Darewicz B, et al. Role of Chlamydia trachomatis in epididymitis. Part III: Clinical diagnosis. Med Sci Monitor. 2000;6:1119–1121. [PubMed] [Google Scholar]
- 8.Okadome A, Takeuchi IF, Ishii T, Haratsuka Y. Tuberculous epididymitis following intravesical bacillus Calmette-Guérin therapy. Jpn J Urol. 2002;93:580–582. doi: 10.5980/jpnjurol1989.93.580. [DOI] [PubMed] [Google Scholar]
- 9.Menke JJ, Heins JR. Epididymal-orchitis following intravesical bacillus Calmette-Guérin therapy. Ann Pharmacother. 2000;34:479–482. doi: 10.1345/aph.19212. [DOI] [PubMed] [Google Scholar]
- 10.Kirkali Z. Amiodarone-induced sterile epididymitis. Urol Int. 1988;43:372–374. doi: 10.1159/000281399. [DOI] [PubMed] [Google Scholar]
- 11.Kaklamani BG, Vaiopoulos G, Markomichelakis N, Kaklamanis P. Recurrent epididymal-orchitis in patients with Behçet’s disease. J Urol. 2000;163:487–489. doi: 10.1016/s0022-5347(05)67908-6. [DOI] [PubMed] [Google Scholar]
- 12.Chen TF, Ball RY. Epididymectomy for post-vasectomy pain: histological review. BJU Int. 1991;68:407–413. doi: 10.1111/j.1464-410x.1991.tb15362.x. [DOI] [PubMed] [Google Scholar]
- 13.West AF, Leung HY, Powell PH. Epididymectomy is an effective treatment for scrotal pain after vasectomy. BJU Int. 2000;85:1097–1099. doi: 10.1046/j.1464-410x.2000.00656.x. [DOI] [PubMed] [Google Scholar]
- 14.Luzzi GA, O’Brien TS. Acute epididymitis. BJU Int. 2001;87:747–755. doi: 10.1046/j.1464-410x.2001.02216.x. [DOI] [PubMed] [Google Scholar]
- 15.Litwin SM, McNaughton-Collins M, Fowler FJ, et al. The NIH Chronic Prostatitis Symptom Index (NIH-CPSI): development and validation of a new outcomes measure. J Urol. 1999;162:369–375. doi: 10.1016/s0022-5347(05)68562-x. [DOI] [PubMed] [Google Scholar]
- 16.Meares EM, Jr, Stamey TA. Bacteriologic localization patterns in bacterial prostatitis and urethritis. Invest Urol. 1968;5:492–518. [PubMed] [Google Scholar]
- 17.Nickel JC. The Pre and Post Massage Test (PPMT): a simple screen for prostatitis. Tech Urol. 1997;3:38–43. [PubMed] [Google Scholar]
- 18.Padmore DE, Norman RW, Millard OH. Analyses of indications for and outcomes of epididymectomy. J Urol. 1996;156:95–96. [PubMed] [Google Scholar]