

Abstract
Objective:
To describe the incidence of catastrophic head injuries in a variety of high school and college sports.
Design and Setting:
Data on catastrophic head injuries were compiled in a national surveillance system maintained by the National Center for Catastrophic Sports Injury Research. The data were compiled with the assistance of coaches, athletic trainers, athletic directors, executive officers of state and national athletic organizations, a national newspaper clipping service, professional associates of the researchers, and national sport organizations.
Subjects:
Data included all high school and college athletic programs in the United States.
Measurements:
Background information on the athlete (age, height, weight, experience, previous injury, etc), accident information, immediate and postaccident medical care, type of injury, and equipment involved. Autopsy reports were used when available.
Results:
A football-related fatality has occurred every year from 1945 through 1999, except for 1990. Head-related deaths accounted for 69% of football fatalities, cervical spinal injuries for 16.3%, and other injuries for 14.7%. High school football produced the greatest number of football head-related deaths. From 1984 through 1999, 69 football head-related injuries resulted in permanent disability. Sixty-three of the injuries were associated with high school football and 6 with college football. Although football has received the most attention, other sports have also been associated with head-related deaths and permanent disability injuries. From 1982 through 1999, 20 deaths and 19 permanent disability injuries occurred in a variety of sports. Track and field, baseball, and cheerleading had the highest incidence of these catastrophic injuries. Three deaths and 3 injuries resulting in permanent disability have occurred in female participants.
Conclusions/Recommendations:
Reliable data collection systems and continual analysis of the data can help us to reduce the number of catastrophic head-related injuries. I include additional recommendations for injury prevention.
Keywords: fatality, brain injury
Head trauma results in more fatalities than any other sport injury and is the cause of most football fatalities, but it can also be associated with other sports.1,2 Fatal head injuries have been reported in soccer, wrestling, track, baseball, and a number of other sports. The morbidity and mortality associated with traumatic brain injury have been labeled a silent epidemic because they have received remarkably little attention compared with other neurologic illnesses.3 Traumatic brain injury is common in contact sports, with an estimated 250 000 concussions occurring every year in football alone.4 Repeated concussions occurring within a short period can be fatal.5,6
Second-impact syndrome, or rapid brain swelling and herniation after a second head injury, is more common than previous reports in the medical literature have suggested.7 Between 1980 and 1991, the National Center for Catastrophic Sports Injury Research at the University of North Carolina at Chapel Hill identified 29 probable cases among football players alone.8,9 Schneider10 first described second-impact syndrome in 1973. The syndrome occurs when an athlete who sustained a head injury—often a concussion or a worse injury, such as a cerebral contusion—sustains a second head injury before symptoms associated with the first have cleared. For a catastrophic condition that has a mortality rate approaching 50% and a morbidity rate nearing 100%, prevention takes on the utmost importance.7
Guskiewicz et al11 found that football players who sustained 1 concussion in a season were 3 times more likely to sustain a second concussion in the same season compared with uninjured players. Recent statistics suggest that approximately 300 000 sport-related traumatic brain injuries or head injuries occur annually in the United States. The Centers for Disease Control and Prevention12 reported a high incidence of repeated head injuries in several sports and warned that the likelihood of serious sequelae increases with repeated head injury.
METHODS
The collection of football fatality data began in 1931, when the American Football Coaches Association initiated the First Annual Survey of Football Fatalities.8 The research has been carried out on a national level every year except for 1942 and has been conducted at the University of North Carolina at Chapel Hill since 1965. The title of the survey was changed in 1980 to the Annual Survey of Football Injury Research. The primary purpose of the research was, and still is, to make the game of football a safer and, therefore, a more enjoyable sport. As a result of these surveys, the game of football has realized many benefits with regard to rules changes and improved equipment, medical care, and coaching techniques. The survey was expanded in 1977 to include neck injuries with permanent disability and again in 1984 to include brain injuries with permanent disability. The annual survey is today known as the Annual Survey of Catastrophic Football Injuries.9 Data collection was expanded again in 1982 to include all sports at the high school and collegiate levels, and a National Center for Catastrophic Sports Injury Research was established. This expansion was related to the lack of catastrophic injury data in sports other than football, the expansion of female sports and female participation due to Title IX, and the dearth of female sport injury data.
The term catastrophic injury is defined as any severe injury incurred during participation in a school- or college-sponsored sport. Catastrophic injuries are categorized as follows:
• Fatal
• Nonfatal: permanent, severe functional disability
• Serious: no permanent functional disability but severe injury; for example, a fractured cervical vertebra without paralysis
Sport-related injuries are also considered direct or indirect.
• Direct: injuries resulting directly from participation in the skills of the sport
• Indirect: injuries caused by systemic failure as a result of exertion while participating in a sport activity or by a complication secondary to a nonfatal injury
Only direct injuries will be discussed in this paper.
Data were compiled with the assistance of coaches, athletic trainers, athletic directors, executive officers of state and national athletic organizations, a national newspaper clipping service, and professional associates of the researchers. The National Collegiate Athletic Association, National Federation of State High School Associations, and American Football Coaches Association also assisted in data collection. On receiving information concerning a possible catastrophic sports injury, contact by telephone, personal letter, and questionnaire was made with the injured player's coach or athletic director. Data collected included background information on the athlete (age, height, weight, experience, previous injury, etc), accident information, immediate and postaccident medical care, type of injury, and equipment involved. Autopsy reports were used when available. Data were collected as close to the time of injury as possible; however, as with any surveillance system, some cases were studied much later. Occasionally, a catastrophic injury is not detected until several years after the event. Furthermore, it is impossible to guarantee that every case is identified by the catastrophic surveillance system; infrequently, a case may be missed. However, every effort is made to identify injured athletes. The system is publicized within the sports medicine community and is supported by the National Collegiate Athletic Association, the National Federation of State High School Associations, and the American Football Coaches Association. The use of a national press clipping service provides a timely and economic mechanism for case identification.
In 1987, a joint endeavor was initiated with the Section on Sports Medicine of the American Association of Neurological Surgeons. The purpose of this collaboration was to enhance the collection of medical data. Dr Robert C. Cantu, Chairman of the Department of Surgery and Chief of the Neurosurgery Service at Emerson Hospital in Concord, MA, has been responsible for contacting the physician involved in each case and collecting the medical data. Dr Cantu is also a past president of the American College of Sports Medicine.
The remainder of this paper will be divided into 3 areas: (1) football head injuries that resulted in fatalities, (2) football head injuries that resulted in permanent disability or recovery, and (3) head injuries in sports other than football that resulted in fatalities, permanent disability, or recovery.
RESULTS
Football Fatalities
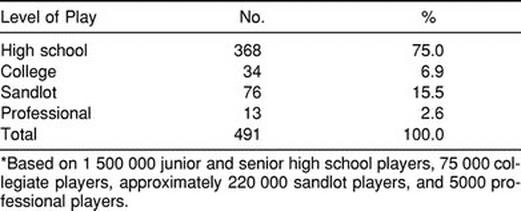
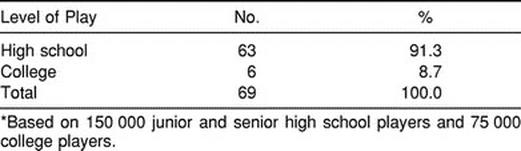
Football fatality data have been collected since 1931, but due to different data collection techniques, I will report football head fatality data from the 1945 through 1999 football seasons. Each year from 1945 through 1999, except for 1990, has produced a fatal head injury. Fatal head injuries include subdural hematomas, brain injury, fractures, and aneurysms. The year 1990 was the only year since 1931 without any record of a football fatality in all of football. There were 712 total football fatalities from 1945 through 1999. As shown in Table 1, head injuries accounted for 491 (69%), cervical spine injuries for 116 (16.3%), and other injuries for 105 (14.7%) of these fatalities. High school football produced the greatest number of football fatal head injuries when compared with college football (Table 2). It must be emphasized that there are now approximately 1 500 000 high school and middle school football players and only 75 000 college players.
Table 1.
Football Fatalities, 1945–1999*
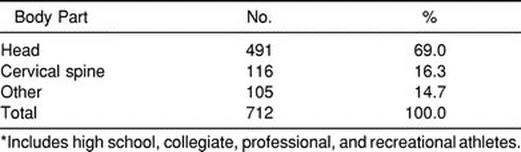
Table 2.
Football Head-Related Fatalities by Level of Play, 1945–1999*
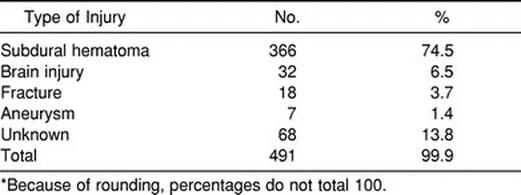
As expected, most of the fatal head injuries happened while the participant was tackling or being tackled in a game. Approximately 75% of the fatal head injuries from 1945 through 1999 were subdural hematoma injuries (Table 3), and 32 fatalities were listed as other brain injuries. If the subdural hematoma fatalities were combined with the brain fatalities, they would be responsible for more than 80% of the total number of fatal head injuries. It is plausible that a large number of the fatal head injuries listed as unknown were some type of fatal brain injury.
Table 3.
Football Head-Related Fatalities by Type of Injury, 1945–1999*
The number of fatalities increased to an all-time high in the decade 1965–1974, then steadily declined through 1985–1994 (Table 4). The decade from 1995 through 2004 is obviously not yet completed, but the preliminary findings suggest a declining trend. The increase in fatal head injuries that began in the early 1960s and continued into the early 1970s can be directly related to the skills of tackling and blocking that were being taught during those years. This period in football became known for tactics such as spearing, butt blocking, face to the numbers, and face in the chest. Players were being taught to make initial contact with the head and face into the opponent's chest. Not only did the rate of fatal head injuries increase, but a similar increase was seen in the rate of fatal cervical spine injuries. The 1976 rule change prohibiting initial contact with the head or face resulted in a dramatic decrease in both fatal head and cervical spine injuries. The number of direct football fatalities per 100 000 participants was low, except for 1968 (Table 5).
Table 4.
Football Head-Related Fatalities by Decade, 1945–1999*
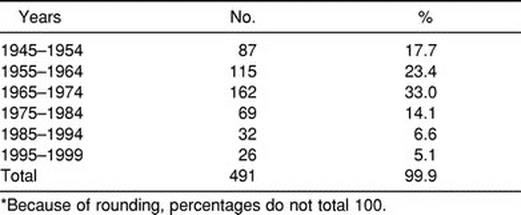
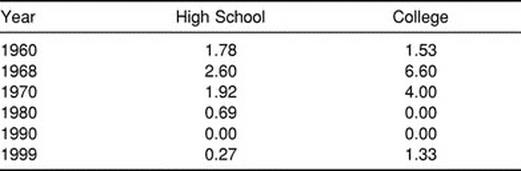
Table 5.
Incidence of Football Fatalities per 100000 Participants
Football Head Injuries Resulting in Permanent Disability or Recovery
In 1977, the National Collegiate Athletic Association initiated funding for the First Annual Survey of Catastrophic Football Injuries under the direction of the National Center for Catastrophic Sports Injury Research. Catastrophic injuries were defined as football injuries resulting in brain or spinal cord injury or head or spine fractures. All cases involved some disability at the time of the injury. Early data collection involved only spinal cord injuries, but in 1984, head injuries were included. From 1984 through 1999, there were 63 high school and 6 collegiate catastrophic head injuries (Table 6). All 69 of these injuries involved incomplete recovery. Using the previously mentioned participation numbers, the catastrophic head injury rate from 1984 through 1999 was 0.27 injuries per 100 000 high school participants. The rate for college players was 0.5 injuries per 100 000 participants. In addition to the injuries with incomplete recovery, a number of serious head injuries each year resulted in complete recovery. For comparison, during this same time span (1984 through 1999), there were 104 spine injuries in high school participants and 15 in collegiate participants. All 119 resulted in incomplete recovery.
Table 6.
Catastrophic Football-Related Head Injuries, 1984–1999*
Catastrophic Head Injuries in Other Sports
For obvious reasons, football has received the most attention in the discussion of catastrophic athletic injury data collection. Until the formation of the National Center for Catastrophic Sports Injury Research in 1982, football was the only sport for which catastrophic injury data was collected. In terms of other sports, track and field and baseball stand out as being associated with the greatest number of catastrophic head injuries (Table 7). The pole vault was associated with most of the catastrophic track and field injuries and posed a serious concern after 3 deaths in 1983. In addition to the pole-vaulting accidents, a number of catastrophic head injuries involved participants being struck by a thrown discus, shot put, or javelin. Most of the baseball injuries have been associated with the head-first slide, player collisions, or being struck by a pitched or thrown ball.
Table 7.
Catastrophic Head Injuries in Other High School and College Sports, 1982–1999*
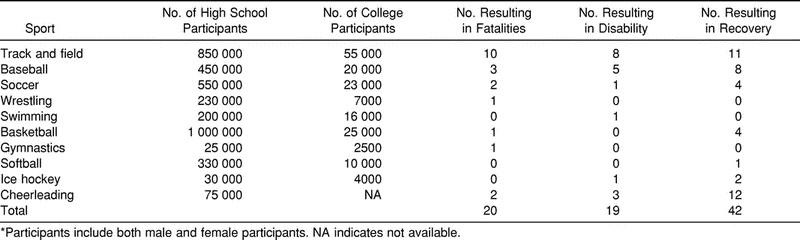
Catastrophic injuries have not been limited to male participants. Cheerleading, gymnastics, softball, field hockey, and volleyball have all been associated with fatalities or permanently disabling injuries in female participants in recent years. Cheerleading accounted for more than 50% of catastrophic injuries to female participants over the past 17 years.
DISCUSSION
Recommendations for Prevention
Catastrophic head injuries may never be totally eliminated from sport, but with reliable injury data collection systems and constant attention to prevention measures, the frequency of these injuries can be dramatically reduced. Several factors are essential for preventing these injuries: (1) Preparticipation medical examinations and medical histories must be mandatory for participants at all levels of competition. (2) Every school and college that participates in athletics should hire an athletic trainer certified by the National Athletic Trainers' Association Board of Certification, and this individual should be a regular member of the school's faculty or organization. (3) Game rules must be strictly enforced by officials, coaches, and school officials. Coaches should know and be able to teach the proper fundamental skills of the sport. Players should be taught not to make initial contact with their head or face while blocking or tackling. (4) An athlete who has experienced or shown signs of head trauma (loss of consciousness, visual disturbance, headache, dizziness, obvious disorientation, memory loss) should receive immediate medical attention and should only return to participation after first being cleared by a physician or certified athletic trainer. (5) Athletes, parents, and coaches should be educated about the signs and symptoms associated with head injury, as well as the dangers of recurrent injury and second-impact syndrome. (6) The team's certified athletic trainer must always be prepared for a possible catastrophic head injury. Everyone involved must know what to do before the injury takes place. Being prepared and knowing what to do may be the difference that prevents permanent disability. A written emergency plan should be distributed to all relevant personnel and should include an evacuation plan, available transportation, portable and open communication, and game and practice schedule awareness in local hospital emergency departments. These recommendations will not prevent injuries from happening, but they will possibly prevent serious injuries from resulting in permanent disability.
CONCLUSIONS
Data from the National Center for Catastrophic Sports Injury Research have played a major role in helping to reduce the incidence of these catastrophic sport injuries. National governing bodies have used the data extensively to identify problem areas within their sports and to implement changes. Our continued collection of data on catastrophic injuries has also allowed these changes to be evaluated. Ongoing surveillance is important because sports are continuously evolving and changing, and inexperienced coaches continue to enter the coaching profession. Catastrophic injuries are rare, but the health care professional needs to be trained and prepared to deal with these potentially serious situations. To this end, every school should strive to have routine and regular access to the services of an athletic trainer certified by the National Athletic Trainers' Association Board of Certification.
ACKNOWLEDGMENTS
This research was supported by the National Collegiate Athletic Association, the National Federation of State High School Associations, and the American Football Coaches Association.
REFERENCES
- 1.Jane JA. Head injuries. Presented at: Art and Science of Sports Medicine, University of Virginia; 1981; Charlottesville, VA. [Google Scholar]
- 2.Nelson WE, DePalma B, Gieck JH, McCue FC, Kulund DN. Intercollegiate lacrosse injuries. Physician Sportsmed. 1981;9(10):86–92. doi: 10.1080/00913847.1981.11711187. [DOI] [PubMed] [Google Scholar]
- 3.Kelly JP, Nichols JS, Filley CM, Lillehei KO, Rubinstein D, Kleinschmidt-DeMasters BK. Concussion in sport: guidelines for the prevention of catastrophic outcome. JAMA. 1991;266:2867–2869. doi: 10.1001/jama.266.20.2867. [DOI] [PubMed] [Google Scholar]
- 4.Gerberich SG, Priest JD, Boen JR, Straub CP, Maxwell RE. Concussion incidences and severity in secondary school varsity football players. Am J Public Health. 1983;73:1370–1375. doi: 10.2105/ajph.73.12.1370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gronwall D, Wrightson P. Cumulative effect of concussion. Lancet. 1975;2:995–997. doi: 10.1016/s0140-6736(75)90288-3. [DOI] [PubMed] [Google Scholar]
- 6.Saunders RL, Harbaugh RE. The second impact in catastrophic contact-sports head trauma. JAMA. 1984;252:538–539. [PubMed] [Google Scholar]
- 7.Cantu RC. Second impact syndrome: immediate management. Physician Sportsmed. 1992;20(9):14–17. [Google Scholar]
- 8.Mueller FO, Diehl JL. Annual Survey of Football Injury Research, 1931–1999. Chapel Hill, NC: American Football Coaches Association, National Collegiate Athletic Association, National Federation of State High School Associations; 2000. pp. 1–27. [Google Scholar]
- 9.Mueller FO, Cantu RC. Annual Survey of Catastrophic Football Injuries, 1977–1999. Overland Park, KS: National Collegiate Athletic Association; 2000. pp. 1–21. [Google Scholar]
- 10.Schneider RC. Head and Neck Injuries in Football: Mechanisms, Treatment and Prevention. Baltimore, MD: Williams & Wilkins; 1973. [Google Scholar]
- 11.Guskiewicz KM, Weaver NL, Padua DA, Garrett WE., Jr Epidemiology of concussion in collegiate and high school football players. Am J Sports Med. 2000;28:643–650. doi: 10.1177/03635465000280050401. [DOI] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention. Sports-related recurrent brain injuries—United States. MMWR Morb Mortal Wkly Rep. 1997;46:224–227. [PubMed] [Google Scholar]