

Abstract
Objective:
To compare the differences in the concentric hamstrings:quadriceps (H:Q) ratio among athletes in different sports at 3 velocities.
Design and Setting:
We measured the H:Q ratio of both knees using the Biodex Pro Isokinetic Device.
Subjects:
Eighty-one male and female collegiate athletes.
Measurements:
We performed analyses for sport, velocity, and side of body for each sex. To compare the means of the concentric H:Q ratios for mean peak torque and mean total work, a 2 × 3 × 4 mixed-factorial analysis of variance was computed for women and a 2 × 2 × 3 mixed-factorial analysis of variance was computed for men.
Results:
We observed no significant interactions for men and women for the concentric H:Q ratio for mean peak torque. There was a significant mean difference among velocity conditions and a significant difference for men with respect to velocity. No significant differences were found for side of body or sport.
Conclusions:
The H:Q ratio increased as velocity increased. No differences existed for the H:Q ratio for sport or side of body.
Keywords: knee, sex, concentric, eccentric
Isokinetic assessment can be used to measure torque values at several joints in the body; the knee is perhaps the joint most commonly tested. This assessment typically involves comparing the involved joint with the uninvolved joint.1 Isokinetic testing can be used to evaluate quadriceps and hamstrings muscle strength, providing a determination of the magnitude of torque generated, and subsequently, the hamstrings to quadriceps (H:Q) strength ratio.2
The H:Q ratio has been used to examine the similarity between hamstrings and quadriceps moment-velocity patterns and to assess knee functional ability and muscle balance.1,3,4 This ratio has conventionally been expressed as concentric hamstrings to quadriceps strength5,6 and recently as eccentric hamstrings to concentric quadriceps strength.7 Researchers have examined this ratio in both sexes and in different age groups and rehabilitation settings.1,6,8–21 The H:Q ratio is velocity and position dependent7 and may reflect predisposition to injury.22,23 This predisposition may result from decreased antagonist hamstrings coactivation during extension loads.24
Baratta et al24 examined antagonist musculature assisting in knee joint stability. Athletes who did not regularly exercise their hamstrings had a significant decrease in hamstrings activation compared with normal healthy subjects and athletes who regularly exercised the hamstrings during knee flexion-extension movements. Inhibiting antagonist coactivation activity allows for increased torque and efficiency during extension. It has been suggested that a highly developed quadriceps muscle contributes to decreased antagonist hamstrings coactivation, thereby increasing susceptibility to anterior cruciate ligament (ACL) injury.24
Although it is difficult to generalize, the normal H:Q ratio is considered to be 50% to 80% as averaged through the full range of knee motion, with a higher ratio at faster speeds.2,8,23 As the ratio approaches 100%, the hamstrings have an increased functional capacity for providing stability to the knee.10 This increased knee stability may reduce the possibility of an anterolateral subluxation of the tibia.4
To date, investigations have focused on evaluation of the H:Q ratio in the ACL-deficient knee.10,25,26 Although the H:Q ratio has been studied in athletes with healthy knees, many of the populations studied have been professional athletes.5,19,23,27,28 Few researchers have investigated the collegiate athletic population.16 Therefore, our purpose was to compare the differences in concentric H:Q ratio for mean peak torque (MPT) and mean total work (MTW) among athletes in different sports and right versus left limbs at 60, 120, and 180°·s−1. The velocities were chosen based on similar velocities used in previous investigations.1,3,4,10,16,22,23
METHODS
The subjects tested were 81 (26 men, 55 women) collegiate athletes with a mean age of 19.3 ± 1.32 years; mean height, 172.16 ± 1.00 cm; mean weight, 70.79 ± 11.34 kg; and mean body fat percentage, 18.65 ± 8.79%. Each subject was currently active with an intercollegiate varsity athletic team and volunteered for the study. The sports represented were men's volleyball (n = 9), women's volleyball (n = 12), men's soccer (n = 17), women's soccer (n = 10), women's basketball (n = 10), and women's softball (n = 23). A subject was disqualified for any documented history of knee ligament or meniscal damage or current injury to the thigh musculature. All procedures were approved by the Institutional Review Board at the University of Missouri-Columbia, and all subjects gave written informed consent to participate in athletics and medical screenings.
To measure the H:Q ratio, we used the Biodex Pro Isokinetic Device (Biodex Medical Systems, Shirley, NY) to perform knee concentric flexion and extension movements. We assessed MPT and MTW among men and women involved in various sports and between right and left limbs. Measurements were taken at 60, 120, and 180°·s−1.
For the testing session, subjects were seated with the powerhead orientation, powerhead tilt, and seat orientation set at 0°. The seatback tilt was set at 15°. Knee axis of rotation was determined by a line drawn in the sagittal plane through the femoral condyles. The subject was restrained when seated in the chair by 2 straps across the torso in a criss-cross fashion and by a strap placed across the thigh midway between the anterior superior iliac spine and superior border of the patella. The standard knee-attachment device was secured to the leg so that the inferior border of the pad was placed on the superior border of the medial malleolus.
Once the subject was secured in the chair, the range-of-motion limits were determined via goniometry and set. The starting position was 90° of knee flexion, and the endpoint was 0° of full knee extension. Gravity correction was performed for each limb before testing in order to reduce the risk of inaccurate data. Failure to correct for the effects of gravity when measuring the H:Q ratio may result in an overestimation of the ratio. This overestimation is due to a perceived increase in the strength of the hamstrings relative to the quadriceps.29 Once the subject was seated and secured, he or she performed 5 repetitions at 60°·s−1, 10 repetitions at 120°·s−1, and 15 repetitions at 180°·s−1. Before the isokinetic test, subjects performed 5 repetitions at 60°·s−1 as a warm-up. A 1-minute rest period was provided between velocities, and at the conclusion of the 180°·s−1 set, the opposite leg was tested. Before the testing sessions, subjects were allowed to practice by performing several light contractions until they demonstrated proper technique.27,30
Statistical Analysis
Analyses were performed for sport, velocity, and side of body for each sex. For women, a 2 × 3 × 4 mixed-factorial analysis of variance (ANOVA) was computed to compare the means of the concentric H:Q ratios for MPT and MTW. The 3 independent variables included 2 within-subjects factors (side of body [right or left] and velocity [60, 120, or 180°·s−1]) and a between-subjects factor of sport (volleyball, soccer, softball, or basketball). For men, a 2 × 2 × 3 mixed-factorial ANOVA was computed with 2 within-subjects factors, side of body and velocity, and the between-subjects factor of sport (volleyball or soccer). We used the generalized least squares procedure from the Statistical Package for Social Sciences31 (version 8.0 for Windows, SPSS Inc, Chicago, IL) to calculate the ANOVAs. For all analyses, the alpha level was set at P = .05.
To test for basic assumptions, the Mauchly test of sphericity was computed for the within-subjects factors of velocity and side of body. We used this test to analyze the similarity of the treatment differences across the 3 velocity conditions for all subjects.
Results
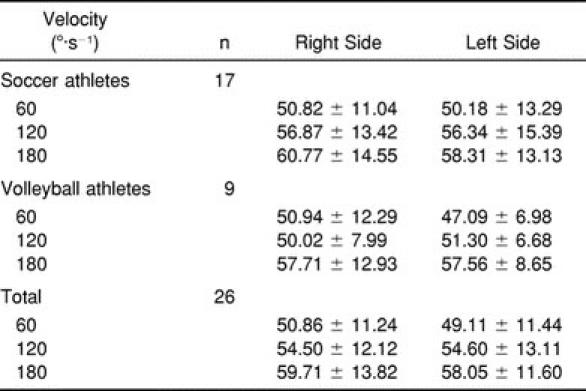
The descriptive statistics for side of body across the 3 velocities and sport are presented in Tables 1 through 4 for women and men. For the Mauchly test of sphericity, the concentric H:Q ratios for MPT for women for velocity and velocity × side of body conditions were significantly different (P < .05) (Mauchly Wspeed = 831; Mauchly Wspeed×side = .571). For men, the concentric H:Q ratios for MPT and MTW were significantly different for velocity (MPT, Mauchly Wspeed = .717; MTW, Mauchly Wspeed = 16.014). We used the Greenhouse-Geiser statistic to adjust for the degrees of freedom.
Table 1.
H:Q Ratio of Right and Left Legs for Mean Peak Torque by Sport and Velocity (°·s−1) in Women
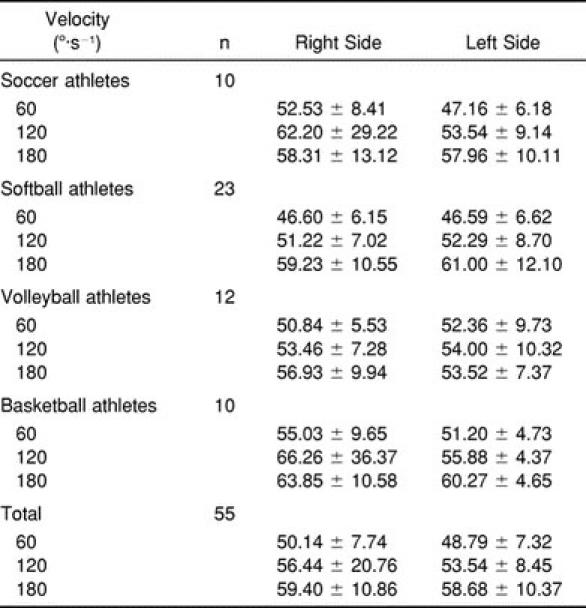
Table 4.
H:Q Ratio of Right and Left Legs for Mean Total Work by Sport and Velocity (°·s−1) for Men
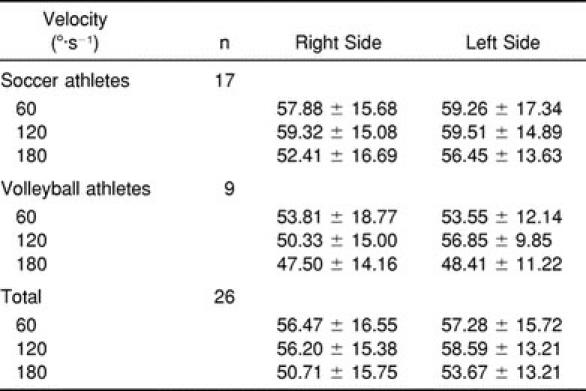
Table 2.
H:Q Ratio of Right and Left Legs for Mean Total Work by Sport and Velocity (°·s−1) in Women
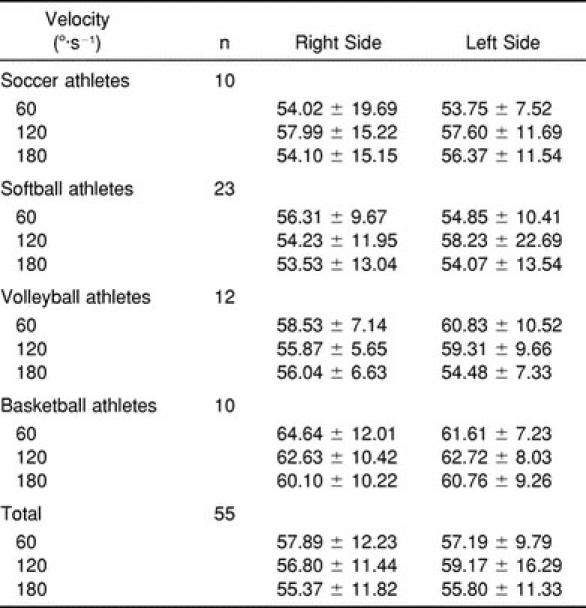
Table 3.
H:Q Ratio of Right and Left Legs for Mean Peak Torque by Sport and Velocity (°·s−1) in Men
For men and women, no significant interactions were found for concentric H:Q ratio for MPT. The analysis of the main effects revealed only a significant mean difference among velocity conditions (women: F1.71,87.22 = 20.962, P = .000; men: F1.56,37.43 = 15.314, P = .000). Pairwise comparisons for both groups indicated that 180°·s−1 was associated with significantly higher MPT values than 120 and 60°·s−1, and 120°·s−1 was associated with significantly higher MPT values than 60°·s−1 (Figures 1 and 2). No significant differences were found for side of body or sport. Additionally, we noted no significant interactions or main effects for concentric H:Q ratio for MTW for women. However, a significant difference was found for men with respect to velocity (F1.56,37.43 = 15.314, P = .000). Analysis of the pairwise comparisons indicated that 120°·s−1 was associated with significantly higher MTW values than 180°·s−1 (Figure 3).
Figure 1.

Women's mean peak torque H:Q ratios. Values were significantly higher at 180°·s−1 than at 120 and 60°·s−1 and significantly higher at 120°·s−1 than at 60°·s−1.
Figure 2.

Men's mean peak torque H:Q ratios. Values were significantly higher at 180°·s−1 than at 120 and 60°·s−1 and significantly higher at 120°·s−1 than at 60°·s−1.
Figure 3.

Men's mean total work H:Q ratios. Values were significantly higher at 120°·s−1 than at 180°·s−1.
DISCUSSION
Isokinetic testing of the H:Q ratio provides a quantitative measurement of torque from agonist and antagonist muscle contraction surrounding the knee joint.15 This ratio has also been examined as a possible screening tool for predisposition to injury.23 When the knee is injured, the H:Q ratio is often used as a rehabilitative goal due to the importance of the flexor-extensor strength balance in overall knee stabilization.16 Reduced function of the antagonist hamstrings due to activities that emphasize loads on the knee extensors may result in muscular imbalances between the hamstrings and quadriceps, thereby possibly predisposing athletes to injury. This predisposition may be due to the surrounding ligamentous structures supporting most of the imposed load and decreased antagonist hamstrings coactivation during extension loads.24,32
Several investigators have examined the H:Q ratio after ACL injury, using different test velocities and examining the consequences of proprioception relative to the H:Q ratio after ACL injury.4,6,10,25,33 In a comparision of injured versus noninjured knees at 2 test velocities, Lund-Hanssen et al6 reported a higher H:Q ratio in injured knees at the higher velocity (240°·s−1) compared with uninjured knees. However, at the lower velocity (60°·s−1), no difference was noted between groups. This difference at the higher test velocity was attributed to a decrease in quadriceps muscle strength in the injured group due to rehabilitation; fast-twitch muscle fiber atrophy may have been caused due to alterations in exercise patterns during rehabilitation.6 Kannus25 also reported a higher H:Q ratio in injured knees at higher speeds (180°·s−1). This led to the conclusions that, in injured knees, the H:Q ratio increases at higher speeds, in part due to quadriceps femoris muscle weakness, and H:Q ratios of the opposite limb should be used as rehabilitative goals. However, the opposite limb ratio should only be used if that limb is not injured. An injured opposite limb may result in misleading H:Q ratios.25
Corrigan et al33 examined proprioception in the ACL-deficient knee, including correlating the position sense of the knee with the H:Q ratio. No correlations were found between position sense and H:Q ratios for the control (non-ACL-deficient) group. However, in the study group, the ACL-deficient knee did significantly correlate with the H:Q ratio for both threshold of perception of movement (joint angle is slowly altered less than 0.5°·s−1) and position sense (ability to reproduce the angle in which the joint had been placed before being moved). No such correlations were found for the non-ACL-deficient knee in the study group.33
In the ACL-deficient knee, hamstrings dominance can aid in stabilization by acting as a synergist to the normal ACL. This stability is of particular importance during high-speed activity because, it has been suggested, instability at slow speeds is well compensated for, while compensation decreases as speeds increase. Posterior stabilization about the knee through proper hamstrings conditioning may assist in the reduction of anterolateral translation and, thereby, reduce the incidence of ACL injury or reinjury.33 However, rehabilitative goals should focus on obtaining an optimal H:Q ratio, not deemphasizing quadriceps strength in knee function.
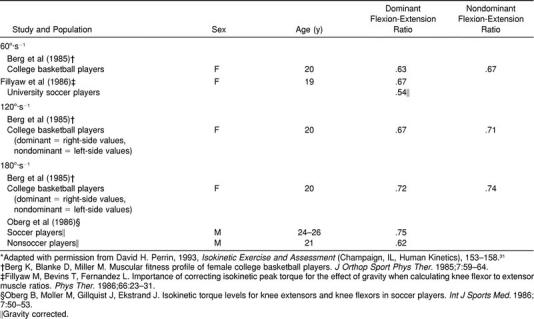
In our investigation using healthy knees, as velocity increased, the H:Q ratio increased. The increased H:Q ratio with increased velocity is consistent with the findings of Kannus25 in injured knees and with those of Croce et al,22 who reported increases in the H:Q ratio from 61.0 ± 14.3% at 60°·s−1 to 62.0 ± 14.7% at 90°·s−1 in nondisabled, sedentary controls. Comparatively, our subjects had H:Q ratios of 49.8% at 60°·s−1, 53.6% at 120°·s−1, and 58.6% at 180°·s−1 for men and 50.3% at 60°·s−1, 56.1% at 120°·s−1, and 58.9% at 180°·s−1 for women. These ratios are lower than those reported by Bennell et al23 at 60°·s−1 and 180°·s−1, yet similar to those of Aagaard et al3 at 120°·s−1. Table 5 presents selected normative values for the H:Q ratio at similar velocities.29
Table 5.
Selected Normative Values for the H:Q Ratio at Velocities of 60°, 120°, and 180°·s−1*
We found no differences in the H:Q ratio between athletes in different sports. Zakas et al28 reported no significant differences in H:Q ratio among different divisions of basketball and soccer players at 60°·s−1 and 180°·s−1. However, Read and Bellamy19 noted differences in the H:Q ratios among tennis, squash, and track athletes. In each case, the authors attributed the findings to training adaptations acquired by the subjects for their respective sports. The finding of no differences in the H:Q ratios among athletes in different sports in our study may be associated with training adaptations and level of competition.
Zakas et al28 suggested that the strength and flexibility associated with game demands in sport, specifically basketball and soccer, may result in specific training adaptations that produce similar H:Q ratios among these 2 sports. Bennell et al,23 in their study of Australian rules footballers, suggested that differences in H:Q ratios may be due to level of competition. The sports represented in our study (volleyball, soccer, basketball, and softball) all require similar movements (running, jumping, cutting, deceleration, and acceleration) to adequately perform the chosen activity. In addition, each subject participated in a collegiate setting, with each sport in the same division. These factors of training adaptations and level of competition may be responsible for the lack of differences in the H:Q ratios among the sports examined. However, coaches, strength and conditioning professionals, and athletic trainers should exercise caution when incorporating training and conditioning programs for similar sports at any level. Attention must be given to proper muscle balance between agonist and antagonist muscle groups due to a possible increased risk of injury as a result of muscular imbalance.24
Muscular imbalance has been shown to affect injury patterns in female athletes. Before training, female athletes exhibit imbalances between hamstrings and quadriceps muscle strength. When comparing the incidence of knee injury in male athletes, untrained female athletes were 4.8 to 5.8 times more likely and trained female athletes were 1.3 to 2.4 times more likely to suffer a knee injury than male athletes.32 Through neuromuscular training, a reduction in knee ligament injuries may be possible because of biomechanical effects (decreased landing forces and adduction-abduction moments) and physiologic effects (decreased estrogen levels and increased H:Q strength ratios).32
Female athletes tend to be quadriceps dominant, contracting the quadriceps muscles in response to anterior tibial translation, versus nonathletes, who tend to contract the hamstrings. If the hamstrings are ignored during training, quadriceps dominance in the trained female athlete influences the H:Q ratio when compared with the nonathlete. To reduce the incidence of knee injury in female athletes, conditioning should include measures to increase the H:Q ratio and decrease abduction-adduction moments.32
Side-to-side differences in muscle strength typically are expressed as differences between dominant and nondominant sides,1,27,34 particularly in uninjured subjects. We found no differences between right and left or dominant and nondominant limbs. These findings are in agreement with those of Holmes and Alderink,1 Gur et al,27 and Calmels et al.34 Leg dominance has been defined as the preferred versus nonpreferred leg34 or the leg preferred for kicking.22,27,35 It is possible that specific loads placed on the lower extremities in these athletes involved in different sports were sufficient to maintain similar strength on both sides.
The H:Q ratio can be used to examine similarities between quadriceps and hamstrings moment-velocity patterns with isokinetic testing. This ratio, however, is velocity dependent, as evidenced by the increase in the H:Q ratio as velocity increases. When using this ratio as an evaluative tool, the velocity-dependent changes in the H:Q ratio must not be ignored as this may lead to inaccurate evaluations of leg strength. As a rehabilitative goal, the H:Q ratio for the injured limb should be compared with that of the uninjured limb. Differences in the H:Q ratios between athletes in different sports may depend on the chosen sport, the level of competition, or both, while sports with similar lower limb demands and similar competitive levels may yield no differences. Differences in limb dominance with the conventional H:Q ratio may not occur because specific loads imposed with training and competition may be similar for both limbs.
If the H:Q ratio is to be used as a possible screening tool for susceptibility to injury,23 future investigations of the H:Q ratio should focus on the conventional H:Q ratio and that proposed by Aagaard et al7 relating to the incidence of injury and recovery from injury. Preseason assessments should include a baseline evaluation of the H:Q ratio with the subsequent tracking of injuries to the lower extremities.
ACKNOWLEDGMENTS
We sincerely thank Robert Schall, PT, of Peak Performance Physical Therapy and Sports Medicine of Columbia, Columbia, MO, for the use of the Biodex Pro isokinetic device for testing and Ms Robin Audesse, of the University of Southern Maine Department of Sports Medicine, for her assistance in compiling the data and preparing the manuscript.
REFERENCES
- 1.Holmes JR, Alderink GJ. Isokinetic strength characteristics of the quadriceps femoris and hamstrings muscles in high school students. Phys Ther. 1984;64:914–918. doi: 10.1093/ptj/64.6.914. [DOI] [PubMed] [Google Scholar]
- 2.Grace TG, Sweetser ER, Nelson MA, Ydens LR, Skipper BJ. Isokinetic muscle imbalance and knee-joint injuries: a prospective blind study. J Bone Joint Surg Am. 1984;66:734–740. [PubMed] [Google Scholar]
- 3.Aagaard P, Simonsen EB, Trolle M, Bangsbo J, Klausen K. Isokinetic hamstring/quadriceps strength ratio: influence from joint angular velocity, gravity correction and contraction mode. Acta Physiol Scand. 1995;154:421–427. doi: 10.1111/j.1748-1716.1995.tb09927.x. [DOI] [PubMed] [Google Scholar]
- 4.Li RCT, Maffulli N, Hsu YC, Chan KM. Isokinetic strength of the quadriceps and hamstrings and functional ability of anterior cruciate deficient knees in recreational athletes. Br J Sports Med. 1996;30:161–164. doi: 10.1136/bjsm.30.2.161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Aagaard P, Simonsen EB, Beyer N, Larsson B, Magnusson P, Kjaer M. Isokinetic muscle strength and capacity for muscular knee joint stabilization in elite sailors. Int J Sports Med. 1997;18:521–525. doi: 10.1055/s-2007-972675. [DOI] [PubMed] [Google Scholar]
- 6.Lund-Hanssen H, Gannon J, Engebretsen L, Holen K, Hammer S. Isokinetic muscle performance in healthy female handball players and players with a unilateral anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 1996;6:172–175. doi: 10.1111/j.1600-0838.1996.tb00085.x. [DOI] [PubMed] [Google Scholar]
- 7.Aagaard P, Simonsen EB, Magnusson SP, Larsson B, Dyhre-Poulsen P. A new concept for isokinetic hamstring:quadriceps muscle strength ratio. Am J Sports Med. 1998;26:231–237. doi: 10.1177/03635465980260021201. [DOI] [PubMed] [Google Scholar]
- 8.Raunest J, Sager M, Burgener E. Proprioceptive mechanisms in the cruciate ligaments: an electromyographic study on reflex activity in the thigh muscles. J Trauma. 1996;41:488–493. doi: 10.1097/00005373-199609000-00017. [DOI] [PubMed] [Google Scholar]
- 9.Aune AK, Ekeland A, Nordsletten L. Effect of quadriceps or hamstrings contraction on the anterior shear force to anterior cruciate ligament failure: an in vivo study in the rat. Acta Orthop Scand. 1995;66:261–265. doi: 10.3109/17453679508995538. [DOI] [PubMed] [Google Scholar]
- 10.Harter RA, Osternig LR, Standifer LW. Isokinetic evaluation of quadriceps and hamstrings symmetry following anterior cruciate ligament reconstruction. Arch Phys Med Rehabil. 1990;71:465–468. [PubMed] [Google Scholar]
- 11.Stafford MG, Grana WA. Hamstring/quadriceps ratios in college football players: a high velocity evaluation. Am J Sports Med. 1984;12:209–211. doi: 10.1177/036354658401200308. [DOI] [PubMed] [Google Scholar]
- 12.Hislop HJ, Perrine JJ. The isokinetic concept of exercise. Phys Ther. 1967;47:114–117. [PubMed] [Google Scholar]
- 13.Boden BP, Garrett WE., Jr Mechanisms of injuries to the anterior cruciate ligament. Med Sci Sports Exerc. 1996;28:S26. [Google Scholar]
- 14.Moul JL, Robinson LK, Apke T. Differences in selected predictors of anterior cruciate ligament tears between male and female basketball players. Med Sci Sports Exerc. 1996;28:S27. [PMC free article] [PubMed] [Google Scholar]
- 15.Snow CJ, Cooper J, Quanbury AO, Anderson JE. Antagonist cocontraction of knee extensors during constant velocity muscle shortening and lengthening. J Electromyogr Kinesiol. 1995;5:185–192. doi: 10.1016/1050-6411(95)00007-m. [DOI] [PubMed] [Google Scholar]
- 16.Holm I, Ludvigsen P, Steen H. Isokinetic hamstrings/quadriceps ratios: normal values and reproducibility in sport students. Isokinetics Exerc Sci. 1994;4:141–145. [Google Scholar]
- 17.Kuhn S, Gallagher A, Malone T. Comparison of peak torque and hamstring/quadriceps femoris ratios during high-velocity isokinetic exercise in sprinters, cross-country runners, and normal males. Isokinetics Exerc Sci. 1991;1:138–145. [Google Scholar]
- 18.Moss CL, Wright PT. Comparison of three methods of assessing muscle strength and imbalance ratios of the knee. J Athl Train. 1993;28:55–58. [PMC free article] [PubMed] [Google Scholar]
- 19.Read MTF, Bellamy MJ. Comparison of hamstring/quadriceps isokinetic strength ratios and power in tennis, squash and track athletes. Br J Sports Med. 1990;24:178–182. doi: 10.1136/bjsm.24.3.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Morris A, Lussier L, Bell G, Dooley J. Hamstring/quadriceps strength ratios in collegiate middle-distance and distance runners. Physician Sportsmed. 1983;11(10):71–77. doi: 10.1080/00913847.1983.11708658. [DOI] [PubMed] [Google Scholar]
- 21.Laird DE. Comparison of quad to ham strength ratios of an intercollegiate soccer team. Athl Train. 1981;16:66–67. [Google Scholar]
- 22.Croce RV, Pitetti KH, Horvat M, Miller J. Peak torque, average power, and hamstrings/quadriceps ratios in nondisabled adults and adults with mental retardation. Arch Phys Med Rehabil. 1996;77:369–372. doi: 10.1016/s0003-9993(96)90086-6. [DOI] [PubMed] [Google Scholar]
- 23.Bennell K, Wajswelner H, Lew P, et al. Isokinetic strength testing does not predict hamstrings injury in Australian Rules footballers. Br J Sports Med. 1998;32:309–314. doi: 10.1136/bjsm.32.4.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Baratta R, Solomonow M, Zhou BH, Letson D, Chuinard R, D'Ambrosia R. Muscular coactivation: the role of the antagonist musculature in maintaining knee stability. Am J Sports Med. 1988;16:113–122. doi: 10.1177/036354658801600205. [DOI] [PubMed] [Google Scholar]
- 25.Kannus P. Ratio of hamstrings to quadriceps femoris muscles' strength in the anterior cruciate ligament insufficient knee: relationship to long-term recovery. Phys Ther. 1988;69:961–965. doi: 10.1093/ptj/68.6.961. [DOI] [PubMed] [Google Scholar]
- 26.Kramer J, Nusca D, Fowler P, Webster-Bogaert S. Knee flexor and extensor strength during concentric and eccentric muscle actions after anterior cruciate ligament reconstruction using the semitendinosus tendon and ligament augmentation device. Am J Sports Med. 1993;21:285–291. doi: 10.1177/036354659302100220. [DOI] [PubMed] [Google Scholar]
- 27.Gur H, Akova B, Punduk Z, Kucukoglu S. Effects of age on the reciprocal peak torque ratios during knee muscle contractions in elite soccer players. Scand J Med Sci Sports. 1999;9:81–87. doi: 10.1111/j.1600-0838.1999.tb00213.x. [DOI] [PubMed] [Google Scholar]
- 28.Zakas A, Mandroukas K, Vamvakoudis E, Christoulas K, Aggelopoulou N. Peak torque of quadriceps and hamstrings muscles in basketball and soccer players of different divisions. J Sports Med Phys Fitness. 1995;35:199–205. [PubMed] [Google Scholar]
- 29.Perrin DH. Isokinetic Exercise and Assessment. Champaign, IL: Human Kinetics; 1993. pp. 154–157. [Google Scholar]
- 30.Horvat M, Croce R, Pitetti KH, Fernhall B. Comparison of isokinetic peak force and work parameters in youth with and without mental retardation. Med Sci Sports Exerc. 1999;31:1190–1195. doi: 10.1097/00005768-199908000-00017. [DOI] [PubMed] [Google Scholar]
- 31.Norusis MJ. SPSS Base 8.0 Application Guide. Chicago, IL: SPSS; 1998. [Google Scholar]
- 32.Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27:699–705. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 33.Corrigan JP, Cashman WF, Brady MP. Proprioception in the cruciate deficient knee. J Bone Joint Surg Br. 1992;74:247–250. doi: 10.1302/0301-620X.74B2.1544962. [DOI] [PubMed] [Google Scholar]
- 34.Calmels PM, Nellen M, van der Borne I, Jourdin P, Minaire P. Concentric and eccentric isokinetic assessment of flexor-extensor torque ratios at the hip, knee, and ankle in a sample population of healthy subjects. Arch Phys Med Rehabil. 1997;78:1224–1230. doi: 10.1016/s0003-9993(97)90336-1. [DOI] [PubMed] [Google Scholar]
- 35.Rosene JM, Fogarty TD. Anterior tibial translation in collegiate athletes with normal anterior cruciate ligament integrity. J Athl Train. 1999;34:93–98. [PMC free article] [PubMed] [Google Scholar]