

Abstract
Objective:
To describe the current roles and responsibilities of program directors of athletic training education programs accredited by the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and to address the dilemmas of program directors' credibility with student athletic trainers, tenure and promotion, and clinical involvement in athletics.
Design and Setting:
We sent a survey to all program directors who direct CAAHEP athletic training education programs.
Subjects:
Eighty-three of 113 program directors of undergraduate programs participated in the study—a response rate of 73.4%.
Measurements:
The survey consisted of demographic data: degree, age, major, years of experience as program director, and route to certification and questions concerning title, job responsibilities, expectations, and academic appointment.
Results:
Most respondents (72%) indicated that their title was program director, and they had a median of 9 years of experience. Sixty-two percent had been certified as an athletic trainer for a median of 18.5 years. Forty-three percent had doctoral degrees and held the rank of assistant professor. Ninety-six percent indicated teaching was the primary duty and expectation of their program director's position.
Conclusions:
The dilemmas of tenure and promotion, decreased clinical involvement, and student athletic trainers' perceptions of program directors remain problematic. The dilemmas still exist as they did 12 years ago and are becoming more involved due to educational reform. Program directors must be able to communicate their roles and responsibilities to their administrators.
Keywords: curriculum director, CAAHEP, athletic training
As early as 1981, program directors (PDs) of athletic training education programs in colleges and universities were described as both clinicians and educators.1–3 Their clinical work was predominately the care of student-athletes in intercollegiate athletics, and the education portion involved teaching classes and providing hands-on instruction in the athletic training room. Leard et al2 described the PD position not only as a clinician and educator but also as a faculty member, recruiter of students, supervisor of clinical assignments, coordinator of educational experience, and liaison between the athletic training curriculum and the accrediting agency. In 1988, Perrin and Lephart3 perceived that PDs were facing several dilemmas. These dilemmas were possibly forcing PDs to make choices between traditional roles as clinicians and the emerging roles of educators. The dilemmas the PDs faced included classroom credibility with student athletic trainers (SATs) when they were actually spending less time in the intercollegiate athletics clinical setting. This dilemma in turn produced a quandary of “career frustration,” wherein the PDs' love and concern for student-athletes, which was the primary reason for becoming an athletic trainer, now was thwarted by limited contact with student-athletes.2,3 Also, how would clinical instruction be evaluated with regard to tenure and promotion? Was it service or teaching, or could it be viewed as research?
In the past 20 years, the PD position has undergone significant changes in administrative responsibilities and institutional expectations. Since the National Athletic Trainers' Association (NATA) approval process began in the early 1970s to the current Commission on Accreditation of Allied Health Education Programs (CAAHEP) process, the standard for the PD is described as “a member of the teaching faculty and 3 years of experience as an NATA-certified athletic trainer.”4,5 (The terms Program Director and Curriculum Director are used interchangeably. However, Program Director is the proper title to reflect the terminology in the CAAHEP standards.) According to Staurowsky and Scriber,6 the PD position has become a “time-intensive occupation.” Furthermore, “PDs are set apart from their faculty colleagues in other disciplines by virtue of the diverse nature of their appointments.”6
With the growth of athletic training education programs in colleges and universities, the demand for a highly qualified faculty member to serve as PD and fill the multiple roles and responsibilities of the position is important and yet problematic. The problem is that the position of PD has been evolving for years, and it has become an occupation within higher education carrying multiple roles and responsibilities. The position is difficult to define because of its complexity. It is important to “explore the distinctions among PDs” to further understand, explain, and justify the professional role in higher education.6 A literature review since 1980 produced only a few studies that documented and described the changing roles, responsibilities, and distinctions among PDs.1,3,6,7 Our purpose was to investigate and describe the current status of the PDs' roles and dilemmas first described by Perrin and Lephart in 1988.
METHODS
In the fall of 1999, we conducted a literature review to investigate workload and position-related issues of the PDs of athletic training education programs. The literature review guided the conceptual formulation of the survey instrument. For this project, we extracted data from the survey instrument in order to address and compare the roles and dilemmas as described by Perrin and Lephart3 in 1988. The entire survey was constructed to elicit responses in the areas of (1) demographics (ie, age, experience, sex, ethnicity, major, and avenue to certification); (2) professional appointment (ie, title, roles, assignment); (3) PD position (ie, duties and responsibilities, institutional expectations); (4) reasons for becoming a PD; (5) reasons for leaving the PD position; (6) most beneficial and most satisfying aspects of the position; (7) least beneficial and least satisfying aspects of the position; and (8) general issues not addressed in previous questions.
The survey included closed-ended demographic questions. To elicit responses in the areas of (2) professional appointment and (3) PD position, subjects were asked to check all that applied. Subjects were asked to provide 2 responses for each of the open-ended questions (reasons for becoming a PD, reason for leaving the position, most beneficial and most satisfying aspects of the position, least beneficial and least satisfying aspects of the position, and general issues not previously addressed).
A panel of experts consisting of 5 professionals from athletic training, health education, and sport management analyzed content validity. The panel reviewed the survey for content, clarity, whether questions would provide the needed data, length of the survey, question order, relevance, and ambiguity. The panel recommended minor editing and grammatic changes, which were incorporated into the survey instrument. The survey focused on collecting descriptive data and was determined sufficient to yield reliable and valid data; therefore, a pilot study was not conducted. The Human Subjects Committee at Southern Illinois University approved the survey instrument.
The PDs' names, addresses, and academic ranks were obtained from the NATA Web site in which program information is updated regularly, ensuring accuracy. The survey was mailed to all PDs of the 114 CAAHEP-accredited athletic training education programs at the time of this study. A coauthor of this article (S.A.P.) did not participate in the study; thus, the sample size was adjusted to 113.
Each PD was asked to complete the survey to the best of his or her ability and return the completed questionnaire in a self-addressed, stamped envelope that was provided in the initial mailing. Subjects who had not responded within a timely manner were sent a reminder through electronic mail.
Subjects
The subjects for this study were 83 PDs from CAAHEP-accredited undergraduate athletic training programs in the United States. The sample consisted of 51 men and 31 women; on one survey the question of sex was not answered.
Statistical Analysis
The data were analyzed using simple descriptive statistics: percentages and median distributions. Medians were reported to find the 50th percentile of the data set for age, years of experience as a certified athletic trainer, and years of experience as a PD. The statistical median best represented the data set by dividing the data into 2 equal halves.
RESULTS
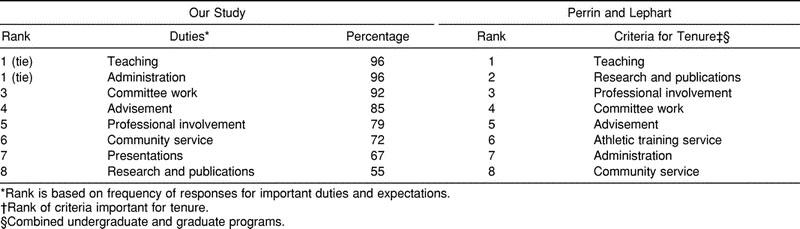
Eighty-three of 113 PDs returned the survey, yielding a 73.4% response rate. After the initial mailing, 74 surveys were returned. An additional 9 surveys were received after we sent a follow-up reminder. The median age of the respondents was 42 years. The vast majority of the respondents, 90%, had been physical education or physical education and health education majors. Fifty-two percent pursued the accredited/approved route and 47% pursued the internship route to certification; 2 respondents did not answer this question. According to information found on the NATA Web site, 43% held doctorate degrees.8 The median number of years of professional experience as a certified athletic trainer was 18.5 years, with a median of 9 years as a PD (Table 1). Seventy-seven percent shared an appointment with athletics. A total of 42% were clinically active in the athletic training room. Also, 17% of the PDs traveled with athletic teams as a duty. Ninety-six percent listed teaching and administrative tasks as a primary duty. As for the university's expectations of the PD, 92% indicated committee work and 72% indicated community service (Table 2). Fourteen percent of the PDs also held the position of head athletic trainer, while 27% were assistant athletic trainers.
Table 1.
Program Directors' Demographics Compared with Perrin and Lephart (1988)3
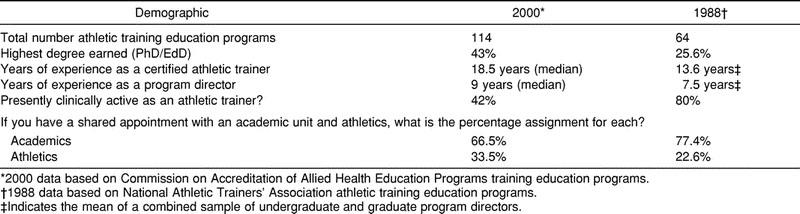
Table 2.
Program Directors' Duties and Expectations Compared with Perrin and Lephart3 by Rank
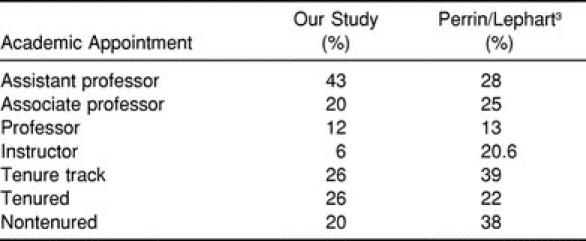
Most of the respondents (72%) indicated that their title included PD. In addition to the PD title, 43% had the title and rank of assistant professor. Twenty-six percent had already received tenure (Table 3).
Table 3.
Nature of Program Directors' Academic Appointments Compared with Perrin and Lephart3
DISCUSSION
Several dilemmas that faced PDs in 1988 are similar to the dilemmas that we have found in our research on PDs today3: tenure and promotion, student athletic trainers' perceptions of PDs, personal quandaries surrounding clinical involvement with student-athletes, and personal and family time.
Traditionally, athletic training education programs have been referred to as minors, concentrations, emphases, or specializations as part of the larger physical education program. The trend within athletic training education appears to be away from these traditional curriculums to the development of and emphasis on stand-alone majors according to the proposed CAAHEP standards. This emphasis, along with PDs' qualifications, may be the reasons that colleges and universities are hiring faculty on tenure-track appointments with both athletic training certification and a PhD, EdD, or equivalent. A content analysis of the NATA Position Vacancy Notice from November 1999 to June 20009 found 42 PD position announcements that indicated a doctoral degree was preferred. Of those positions, 14 were tenure-track appointments. With the possible trend in hiring PDs with terminal degrees on tenure-track appointments, it is even more important for PDs to understand the tenure and promotion (T&P) process. Perrin and Lephart3 found that 25.6% of NATA-approved undergraduate PDs had doctoral degrees, as compared with 43% of CAAHEP-accredited undergraduate PDs in our study.
Perrin and Lephart3 indicated that, depending on the size of the college and university, each of the T&P areas (teaching, research, and service) may be accorded different weights. Generally, each institution adheres to a T&P process that involves a probationary period. In a typical case scenario at University X, faculty are reviewed annually by the department chairperson or personnel committee and the dean of the college. They are directed in the preparation of a tenure dossier and are evaluated on the progress made in each of the 3 T&P areas. After the third year, the tenured faculty, chairperson, and dean of the college conduct a mock tenure review to assess the progress made in all 3 areas. In the sixth year, a tenure dossier is finalized and submitted for review at the department level and then forwarded to the faculty norms committee, dean, president, and board of trustees for the final decision on tenure.
Teaching at colleges and universities may be viewed as the most important of the 3 T&P areas, depending upon the institution. Perrin and Lephart3 found that PDs ranked teaching as the most important criterion for tenure. In our study, 96% of all respondents were responsible for teaching athletic training courses (Table 2). Good to excellent ratings on courses taught by PDs are expected. Evaluation by SATs of clinical instruction is also necessary. Faculty “peer” evaluation of the PD's performance in the classroom and clinical setting should also be included to complete the teaching evaluation process.
Research appears to be an important area in the T&P process in many institutions. PDs are expected to make presentations and publish articles in peer-reviewed journals. The publication requirement may be one article per year or more, depending on the college or university T&P criteria. Presentations at local, state, district, or national meetings or workshops are also part of the research area. In our study, 55% of the respondents perceived publishing as a college or university expectation, and 67% listed presentations as a college or university expectation. Perrin and Lephart3 ranked research and publication second and professional involvement third as expectations (Table 2).
There may also be an argument for clinical instruction as a viable research activity. If this is the case, clinical instruction techniques must be validated, presented, and published. One way to incorporate research into the PD's clinical instruction is through “systematic observation,” which is used extensively in the teaching profession. The techniques of “observing and recording behavior” and competency evaluation have been used successfully in documenting teaching; thus, the reliability is well documented.10 This method of objective evaluation can easily be incorporated and is useful in identifying problems that ultimately can change clinical instruction and practices. PDs may write scholarly papers on the uses and the effects of these methods in clinical education. Such papers can be presented at professional meetings or conferences and published in discipline-specific journals.
Service is an integral part of the T&P process but may be considered of less importance in relation to the teaching and research areas, depending on the institution. Our study found that PDs perceived professional involvement (79%) and community service (72%) as important college and university expectations (Table 2). Service can be further delineated into several areas, such as national, district, or state or university, college, department, or community. The PD must determine how service is viewed within the T&P process and should educate members of the T&P committee and administrators as to its importance. Finally, advising students may also be perceived by college and university administrators to be service. In our study, 85% of respondents regarded advising students as a responsibility. Whereas Perrin and Lephart's3 study combined undergraduate and graduate programs' important criteria for tenure and promotion, respondents ranked advising fifth (Table 2). This is consistent with the finding of Staurowsky and Scriber6 that their respondents had student advising responsibilities.
Initially, individuals assuming the PD position may have perceived that they would have an increase in discretionary time due to a reduction in their clinical role in athletics. However, such an increase may not have been realized because of an unexpected increase in the demands and responsibilities of the position as PD. The PD today is working less with student-athletes in a clinical setting.2 In our study, 42% of respondents indicated they were clinically active, as compared with Perrin and Lephart,3 who reported 80% were clinically active in the athletic training room. In addition, we found that 77% of the PDs responding to the question on multiple role appointment had a shared appointment with athletics, but only 33% of that shared appointment involved working in the athletic training room (Table 1). These data can be misleading, as the PD position may be funded by athletics with only academic responsibilities.
The love for athletics and concern for the health and welfare of the student-athlete are typical forces driving one into the athletic training profession.3 However, changing roles may have created personal quandaries for the PD. Accepting the role of PD may have been perceived as an opportunity to decrease time spent traveling with athletic teams and, subsequently, an increase in personal and family time. We found that only 17% of the respondents had traveling responsibilities with athletics. This may also force the PD to make difficult choices among T&P requirements, involvement in clinical work, and personal and family time.
It has become increasingly difficult for PDs to keep up with clinical responsibilities in athletics as an athletic trainer. By limiting the clinical responsibilities and contact with student-athletes, the PD is not integrally involved in the daily operation of the athletic training room.11 This may affect the SAT's opinion of the PD's abilities as an athletic trainer. Also, this may be a conflict for the PD who wishes to continue performing clinical work. Restricting or eliminating this contact with the student-athlete may be a source of career dissatisfaction.3 Program directors may not feel they have the time to do everything that is required of them and are unsure how everything “fits in” with the overall priorities of the position. If left unsettled, this stressor could lead to job burnout and eventually more severe consequences, such as removing themselves from the athletic training profession completely.
RECOMMENDATIONS
Program directors must educate T&P faculty members, administrators, chairpersons, and deans on the responsibilities of their position. There may be some consideration given during a T&P decision if committee members are aware that the responsibilities of the PDs are much different than the traditional faculty member. Also, the aspect of clinical instruction needs to be addressed. In which area should clinical instruction be evaluated, and how?
The PD must understand the T&P process and be aware of how each of the 3 areas (teaching, research, and service) of the process are viewed and weighed at each respective institution. Do not assume that one area is weighted more than another. Find out from the most reliable source: the chairperson of the department or dean of the college. More time and effort should be spent on the areas of deficiency or areas viewed as more important by administrators. For example, if research is perceived by the university to be more important than service, then PDs need to make time in their schedule to concentrate on doing research, presenting research at scholarly meetings or conferences, and publishing research in refereed journals. As Perrin and Lephart3 indicated, areas such as teaching and student advising may suffer because of the “publish or perish” requirement.
When dealing with students' perceptions, the PD may need to spend more time with SATs when they are treating student-athletes or stop by and visit their practice sites. This is an important element of clinical experience and should be incorporated into the evaluation process. Injuries can be discussed and questions from the SAT can be answered. This makes the PD one of the “practicing athletic trainers” who has discussed their student-athletes' injuries. Also, attend workshops and demonstrate new techniques to SATs. This shows that the athletic training skills of PDs are no different than the skills of athletic trainers employed in athletics or other settings.
There is a question as to where clinical instruction belongs in the T&P process. Does it belong under teaching, research, or service? If clinical instruction is going to be evaluated in the area of teaching, then goals and objectives should be designed for clinical instruction. In addition, instructor and peer evaluations should be administered to assess the effectiveness of this form of teaching. Clinical instruction that is considered service should be logged or documented (including the number of hours spent on clinical instruction and a site evaluation) to show its importance. For clinical instruction to be considered research, there must be a well-thought-out plan, which may include validation of clinical techniques, presentation of quantitative or qualitative findings at regional and national conferences, and publication in appropriate peer-reviewed journals.
An athletic trainer should be designated as the clinical coordinator. The responsibilities of the clinical coordinator are to ensure that information taught in the classroom is practiced in the clinical setting. This is very helpful for the PD who has no clinical instructor or athletic responsibilities. It also lessens students' confusion when they are taught one technique in the classroom, only to be told to perform a different technique in the clinical setting.
CONCLUSIONS
The position of PD in an athletic training education program is continuing to evolve. Many of the expectations of the PD regarding tenure are the same today as they were more than a decade ago. It also appears that the profile of the PD is changing athletically, with fewer clinical activities involving student-athletes, and educationally with more terminal degrees.
Even though expectations have remained the same, roles and responsibilities have been increasing, thus creating a greater workload for the PD. Finally, the dilemmas described by Perrin and Lephart3 still exist today and may have become more complex because of educational reform and promotion and tenure requirements. Our study confirms that ongoing evaluation of the PD position is necessary.
REFERENCES
- 1.Sciera JL. The role of the NATA program director. Athl Train J Natl Athl Train Assoc. 1981;16:125–126. [Google Scholar]
- 2.Leard JS, Booth C, Johnson JC. A study of career pathways of NATA curriculum program directors. J Athl Train. 1991;26:211–214. [Google Scholar]
- 3.Perrin DH, Lephart SM. Role of the NATA curriculum director as clinician and educator. Athl Train J Natl Athl Train Assoc. 1988;23:41–43. 63. [Google Scholar]
- 4.Guidelines for Development and Implementation of NATA Approved Undergraduate Athletic Training Programs. Dallas, TX: National Athletic Trainers' Association; 1984. [Google Scholar]
- 5.Commission on Accreditation of Allied Health Education Programs. Standards and Guidelines on Education Programs for the Athletic Trainer. Chicago, IL: Commission on Accreditation of Allied Health Education Programs; 1991. [Google Scholar]
- 6.Staurowsky E, Scriber K. An analysis of selected factors that affect the work lives of athletic trainers employed in accredited educational programs. J Athl Train. 1998;33:244–248. [PMC free article] [PubMed] [Google Scholar]
- 7.Capel SA. Attrition of athletic trainers. J Athl Train. 1990;25:34–39. [Google Scholar]
- 8.National Athletic Trainers' Association. Accredited Programs. Available at: http://www.nata.org/Departments/membership/accredited.html. Accessed January 3, 2000.
- 9.National Athletic Trainers' Association. Position Vacancy Notice. Available at: http://www.nata.org/Departments/membership/pvn/2732.html. Accessed November 1, 1999–June 15, 2000.
- 10.Siedentop D, Tannehill D. Developing Teaching Skills in Physical Education. Mountain View, CA: Mayfield Publishing Co; 2000. p. 324. [Google Scholar]
- 11.Mangus B. The evolving roles of athletic training educators and clinicians. J Athl Train. 1998;33:308–309. [PMC free article] [PubMed] [Google Scholar]