

Abstract
Objective:
To assess scapular-positioning patterns using a static measurement technique.
Design and Setting:
We used a 4–within-factor design to compare scapular upward rotation among subjects. The within factors included side (dominant, nondominant), plane of motion (scapular, sagittal), direction of motion (ascending, descending), and level of humeral rotation (rest, 30°, 60°, 90°, 120°).
Subjects:
Twenty-seven subjects with unimpaired shoulders.
Measurements:
We measured scapular position and glenohumeral range of motion using a digital inclinometer and goniometer, respectively. All measurements were performed bilaterally.
Results:
Between-session repeatability was poor to excellent depending on humeral-elevation angle. The scapular plane demonstrated significantly more scapular upward rotation than did the sagittal plane at 120° of humeral elevation.
Conclusions:
The scapula demonstrated a consistent pattern of downward rotation initially from rest to 30° of humeral elevation, followed by an upward rotation after 30° of humeral elevation to the highest level (120°). Scapular upward rotation is greater in the scapular plane than in the sagittal plane. Therefore, overhead rehabilitation exercises should be performed in the scapular plane, especially in subjects with rotator cuff tendinopathy.
Keywords: scapular upward rotation, glenohumeral, inclinometer, scapular plane
During dynamic arm movement, the scapula must move synchronously with the humerus to provide optimal congruence between the glenoid and the humeral head. This congruence is necessary for establishing adequate length-tension relationships for the muscles acting on the scapula and the humeral head1–3 and for maintaining a stable base for transferring kinetic energy from proximal to distal segments.4–6 In addition, abnormal scapular movement (or positioning), especially at the extremes of humeral elevation, has been identified as a causative agent in the development of shoulder conditions such as subacromial impingement and glenohumeral instability.4,7–10
During humeral movement, the scapula has been shown to rotate about 3 axes, anterior-posterior or horizontal (perpendicular to the scapular plane), superior-inferior or vertical, and medial-lateral (parallel to the scapular spine), thus producing 3 distinct motions, anterior-posterior tilting, upward-downward rotation, and internal-external rotation, respectively.11–13 Researchers have developed quantitative techniques for assessing 3-dimensional scapular kinematics that require significant technical detail by using costly equipment.3,9,11,12 High cost and technologic sophistication have precluded the use of these techniques in the clinical setting. Because of the need for a quantifiable method of assessing scapular kinematics, clinical scientists have been experimenting with instrumented techniques that are cost and time efficient and clinically useful.3,4
Upward rotation of the scapula is suggested to be clinically important because the scapula must rotate adequately in an upward fashion to prevent the humeral head from compressing and shearing against the undersurface of the acromion process during humeral elevation.3,4,7,10,14 The combination of shear (mechanical abrasion) and compression forces of the humeral head on the undersurface of the acromion and coracohumeral arch has been described as the main mechanism responsible for producing subacromial impingement.4,7,10,14 Clinically, patients with rotator cuff impingement pain have less scapular upward rotation than do patients without rotator cuff impingement.10 The ability to detect diminished upward rotation of the scapula may aid in preventing and evaluating shoulder impairments. For example, it may help diagnose impairment, such as impingement, or can be used to screen athletes who may be predisposed to shoulder impairment, such as throwers and swimmers.3,14–16
Because the humerus is free to move in multiple planes and directions of motion, it may be important to assess scapular motion during humeral motion in multiple planes, angles or arcs, and directions of motion. To date, most of the published reports investigating scapular kinematics in vivo and ex vivo have described scapular motion (position) as a function of humeral elevation in one plane or one direction of movement (or both).1–14,17–19 Warner et al7 and McClure et al20 studied scapular positioning during upward and downward rotation of the humerus, whereas Koh et al11 and Pascoal et al21 studied scapular upward rotation in multiple planes and angles of humeral elevation. No conclusions were drawn as to which angle (arc), direction, or plane of humeral motion was optimal for identifying normal and abnormal scapular kinematic patterns. To establish optimal testing procedures for future studies using this instrumented technique, it is important to determine whether there are differences among the measurements obtained at different angles and in different planes and directions of humeral motion.
Therefore, our primary aim was to assess and compare scapular upward rotation bilaterally, in 2 planes (scapular and sagittal), in 2 directions (ascending and descending), and at multiple angles of humeral elevation.
Secondary objectives were to compare measures of isolated glenohumeral range of motion with scapular upward rotation. Measures of isolated glenohumeral range of motion are presumed to represent capsular mobility. Theoretically, decreased capsular mobility may result in a “pulling” of the scapula during humeral elevation, with a subsequent increase in scapular upward rotation. Conversely, greater glenohumeral range of motion could increase the relative contribution of humeral motion to the scapulohumeral rhythm, resulting in decreased scapular upward rotation. Clinically, it is important to understand the relationship among these variables in unimpaired shoulders to establish normative data. Therefore, preliminary investigation of these relationships is warranted.
METHODS
Subjects and Design
A sample of convenience comprising 27 subjects (10 men, 17 women; mean age = 20.4 ± 2.4 years, height = 171.7 ± 12.0 cm, mass = 70.4 ± 14.7 kg) who volunteered to participate was used in this study. Subjects were included if both shoulders were unimpaired and they could elevate their arms more than 120°. Subjects were excluded if they had a history of injury to either shoulder or if they had participated in an overhead sport or occupation for 10 years or more. Informed consent was obtained before testing. The institution's human subjects review board for health sciences reviewed and approved the study protocol.
A 4–within-factor design was used to compare scapular upward rotation among subjects. The within factors included side (dominant and nondominant), plane of motion (scapular and sagittal), direction of motion (ascending and descending), and level of humeral elevation (rest, 30°, 60°, 90°, or 120°).
Instrumentation
Scapular position was measured using a Saunders Digital Inclinometer (The Saunders Group Inc, Chaska, MN) modified to rest evenly on the scapular spine (Figure 1).3 The digital inclinometer can measure angles up to 360° and is accurate to 0.1°, as reported by the manufacturer. A 2.13-m (7-ft) pole was used to guide the arm during humeral elevation. Markers were placed on the pole at the selected angles where scapular-position measures were taken. A standard plastic goniometer was used to measure isolated glenohumeral internal and external rotation and abduction.
Figure 1.

Modified digital inclinometer. A, Locator rods. B, Digital display of angle. C, Hold button. D, Bubble level.
Data Collection
Scapular Position
We measured scapular position using the protocol developed by Johnson et al,3 which demonstrated good to excellent intraexaminer reliability and good to excellent criterion-related validity when measuring scapular upward rotation in the scapular plane. The subject stood with feet shoulder-width apart and arms at the sides. Subjects were instructed to place their heels on a line on the floor and extend their arms with the hand open. Also, subjects had to point their thumbs toward the ceiling throughout the testing motion to control for humeral rotation. The guiding pole was placed at an angle of 40° anterior from the frontal plane, ensuring humeral elevation in the scapular plane, and 90° anterior from the frontal plane, ensuring elevation in the sagittal plane. The selected humeral-elevation angles were determined using the digital inclinometer. The digital inclinometer was placed along the lateral border of the upper arm at midshaft, and the subject's arm was moved to each angle where the position was marked on the guiding pole.
When instructed, the subject raised (or lowered) the arm slowly to the specified mark on the guiding pole, and the scapular position was measured. Scapular position was measured at 5 angles of humeral elevation (rest, 30°, 60°, 90°, 120°). Scapular position was measured by locating the root of the scapular spine and the posterolateral acromion by palpation. The medial locator arm of the digital inclinometer was placed over the root, whereas the lateral locator arm was placed over the posterolateral acromion (Figure 2). The digital inclinometer was then held at a right angle to the horizontal plane using a bubble level, and the examiner pressed the hold button to secure the measure. To avoid examiner bias, a slip of paper was placed over the screen on which a digital readout of the measure was given. After the hold button was pressed, the examiner removed the slip and recorded the measure.
Figure 2.

Clinical technique for measuring scapular upward rotation with the modified digital inclinometer. Locator rods were aligned with the scapular spine.9
Ascending measurements were obtained by having the subject elevate the arm from the resting position directly to the test position. Descending measurements were taken by having the subject raise the arm to the maximum elevation, hold it for 2 seconds, and then lower it to the selected angle. A 5-second rest (recovery) period was provided between test trials. The order in which test positions (side, humeral-elevation angle, plane of motion, and direction of motion) were measured was determined randomly. The same investigator performed all test measurements. One measurement (trial) was taken at each test position. The rationale for using only 1 measurement at each position was based on a small-scale pilot study that we performed using 10 subjects. The test procedures were identical except that 3 measurements were performed at each level of humeral elevation. Intraclass correlation (ICC) analysis for scapular upward rotation revealed minimal differences (<0.5°) and high repeatability (ICC = .97 to .99) among the 3 trials. In addition, Johnson et al3 showed excellent reliability between 2 trials of testing at each position of humeral elevation (ICC = .89 to .96).
No subject complained of fatigue during the test trials; therefore, we do not believe that fatigue was a limiting factor in the study. Also, counterbalancing our test measurements helped to control for fatigue.
To determine test-retest repeatability, 10 subjects (5 men and 5 women: 20 shoulders) were instructed to return 1 week later for a second test session.
Isolated Glenohumeral Range-of-Motion Measures
After scapular kinematic testing, isolated glenohumeral internal-external rotation and elevation range-of-motion measures were performed on each subject using standard examination techniques.22 With the subject lying supine, the humerus was placed in a position of 90° abduction and neutral rotation, and the elbow was flexed to 90°. The examiner passively moved the arm into internal or external rotation until a clinical endpoint was reached. At that point, the angle was measured with the goniometer.
Isolated glenohumeral elevation also was measured using the methods described by Lintner et al.23 It was defined as the angle of humeral elevation at which the inferior angle of the scapula began to rotate in the upward direction as detected by examiner palpation.23 The subject was seated, and the inferior angle of the scapula was located by palpation. The subject was instructed to actively elevate the arm in the scapular plane. Once scapular upward rotation occurred, the subject was instructed to hold that position, and the examiner measured the humeral-elevation angle with the goniometer.
The measures of isolated glenohumeral range of motion are considered to be achieved purely at the glenohumeral joint when the scapula is stabilized.22,23 Test order for side (dominant, nondominant) and direction (internal-external rotation, elevation) was performed in a random manner.
Statistical Procedures and Analysis
Repeatability
We calculated between-session repeatability using the ICC (2,1) formula reported previously.24,25 Using an analysis of variance (ANOVA) for repeated measures, the mean square values were obtained for inclusion in the ICC (2,1) formula. All repeatability coefficients were interpreted as follows: below .69 was poor, .70 to .79 was fair, .80 to .89 was good, and .90 to 1.00 was considered excellent.26
Within-Subjects Comparisons
We used a 4-factor within-subjects ANOVA to determine significant mean differences among the levels of the independent variable, scapular position. In the presence of a significant interaction effect, planned and unplanned pairwise comparisons with Bonferroni adjustments for multiple comparisons were used to determine main effects and simple main effects, respectively.
Correlations
Pearson bivariate correlations were calculated to assess the statistical relationship between total range for scapular upward rotation and glenohumeral internal-external and elevation range of motion. For the purposes of this study, correlation coefficients were interpreted as follows: below .50 was poor, .50 to .75 was good, and above .75 was excellent.26
All statistical calculations were performed using the SPSS statistics package (version 10.0, SPSS Inc, Chicago, IL).
RESULTS
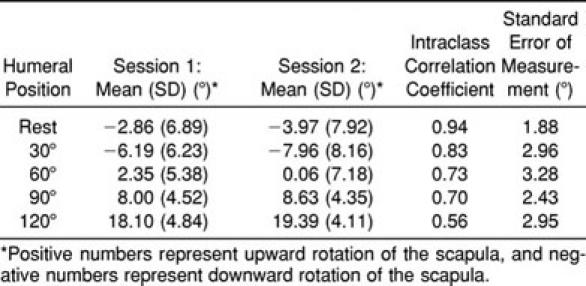
Intraclass correlation (2,1) values, means, standard deviations, and standard errors of measurements were calculated for scapular upward rotation at each of the specified humeral angles for both sessions (Table 1).
Table 1.
Between-Session Repeatablity at Each Angle of Humeral Elevation
Mean scapular-position values for each humeral-elevation angle are presented in Figure 3. Analysis of variance revealed a significant interaction effect for plane × angle (F4,104 = 7.86, P < .001) (Figure 4). The interaction effects for side × plane × direction × angle (F4,104 = 1.39, P = .24), side × plane × angle (F4,104 = 1.32, P = .27), side × plane × direction (F1,26 = 0.065, P = .80), side × direction × angle (F4,104 = 2.04, P = .09), plane × direction × angle (F4,104 = 0.422, P = .79), side × plane (F1,26 = 6.4, P = .50), side × direction (F1,26 = 0.27, P = .61), side × angle (F4,104 = 0.54, P = .71), plane × direction (F1,26 = 1.35, P = .25), and direction × angle (F4,104 = 0.722, P = .58) were not statistically significant.
Figure 3.

Global scapular-positioning pattern plotted as a function of humeral-elevation angle. Error bars represent standard deviations. Scapular position was significantly different between humeral-elevation angles (P < .05).
Figure 4.

Mean (±SD) scapular upward rotation plotted as a function of humeral-elevation angle to show significant differences between the sagittal and scapular planes. *Scapular plane demonstrated significantly more scapular upward rotation than did the sagittal plane from 90° to 120° of humeral elevation (P < .001).
For the plane × angle interaction effect, unplanned pairwise multiple comparisons were used to test for simple main effects with an accepted alpha level of P ≤ .01 (.05/5 Bonferroni adjustment for multiple comparisons). The scapular plane demonstrated significantly more scapular upward rotation than did the sagittal plane at 120° of humeral elevation (t26 = 3.6, P = .001) (see Figure 4).
The main effect for angle (F1,26 = 163.2, P < .001) was significant. Planned pairwise comparisons revealed significant differences between angles of humeral elevation (P < .05) (see Figure 3). Main effects for side (F1,26 = 0.126, P = .73), plane (F1,26 = 0.018, P = .89), and direction (F1,26 = 0.245, P = .65) were not significant.
Pearson bivariate correlation coefficients revealed poor relationships between the total range for scapular upward rotation and isolated glenohumeral internal-external rotation (r = .35, P = .010), external rotation (r = .38, P = .004), and elevation (r = .31, P = .024).26
DISCUSSION
Repeatability
The clinical technique we used to assess scapular upward rotation demonstrated poor to excellent repeatability between test sessions26 and standard errors of measurement between 1.8° and 3.3°, depending on the arc of humeral elevation (see Table 1). In a similar study, Johnson et al3 reported good to excellent intraexaminer reliability during a single test session; however, intersession reliability was not investigated. Our measures revealed a trend toward lower test-retest repeatability as the humeral-elevation angle increased. We attribute this decreased repeatability at the higher angles of humeral elevation to increased difficulty and a lack of consistency in palpating and locating bony reference points. Lack of clinical experience or mastery of this technique may negatively affect the repeatability and precision of measurement. To improve repeatability, we recommend that the examiner have sufficient practice with the technique and conduct pilot studies before using it to ensure that the measures are repeatable and precise.
Global Scapular-Positioning Pattern
The scapula demonstrated a discernable pattern of rotation in relation to elevation of the humerus. In our sample of subjects with unimpaired shoulders, the scapula demonstrated a consistent pattern of downward rotation initially (average, 5°) from 0° to 30° of humeral elevation, followed by an upward rotation (average, 18°) after 30° of humeral elevation to the highest level (120°) (see Figure 3). This pattern of downward rotation has not been reported in previous studies; however, several investigators discuss a “setting” phase or period in which scapular rotation is highly variable among subjects. During this setting phase, the scapula has been reported to abduct, adduct, oscillate, or remain fixed.2,7 This setting phase is suggested to occur from rest to 60° of humeral elevation, after which a consistent relationship (of approximately 2:1) between humeral elevation and scapular upward rotation exists throughout the remainder of the range of motion.1,18,27 It seems reasonable that downward rotation of the scapula may occur during this setting phase because of the weight of the limb and the resultant muscular forces acting on the scapula and the humerus during movement of the arm from a resting position. The forces created by the scapular (upper trapezius and serratus anterior) and humeral (deltoid and supraspinatus) rotators may pull the scapula downward initially in an attempt to create adequate length-tension relationships for these muscles acting on the humerus.
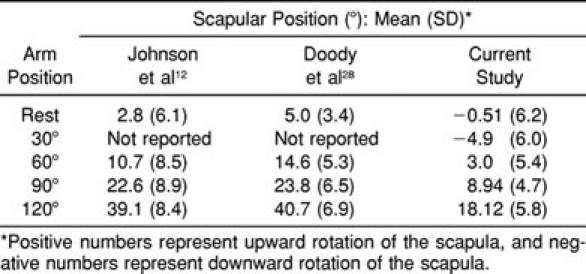
Our mean values for scapular upward rotation are considerably less than those reported by Johnson et al3 in a similar study using the same instrumentation, technique, and testing protocol for a mixed group of subjects with unimpaired and impaired shoulders as well as the values reported in other studies using different instrumentation (Table 2).9,10,12,14,28 Lukasiewicz et al14 reported a mean scapular upward rotation of 28.2° (±8.4°) from rest to 120° of arm elevation in a mixed group of subjects with unimpaired and impaired shoulders. Johnson et al12 reported mean scapular upward-rotation values ranging from 30° to 35° in healthy shoulders. Most other studies show mean scapular upward-rotation values ranging from 28° to 40° at rest to 140° of arm elevation.9,10,18,28 Instrumentation and experimental procedures varied among studies, as did age and injury status. Some authors used subjects from a wide spectrum of age groups, whereas others used only subjects of college-going age. Similarly, some researchers measured only abnormal shoulders, whereas others pooled data from both impaired and unimpaired shoulders. These differences may have accounted for some of the variances between our results and those of others.
Table 2.
Mean Values for Scapular Upward Rotation
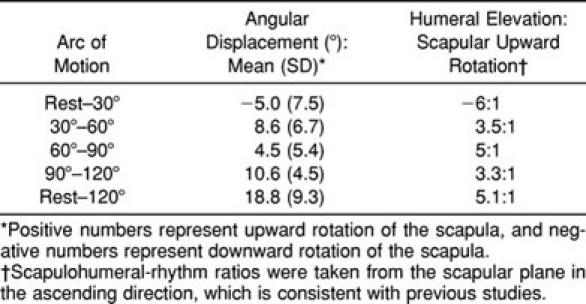
Another aim of the study was to look at the relative contributions of the scapula and the humerus to overall arm elevation. This relationship between humeral and scapular motion, often referred to as scapulohumeral rhythm, depends on the angle of humeral elevation.18 Because this relationship has been shown to be nonlinear, it may be more appropriate to observe and interpret scapulohumeral rhythm in increments or isolated arcs of motion.8,18 Scapulohumeral-rhythm ratios have been shown to be very high in the early stages of elevation (eg, setting phase), followed by decreasing ratios as the humeral angle increases over the arc of motion. A higher ratio indicates less relative contribution of the scapula to the overall motion of the elevating shoulder. Most investigators reporting scapulohumeral rhythm took measures in the scapular plane and ascending direction of humeral elevation. Our scapulohumeral ratios for the scapular plane during the ascending direction ranged from 2.8° to 6.7° of humeral elevation to 1° of scapular upward rotation with an overall ratio of 5.1:1 (Table 3). Our findings deviate from early findings of ratios ranging from 3:1 to 1:127,29,30 but are more consistent with recent findings of 7.9:1 to 2.9:1 by McQuade and Smidt.31 Our ratios were lowest in the midrange of elevation, indicating a larger contribution of the scapula to elevation. This finding is consistent with those of Freedman and Munro30 and Doody et al,32 who stated that during the midrange of elevation, the moment arms of the scapular rotators are greater than those of the humeral rotators, thus creating a mechanical advantage for the scapula. Scapulohumeral-rhythm ratios also have been reported to decrease as resistance or load is added to the humerus during elevation.31
Table 3.
Angular Displacement of the Scapula as a Function of Humeral Elevation with Related Scapulohumeral Rhythm Ratios
Effect of Plane and Direction of Motion
Our results demonstrate greater upward rotation of the scapula in the scapular plane than in the sagittal plane during the final arc of humeral elevation (90° to 120°) (see Figure 4). We hypothesize that the smaller amount of scapular upward rotation in the sagittal plane is due to limited subacromial clearance for the humeral head during humeral elevation. This planar difference in humeral elevation during the terminal stage of scapular upward rotation is an important finding when considering the relationship between scapular upward rotation and subacromial impingement. During the evaluation of a patient with an injured shoulder, scapular upward-rotation testing in both the sagittal and the scapular planes may be useful for observing dyskinetic scapular motion. Furthermore, testing in the sagittal plane may be useful because it closely replicates the Neer sign and, therefore, may be a sensitive test for identifying impairment due to rotator cuff tendinopathy.
Our findings suggest that to lower the chances of subacromial impingement, it may be advantageous for patients with rotator cuff tendinopathy to perform overhead rehabilitation exercises in the scapular plane rather than in the sagittal plane.
Although the scapular plane demonstrated significantly more upward rotation than did the sagittal plane during the final arc of humeral elevation (90° to 120°), scapular-positioning patterns do not appear to vary significantly among planes and directions of humeral elevation (Figure 5). Therefore, for a better appreciation of dyskinetic scapular motion, we recommend testing in both the sagittal and the scapular planes when making side-to-side comparisons. We further recommend taking the measure using only 1 direction of motion. By using only 1 direction of motion, the examiner will significantly reduce the time required to perform the test and prevent patient discomfort from prolonged humeral elevation.
Figure 5.

Scapular-positioning pattern plotted as a function of humeral-elevation angle between the ascending and descending directions of motion.
Correlations
Gibson et al6 posited that premature scapular motion during humeral abduction may occur as a result of restricted or tight capsuloligamentous tissue. We hypothesized that subjects with less isolated glenohumeral internal and external rotation and elevation would show more scapular upward rotation. Less glenohumeral range of motion would indicate a tighter capsule. The increased scapular upward rotation would be the result of a tighter capsule “pulling” the scapula along during humeral elevation or rotation, whereas a more lax capsule would cause less scapular upward rotation, especially at the lower ranges of humeral elevation. Our correlations revealed statistically significant relationships between glenohumeral range of motion and scapular upward rotation; however, the relationships were considered to be poor (<0.50).26 It appears that other factors, such as muscular forces, contribute more significantly to scapular upward rotation than does capsular tension.
Future Directions
Based on our repeatability findings, we believe that it is necessary to conduct a more large-scale study of between-examiner and between-session repeatability to further elucidate the issue of difference in measurement among studies. Once repeatability is fully established, future researchers should examine the effectiveness of this clinical technique in predicting or detecting shoulder abnormalities and in determining the effectiveness of selected therapeutic interventions.
CONCLUSIONS
The scapula demonstrated a consistent pattern of downward rotation initially from rest to 30° of humeral elevation, followed by an upward rotation after 30° of humeral elevation to the highest level (120°). Scapular upward rotation is greater in the scapular plane than in the sagittal plane. Therefore, overhead rehabilitation exercises should be performed in the scapular plane, especially in subjects with rotator cuff tendinopathy.
REFERENCES
- 1.Culham E, Peat M. Functional anatomy of the shoulder complex. J Orthop Sports Phys Ther. 1993;18:342–350. doi: 10.2519/jospt.1993.18.1.342. [DOI] [PubMed] [Google Scholar]
- 2.Hart DL, Carmichael SW. Biomechanics of the shoulder. J Orthop Sports Phys Ther. 1985;6:229–234. [PubMed] [Google Scholar]
- 3.Johnson MP, McClure PW, Karduna AR. New method to assess scapular upward rotation in subjects with shoulder pathology. J Orthop Sports Phys Ther. 2001;31:81–89. doi: 10.2519/jospt.2001.31.2.81. [DOI] [PubMed] [Google Scholar]
- 4.Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998;26:325–337. doi: 10.1177/03635465980260022801. [DOI] [PubMed] [Google Scholar]
- 5.Paine RM, Voight M. The role of the scapula. J Orthop Sports Phys Ther. 1993;18:386–391. doi: 10.2519/jospt.1993.18.1.386. [DOI] [PubMed] [Google Scholar]
- 6.Gibson MH, Goebel GV, Jordan TM, Kegerreis S, Worrell TW. A reliability study of measurement techniques to determine static scapular position. J Orthop Sports Phys Ther. 1995;21:100–106. doi: 10.2519/jospt.1995.21.2.100. [DOI] [PubMed] [Google Scholar]
- 7.Warner JJ, Micheli LJ, Arslanian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome: a study using Moire topographic analysis. Clin Orthop. 1992;285:191–199. [PubMed] [Google Scholar]
- 8.McQuade KJ, Dawson J, Smidt GL. Scapulothoracic muscle fatigue associated with alterations in scapulohumeral rhythm kinematics during maximum resistive shoulder elevation. J Orthop Sports Phys Ther. 1998;28:74–80. doi: 10.2519/jospt.1998.28.2.74. [DOI] [PubMed] [Google Scholar]
- 9.Ludewig PM, Cook TM, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24:57–65. doi: 10.2519/jospt.1996.24.2.57. [DOI] [PubMed] [Google Scholar]
- 10.Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. 2000;80:276–291. [PubMed] [Google Scholar]
- 11.Koh TJ, Grabiner MD, Brems JJ. Three-dimensional in vivo kinematics of the shoulder during humeral elevation. J Appl Biomech. 1998;14:312–326. doi: 10.1123/jab.14.3.312. [DOI] [PubMed] [Google Scholar]
- 12.Johnson GR, Stuart PR, Mitchell S. A method for the measurement of three-dimensional scapular movement. Clin Biomech. 1993;8:269–273. doi: 10.1016/0268-0033(93)90037-I. [DOI] [PubMed] [Google Scholar]
- 13.Karduna AR, McClure PW, Michener LA. Scapular kinematics: effects of altering the Euler angle sequence of rotations. J Biomech. 2000;33:1063–1068. doi: 10.1016/s0021-9290(00)00078-6. [DOI] [PubMed] [Google Scholar]
- 14.Lukasiewicz AC, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;21:574–586. doi: 10.2519/jospt.1999.29.10.574. [DOI] [PubMed] [Google Scholar]
- 15.Odom CJ, Taylor AB, Hurd CE, Denegar CR. Measurement of scapular asymmetry and assessment of shoulder dysfunction using the lateral scapular slide test: a reliability and validity study. Phys Ther. 2001;81:799–809. doi: 10.1093/ptj/81.2.799. [DOI] [PubMed] [Google Scholar]
- 16.Crotty NM, Smith J. Alterations in scapular position with fatigue: a study in swimmers. Clin J Sport Med. 2000;10:251–258. doi: 10.1097/00042752-200010000-00005. [DOI] [PubMed] [Google Scholar]
- 17.de Groot JH, van Woensel W, van der Helm FC. Effect of different arm loads on the position of the scapula in abduction postures. Clin Biomech (Bristol, Avon) 1999;14:309–314. doi: 10.1016/s0268-0033(98)90094-8. [DOI] [PubMed] [Google Scholar]
- 18.Bagg SD, Forrest WJ. A biomechanical analysis of scapular rotation during arm abduction in the scapular plane. Am J Phys Med Rehabil. 1988;67:238–245. [PubMed] [Google Scholar]
- 19.Youdas JW, Carey JR, Garrett TR, Suman VJ. Reliability of goniometric measurements of active arm elevation in the scapular plane obtained in a clinical setting. Arch Phys Med Rehabil. 1994;75:1137–1144. doi: 10.1016/0003-9993(94)90091-4. [DOI] [PubMed] [Google Scholar]
- 20.McClure PW, Michener LA, Sennett BJ, Karduna AR. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg. 2001;10:269–277. doi: 10.1067/mse.2001.112954. [DOI] [PubMed] [Google Scholar]
- 21.Pascoal AG, van der Helm FF, Pezarat Correia P, Carita I. Effects of different arm external loads on the scapulo-humeral rhythm. Clin Biomech (Bristol, Avon) 2000;15(suppl 1):S21–S24. doi: 10.1016/s0268-0033(00)00055-3. [DOI] [PubMed] [Google Scholar]
- 22.Norkin CC, White DJ. Measurement of Joint Motion: A Guide to Goniometry. Philadelphia, PA: FA Davis; 1985. [Google Scholar]
- 23.Lintner SA, Levy A, Kenter K, Speer K. Glenohumeral translation in the asymptomatic athlete's shoulder and its relationship to other clinically measurable anthropometric variables. Am J Sports Med. 1996;24:716–720. doi: 10.1177/036354659602400603. [DOI] [PubMed] [Google Scholar]
- 24.Denegar CR, Ball DW. Assessing reliability and precision of measurement: an introduction to intraclass correlation and standard error of measurement. J Sport Rehabil. 1993;2:35–42. [Google Scholar]
- 25.Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–428. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- 26.Portney L, Watkins M. Foundations of Clinical Research: Applications to Practice. Norwalk, CT: Appleton & Lange; 1993. [Google Scholar]
- 27.Inman VT, Saunders JB, Abbott LC. Observations of the function of the shoulder joint. J Bone Joint Surg Am. 1944;32:1–30. [Google Scholar]
- 28.Doody SG, Waterland JC, Freedman L. Scapulo-humeral goniometer. Arch Phys Med Rehabil. 1970;51:711–713. [PubMed] [Google Scholar]
- 29.Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976;58:195–201. [PubMed] [Google Scholar]
- 30.Freedman L, Munro RR. Abduction of the arm in the scapular plane: scapular and glenohumeral movements: a roentgenographic study. J Bone Joint Surg Am. 1966;48:1503–1510. [PubMed] [Google Scholar]
- 31.McQuade KJ, Smidt GL. Dynamic scapulohumeral rhythm: the effects of external resistance during elevation of the arm in the scapular plane. J Orthop Sports Phys Ther. 1998;27:125–133. doi: 10.2519/jospt.1998.27.2.125. [DOI] [PubMed] [Google Scholar]
- 32.Doody SG, Freedman L, Waterland JC. Shoulder movements during abduction in the scapular plane. Arch Phys Med Rehabil. 1970;51:595–604. [PubMed] [Google Scholar]