

Abstract
Objective:
To compare the effects of low doses of creatine and creatine loading on strength, urinary creatinine concentration, and percentage of body fat.
Design and Setting:
Division IA collegiate football players took creatine monohydrate for 10 weeks during a sport-specific, periodized, off-season strength and conditioning program. One-repetition maximum (1-RM) squat, urinary creatinine concentrations, and percentage of body fat were analyzed.
Subjects:
Twenty-five highly trained, Division IA collegiate football players with at least 1 year of college playing experience.
Measurements:
We tested strength with a 1-RM squat exercise before, during, and after creatine supplementation. Percentage of body fat was measured by hydrostatic weighing before and after supplementation. Urinary creatinine concentration was measured via light spectrophotometer at 0, 1, 3, 7, 14, 21, 28, 35, 42, 48, 56, and 63 days. An analysis of variance with repeated measures was computed to compare means for all variables.
Results:
Creatine supplementation had no significant group, time, or interaction effects on strength, urinary creatinine concentration, or percentage of body fat. However, significant time effects were found for 1-RM squat and fat-free mass in all groups.
Conclusions:
Our data suggest that creatine monohydrate in any amount does not have any beneficial ergogenic effects in highly trained collegiate football players. However, a proper resistance training stimulus for 10 weeks can increase strength and fat-free mass in highly trained athletes.
Keywords: creatine phosphate, ergogenic aids, resistance training
Athletes continue to search for the most effective supplement to aid performance. Athletes use a wide variety of commercial supplements because of the belief that the supplements possess beneficial effects. Some examples include l-carnitine, ginseng, chromium, glutamine, amino acids, protein powders, and creatine monohydrate, taken alone or in combination. Some supplements may cause long-term or short-term harmful effects, a possibility that has stimulated concern among health care professionals, exercise physiologists, and coaches. Because we do not know conclusively which supplements are ergogenic or ergolytic, we need to further examine specific supplements and their effects on exercise.
Recently, creatine monohydrate has become the nutritional supplement of choice for athletes. This compound has accounted for most of the supplement sales during the past few years, and the market continues to grow as a result of endorsement by professional athletes. In addition, creatine does not appear on the banned list of substances of any sports federation.
Professional athletes have a tremendous influence on many other athletes at various levels of competition. Currently, college, high school, and recreational athletes are questioning the effects of creatine. Recent studies have supported creatine as an effective, harmless ergogenic aid with no short-term contraindications.1–11 However, the effect of long-term use of creatine monohydrate on athletes is unclear; hence, the medical community has raised concerns, and possible health risks have been suggested.12
Creatine supplementation has resulted in positive physiologic effects on skeletal muscle creatine phosphate stores; short-duration, high-intensity anaerobic exercise; strength; and body composition in physically active subjects.1–21 These subjects have used a loading protocol of 20 to 30 g·d−1 for up to 7 days, but most of these studies were not conducted in sport-specific settings.1,2,13–18
If creatine supplementation, specifically loading, causes a surplus of creatine in the muscle, then any excess can be converted and excreted in the form of creatinine.13,19,20 Creatinine is produced from creatine as a byproduct of catabolism in skeletal muscle, and it appears in the urine. Therefore, creatine loading may not be beneficial to athletes if the muscle can only hold a predetermined concentration. Harris et al22 showed that approximately 155 mmol·kg−1 of dry muscle mass may represent the upper storage limit of creatine when a subject ingests 5 g 4 to 6 times per day. Thus, creatine loading may result in an excessive creatine concentration, which can be converted to creatinine and excreted. This finding suggests that creatine loading may not be necessary for those athletes (eg, football players) engaged in long-term supplementation.
Therefore, the purpose of our investigation was to compare the effects of low-dose creatine supplementation (3 g·d−1) to a loading protocol of 20 g·d−1 for 7 days and 5 g·d−1 thereafter for 10 weeks on 1-repetition maximum (1-RM) squat strength, creatinine excretion, and percentage of body fat in highly trained collegiate football players.
METHODS
Procedures
The subjects in this study were 25 male (age, 19 ± 1.02 years; height, 185.8 ± 5.27 cm; mass, 100.89 ± 21.79 kg), highly trained, NCAA Division IA collegiate football players with at least 1 year of college experience. All subjects were engaged in an off-season resistance training and conditioning program designed by the members of our strength and conditioning staff from the Department of Intercollegiate Athletics. Written consent was obtained from all subjects before testing and training, and the Institutional Review Board for the Protection of Human Subjects approved this project.
We selected subjects using the following criteria: (1) members of the institution's football team for at least 1 season; (2) weight training and conditioning limited to 4 specified sessions per week during the off-season program; (3) injury free; (4) not taking other substances that might aid athletic performance for 4 weeks before the study began and no other supplements for 10 weeks; and (5) maintenance of a normal diet while participating in the study.
We randomly placed 25 subjects into 1 of 3 groups: (1) creatine supplementation of 3 g·d−1; (2) creatine supplementation of 20 g·d−1 for 7 days, followed by creatine supplementation of 5 g·d−1 for the remainder of the study; or (3) a placebo group. The subjects were permitted to withdraw from the study at any time.
All subjects were familiarized with the scope of the study 1 week before its start. Since all subjects were team members for at least 1 year, they were extremely familiar with the training program, especially the squat exercise. Each subject took part in the preliminary testing 3 days before supplementation. The 1-RM squat, baseline urinary creatinine concentrations, and percentage of body fat (via hydrostatic weighing) were measured.
Creatine supplementation took place in a single-blind fashion, with each subject receiving a high or low dose of creatine or the placebo. Each creatine tablet (Createam Chewables, NutraSense Co, Shawnee Mission, KS) contained 1 g of creatine and 1.4 g of dextrose. The placebo tablet (Nutrasense) contained 2.4 g of dextrose. For the first week (loading phase), ingestion occurred 4 times per day. High-dose creatine (5 creatine tablets), low-dose creatine (3 creatine tablets and 2 placebo tablets), or placebo (5 placebo tablets) was taken when the subjects awoke, before and after the workout session, and in the evening before bed. For the subsequent 9 weeks, the high or low dose of creatine or the placebo dose was ingested once per day after workouts and at the same time on off days.
During the 10-week supplementation period, all subjects participated only in the University's off-season conditioning program, which consisted of periodized resistance and agility training. More specifically, the program consisted of 4 h·week−1 of heavy resistance training and 4 h·week−1 of conditioning. Weight training and conditioning were performed on Monday, Tuesday, Thursday, and Friday. All subjects completed the same number of morning workouts, sets, repetitions, and exercises at specified percentages of a 1-RM, regardless of position. The strength and conditioning coach led all workout sessions to ensure highly productive strength training and took a team approach in which each exercise is performed on the strength coach's cue. For example, all athletes started a lift on command. After each set was a specified rest interval, and then the next set would begin.
A 10-week, periodized resistance training program was designed. The primary exercises in the strength program were the front squat, back squat, hang clean, power clean, overhead press, bench press, single-arm dumbbell press, 1-arm rows, straight-leg dead lift, power shrugs, upright rows, chin-ups, dips, medicine ball plyometrics, and bumper-plate push-ups. The periodization protocol was a 5-week base hypertrophy phase (4 to 6 sets at 50% to 80% 1-RM), followed by a 2-week power phase (3 to 5 sets at 80% to 88%). After this 7-week period, a 2-week strength phase (1 to 3 sets at 90% to 95%) was implemented, followed by a 1-week peak strength phase (1 to 3 sets at 95% to 100%). The strength and conditioning staff, athletic trainers, and football coaches supervised all strength and conditioning sessions.
The 1-RM back-squat values were obtained before (week 0), during (week 5), and after supplementation (week 10). Urine samples were collected in sterile containers during the supplementation period on days 0, 1, 3, 7, 14, 21, 28, 35, 42, 49, 56, and 63, 4 hours after creatine tablet ingestion. During this 4-hour period, each subject was allocated 300 mL of water in a water bottle, the only liquid the athlete was allowed to consume until the urine sample was obtained. Each sample was analyzed using a spectrophotometric method.
Creatinine Measurement
A creatinine assay kit (Sigma Diagnostics, St. Louis, MO) was used to prepare the urine for analysis. The urine was diluted with distilled water in a standard test tube (0.5 mL of urine was added to 7 mL of distilled water). An alkaline picrate solution was prepared by mixing 5 parts of the creatinine color reagent (0.6% picric acid, sodium borate, and surfactant) to 1 part sodium hydroxide. Next, a pipette was used to place 300 μL of the diluted urine in a cuvette, where it was mixed with 3 mL of the alkaline picrate solution. This mixture was allowed to incubate for 10 minutes before the initial absorbance was read at 500 μm by the spectrophotometer. Finally, 100 μL of an acid reagent (mixture of sulfuric and acetic acid) was added to the assay and allowed to incubate for 5 minutes. Then the final absorbance was read at 500 μm by the spectrophotometer.
Back Squat
The back-squat exercise was performed on a standard lifting platform with an Olympic-size bar and rubber bumper plates. The parallel-squat position is defined as the subject's ability to lower a weight until the thigh is parallel to the floor and then return to the starting position. We instructed our subjects to ride a stationary bike for 5 minutes before performing the squat exercise. Each subject completed 2 repetitions at 60, 70, and 80% of a predicted 1-RM. After these 3 sets, subjects continued to complete 1 repetition, increasing the weight by 2.72-kg (5-lb) increments until either the parallel position could not be reached or the subject failed to return to the starting position.
Hydrostatic Weighing
Hydrostatic weighing was used to measure body density before (week 0) and after supplementation (week 10). Subjects reported to the underwater weighing tank in swimsuits. Body weight was first determined out of water by an electronic scale (model Toledo SL-39, Mettler Toledo Scales and Systems, Columbus, OH). Underwater weight was assessed by a force transducer (model 37–9.2, West Coast Research Co, Los Angeles, CA) connected by a transbridge (model TB-4, World Precision Instruments, Sarasota, FL), which was interfaced using Acknowledge software (version 3.0, BIOPAC System Inc, Goleta, CA) on a computer (Gateway 4DX2–66, Gateway, Inc, Sioux City, SD). Calibration was conducted daily by establishing linear interpolation from 2 known weights. Data points were recorded with data acquisition software, Acknowledge 3.0, from the force transducer. Subjects were submerged in warm water and asked to exhale a maximal amount of air while a signal from the force transducer produced a readable analog wave. The most stable waveform was selected, and the mean value was recorded. Subjects performed this procedure until at least 2 trials were within a 3% difference or a total of 10 trials was completed. If a 3% difference could not be obtained, mean values were calculated for the final underwater weight. Next, body density was calculated after weight was recorded in and out of water. The Siri equation was used to calculate percentage of body fat. Fat-free mass (FFM) was also calculated from the percentage of body fat.
Treatment of Data
Statistical analyses were performed using the Statistical Package for the Social Sciences for Windows software (version 8.0, SPSS, Inc, Chicago, IL). Our hypotheses were tested at an α level of .05. The 1-RM squat was measured before, during, and after supplementation. Urinary creatinine concentration was measured on days 0, 1, 3, 7, 14, 21, 28, 35, 42, 49, 56, and 63. Percentage of body fat was determined by hydrostatic weighing, and FFM was calculated before and after supplementation. All variables were analyzed between groups and over time by an analysis of variance with repeated measures. In addition, the Tukey pairwise comparison post hoc test for repeated measures was used for all data that showed significant differences.
RESULTS
Significant differences in absolute maximal strength were found over time with our periodized resistance training program (P = .001, F1,22 = 13.52); however, no group or interaction effects were noted (P = .232, F2,22 = 1.50) (Table 1). Each group showed significant increases: the low-dose group increased 19.03 kg, the loading group increased 8.80 kg, and the placebo group increased 8.83 kg (Figure 1). Using the post hoc pairwise comparison, we found that significant differences in absolute strength occurred before and during, during and after, and before and after supplementation.
Table 1.
Group Means ± SDs for 1-Repetition Maximum (1-RM) Strength, Percentage of Body Fat, and Fat-Free Mass*
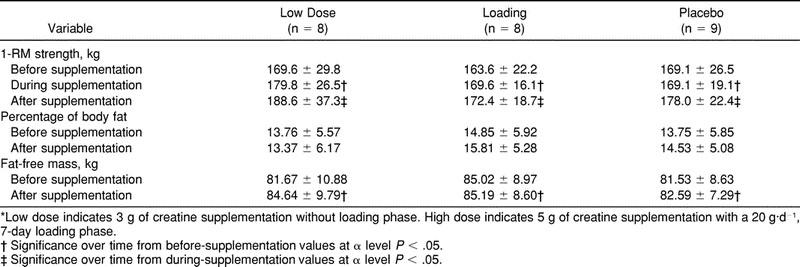
Figure 1.

Changes in 1-repetition maximum for the squat exercise among groups throughout 10 weeks of creatine supplementation or placebo.
When we analyzed urinary creatinine concentration output, we found a large amount of variation among subjects (Table 2). No statistically significant group, time, or interaction effects could be found (P = .751, F22,242 = .778). Initially, there was a nonsignificant decrease in urinary creatinine concentration at the beginning of supplementation for all groups (Figure 2). After initial ingestion, the low-dose and loading groups showed nonsignificant increases in creatinine concentration (0.034 μmol·L−1 and 0.057 μmol·L−1) on day 3. The placebo's group urinary creatinine concentration actually decreased from week 0 (−1.66 mg·dL−1) after day 3, but none of these values were statistically significant. At the end of the loading period, all groups continued to show similar urinary creatinine concentrations.
Table 2.
Urinary Creatinine Concentration (Mean ± SD)*
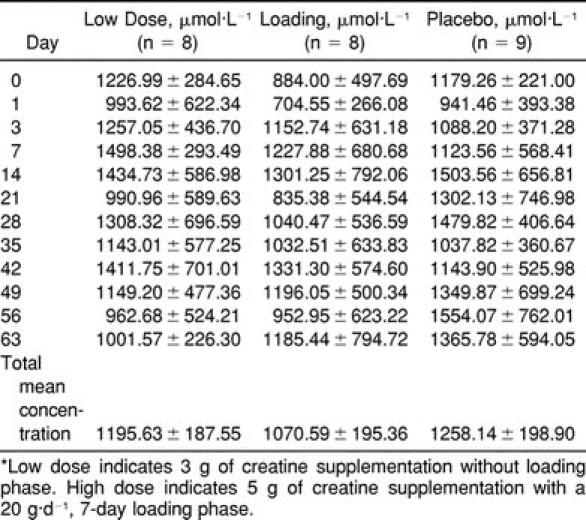
Figure 2.

Group changes in urinary creatinine concentration throughout 10 weeks of creatine supplementation or placebo.
Percentage of body fat was analyzed by hydrostatic weighing. The group, time, and interaction effects showed no significant differences (P = .52, F2,22 = .683) in hydrostatic weighing during 10 weeks of supplementation (Table 1). However, analysis of FFM showed significant differences over time (P = .037, F1,22 = 4.93) but no group or interaction effects occurred (P = .211, F2,22 = 1.67). The total change in FFM for the low-dose group was 2.46 kg, compared with 1.79 kg for the loading group and 1.16 kg for the placebo group.
DISCUSSION
Physiologically, creatine aids in recycling adenosine triphosphate (ATP) during short-term, high-intensity muscular work. Approximately 1 to 2 g of creatine is synthesized each day from the amino acids arginine, glycine, and methionine in the liver, kidneys, and pancreas.14,23–25 Once synthesized, creatine must be transported by the blood to the tissues within the body for storage and utilization. Approximately 95% of creatine is found in skeletal muscle. Of this amount, 60% is in the form of creatine phosphate, with the remainder in the form of free creatine.24 Some studies have indicated anabolic effects with short-term creatine loading; for example, 5 g 4 times a day may increase body mass, FFM, and strength.16,17 Although these effects have been well documented in the laboratory, low doses and loading doses of creatine need to be compared.
Creatine loading has been found to increase creatine phosphate stores within skeletal muscle; thus, the possibility exists for enhancing performance, especially in short-term work bouts, and enhancing recovery between sessions.2,6,25–30 Creatine loading is comparable with carbohydrate loading, in which the goal is to increase glycogen stores within the muscle during a week of high carbohydrate ingestion, However, it is possible that athletes are not just loading creatine for 1 week before competition but are ingesting high doses of creatine on a daily basis because of the proposed anabolic effects. Some research conducted on repeated anaerobic events has not shown performance enhancement,7–9 although studies on strength training have shown significant increases in 1-RM strength.8,16,19,31 We question whether or not creatine loading is necessary or even safe for athletes who are ingesting creatine habitually.
Our data suggest that creatine monohydrate use for 10 weeks did not produce any effects on 1-RM squat strength, urinary creatinine concentration, or body composition in collegiate football players. The 1-RM strength increased in all groups. Therefore, we believe that the periodized resistance training program was the cause of the strength increases. These results contradict the findings of other researchers of significant differences between creatine and placebo groups.4,5,17 In addition, the changes occurred throughout the entire 10 weeks. We did observe that the low-dose group had the greatest change in 1-RM values, but it was not significantly different from the other 2 groups. In addition, all groups increased FFM throughout 10 weeks of training. This increase in FFM may have allowed subjects to perform at higher intensities, thus increasing overall strength because more actin and myosin were available for binding, which in turn may have allowed greater force production. This explanation is supported by other findings of similar increases in FFM and maximal 1-RM strength.8,18 Furthermore, our subjects were highly trained athletes. We would expect this population to show minimal changes in strength compared with populations that are not involved in resistance training.
Creatinine formation is directly related to creatine phosphate concentration in skeletal muscle. Harris et al22 showed that creatine saturation in muscle was associated with elevated levels of urinary creatinine. This result suggests that the muscle cannot phosphorylate excess free creatine; therefore, excessive supplementation yields elevated urinary creatinine. Other researchers have used muscle biopsy to show that creatine loading (20 g·d−1) can increase creatine phosphate within muscle.13,20,22 Moreover, a relationship exists between creatine loading and increased urinary creatinine concentrations.19,20,22
In our study, urinary creatinine concentrations were measured throughout 10 weeks, and large variations were seen among subjects. These variations were also shown by Hultman et al,20 who found in addition that creatinine degradation was directly proportional to muscle creatine phosphate content. We did not evaluate total creatine phosphate concentration within skeletal muscle but attempted to determine if creatine supplementation would increase levels of creatine phosphate within the muscle, as indicated by elevated urinary creatinine 4 hours after ingestion and exercise. We did not observe any group, time, or interaction effects. Some variation did occur during the loading phase, although the loading group did not show increased urinary creatinine concentrations compared with the low-dose and placebo groups. We expected that the loading group might have elevated urinary creatinine concentrations because this group was ingesting higher doses of creatine (5 g 4 times a day) compared with other groups. At the end of week 1, the low-dose and loading groups had similar creatinine concentrations (3.07 and 3.89 mg·dL−1) when compared with the placebo group. This result is consistent with the finding of Hultman et al20 that lower doses of creatine produced similar effects to loading higher doses of creatine over time.
One possible explanation is that we did not collect 24-hour samples for analysis. It is possible that excess creatine was not excreted as creatinine within 4 hours of supplementation. It is also possible that creatine ingestion did not increase muscle creatine phosphate levels; we did not take biopsy specimens of the muscle and, therefore, were unable to accurately assess creatine phosphate levels. It is likely that our subjects were nonresponders, even though they had been free of creatine supplementation for 4 weeks before the study began. We did not monitor diet, and our subjects may have had previously elevated levels of creatine due to excessive protein ingestion. Finally, most of the creatine may have been converted to creatine phosphate and used during exercise. Our subjects were highly trained football players with large amounts of FFM, which may increase capacity for utilization of creatine phosphate. On the other hand, other tissues or organs (eg, liver or kidney) may be affected by elevated doses of creatine. Furthermore, hydration status may have an effect on creatinine concentration. We attempted to control hydration status by having the subjects drink only 300 mL of water during the 4 hours after creatine ingestion. We assumed that all subjects followed this procedure, but some subjects could have ingested more than 300 mL of fluid in the 4-hour window. In addition, it is very possible that the subjects' hydration status varied before workout sessions, which could have affected urinary creatinine concentration. These data suggest that creatine supplementation, with or without a loading phase, had no effect on urinary creatinine concentrations 4 hours after resistance training.
LIMITATIONS OF THE STUDY AND CONSIDERATIONS FOR FUTURE RESEARCH
We used a practical training design; therefore, our data differ slightly from other researchers' findings. We realize that our study does not support most of the published literature. Possible reasons that creatine supplementation did not cause significant effects are as follows. First, we did not take 24-hour urine samples to evaluate total urinary creatinine. Pre-exercise hydration status may have affected the urinary creatinine concentration 4 hours after exercise. Second, our creatinine data might have been more substantiated if we had taken muscle biopsy specimens to measure the current creatine levels of our subjects. Moreover, the possibilities of nonresponders and limited uptake in skeletal muscle are likely. Third, the subjects' diets were not monitored. Some of our subjects may have consumed more protein, which could have led to elevated creatine levels before supplementation. A high-protein diet may result in the ingestion of 3 or more g·d−1 of creatine, which could confound the effects of low-dose creatine supplementation. Fourth, the 1-RM squat exercise requires a single burst of energy that is fueled by the ATP-phosphocreatine (PC) energy system. Although significant strength gains did not occur among groups, the ingested creatine may still have had some effect in creatine phosphate resynthesis. To put further stress on the ATP-PC energy system, repeated anaerobic resistive exercises could be used to determine if creatine supplementation can affect creatine phosphate resynthesis.
Future studies should emphasize highly trained male and female athletes in controlled, sport-specific settings. Hydration status during exercise should be specifically addressed; 24-hour urine samples should be taken for more accurate measurement of creatine and creatinine levels; and muscle biopsy specimens should be taken to determine the actual relationship between creatine phosphate and urinary creatinine levels. In addition, future researchers should monitor protein intake, especially in the form of red meats, and use a repeated anaerobic exercise, such as a repeated maximal squat, to tax the ATP-PC energy system. Finally, longitudinal studies are needed to determine if creatine causes adverse effects that may hinder athletic performance or cause injury or illness.
In conclusion, our main findings are that lower doses and loading creatine had no significant effects on 1-RM strength, urinary creatinine concentration, or percentage of body fat. Also, increases in 1-RM strength and FFM did occur throughout the entire periodized resistance training program. Hence, a periodized resistance training program without creatine supplementation was sufficient to produce changes in 1-RM strength and increased FFM in highly trained collegiate football players.
ACKNOWLEDGMENTS
We thank NutraSense Co (Shawnee Mission, KS) and Jon Scott for the donation of Createam Chewable Tablets for this project and the School of Recreation and Sport Sciences for supporting funds. Finally, thanks to Ohio University Head Football Coach Jim Grobe and his staff for supporting this project.
REFERENCES
- 1.Balsom PD, Ekblom B, Söderlund K, Sjodin B, Hultman E. Creatine supplementation and dynamic high intensity intermittent exercise. Scand J Med Sci Sports. 1993;3:143–149. [Google Scholar]
- 2.Casey A, Constantin-Theodosiu D, Howell S, Hultman E, Greenhaff PL. Creatine ingestion favorably affects performance and muscle metabolism during maximal exercise in humans. Am J Physiol. 1996;271(1 pt 1):E31–E37. doi: 10.1152/ajpendo.1996.271.1.E31. [DOI] [PubMed] [Google Scholar]
- 3.Ekblom B. Effects of creatine supplementation on performance. Am J Sports Med. 1996;24(suppl 6):S38–S39. [PubMed] [Google Scholar]
- 4.Becque MD, Lochmann JD, Melrose D. Effects of creatine supplementation during strength training on 1RM and body composition. Med Sci Sports Exerc. 1997;27(suppl):146. doi: 10.1097/00005768-200003000-00016. [DOI] [PubMed] [Google Scholar]
- 5.Earnest CP, Snell PG, Rodriguez R, Almada AL, Mitchell TL. The effect of creatine monohydrate ingestion on anaerobic power indices, muscular strength and body composition. Acta Physiol Scand. 1995;153:207–209. doi: 10.1111/j.1748-1716.1995.tb09854.x. [DOI] [PubMed] [Google Scholar]
- 6.Dawson B, Cutler M, Moody A, Lawerence S, Goodman C, Randall N. Effects of oral creatine loading on single and repeated maximal short sprints. Aust J Sci Med Sport. 1995;27:56–61. [PubMed] [Google Scholar]
- 7.Burke LM, Pyne DB, Telford RD. Effect of oral creatine supplementation on single-effort sprint performance in elite swimmers. Int J Sport Nutr. 1996;6:222–233. doi: 10.1123/ijsn.6.3.222. [DOI] [PubMed] [Google Scholar]
- 8.Cooke WH, Grandjean PW, Barnes WS. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J Appl Physiol. 1995;78:670–673. doi: 10.1152/jappl.1995.78.2.670. [DOI] [PubMed] [Google Scholar]
- 9.Mujika I, Chatard JC, Lacoste L, Barale F, Geyssant A. Creatine supplementation does not improve sprint performance in competitive swimmers. Med Sci Sports Exerc. 1996;28:1435–1441. doi: 10.1097/00005768-199611000-00014. [DOI] [PubMed] [Google Scholar]
- 10.Odland ML, MacDougall JD, Tarnopolsky MA, Elorriaga A, Borgmann A. Effect of oral creatine supplementation on muscle [Pcr] and short-term maximum power output. Med Sci Sports Exerc. 1997;29:216–219. doi: 10.1097/00005768-199702000-00008. [DOI] [PubMed] [Google Scholar]
- 11.Ziegenfuss TN, Lemon P, Rogers MR, Ross R, Yarasheski YE. Acute creatine ingestion: effects on muscle volume, anaerobic power, fluid volumes, and protein turnover. Med Sci Sports Exerc. 1995;27(suppl):127. [Google Scholar]
- 12.Plisk SS, Kreider RB. Creatine controversy? Strength Condition J. 1999;21:14–23. [Google Scholar]
- 13.Greenhaff PL, Bodin K, Soderlund K, Hultman E. Effect of oral creatine supplementation on skeletal muscle phosphocreatine resynthesis. Am J Physiol. 1994;266(5 pt 1):E725–E730. doi: 10.1152/ajpendo.1994.266.5.E725. [DOI] [PubMed] [Google Scholar]
- 14.Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E. Influence of oral creatine supplementation of muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci (Colch) 1993;84:565–571. doi: 10.1042/cs0840565. [DOI] [PubMed] [Google Scholar]
- 15.Johnson KD, Smodic B, Hill R. The effects of creatine monohydrate supplementation on muscular power and work. Med Sci Sports Exerc. 1997;29:S251. [Google Scholar]
- 16.Noonan D, Berg K, Latin RW, Wagner JC, Reimers K. Effects of varying dosages of oral creatine relative to fat-free body mass on strength and body composition. J Strength Condition Res. 1998;12:104–108. [Google Scholar]
- 17.Kelly VG, Jenkins DG. Effects of oral creatine supplementation on near maximal strength and repeated sets of high intensity bench press exercise. J Strength Condition Res. 1998;12:109–115. [Google Scholar]
- 18.Peeters BM, Lantz CD, Mayhew JL. Effects of oral creatine monohydrate and creatine phosphate supplementation on maximal strength indices, body composition, and blood pressure. J Strength Condition Res. 1999;13:3–9. [Google Scholar]
- 19.Vandenberghe K, Goris M, Van Hecke P, Leemputte M, Vangerven L, Hespel P. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol. 1997;83:2055–2063. doi: 10.1152/jappl.1997.83.6.2055. [DOI] [PubMed] [Google Scholar]
- 20.Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol. 1996;81:232–237. doi: 10.1152/jappl.1996.81.1.232. [DOI] [PubMed] [Google Scholar]
- 21.Rossiter HB, Cannell ER, Jakeman PM. The effect of oral creatine supplementation on the 1000-m performance of competitive rowers. J Sports Sci. 1996;14:175–179. doi: 10.1080/02640419608727699. [DOI] [PubMed] [Google Scholar]
- 22.Harris RC, Soderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci (Colch) 1992;83:367–374. doi: 10.1042/cs0830367. [DOI] [PubMed] [Google Scholar]
- 23.Clark JF. Creatine and phosphocreatine: a review of their use in exercise and sport. J Athl Train. 1997;32:45–51. [PMC free article] [PubMed] [Google Scholar]
- 24.Volek JS, Boetes M, Bush JA, Putukian M, Sebastianelli WJ, Kraemer WJ. Response of testosterone and cortisol concentrations to high-intensity resistance exercise following creatine supplementation. J Strength Condition Res. 1997;11:182–187. [Google Scholar]
- 25.Greenhaff PL. Creatine and its application as an ergogenic aid. Int J Sport Nutr. 1995;5:S100–S110. doi: 10.1123/ijsn.5.s1.s100. [DOI] [PubMed] [Google Scholar]
- 26.Balsom PD, Soderlund K, Sjodin B, Ekblom B. Skeletal muscle metabolism during short duration high-intensity exercise: influence of creatine supplementation. Acta Physiol Scand. 1995;154:303–310. doi: 10.1111/j.1748-1716.1995.tb09914.x. [DOI] [PubMed] [Google Scholar]
- 27.Greenhaff PL, Contantin-Teodosiu D, Casey A, Hultman E. The effect of oral creatine supplementation on skeletal muscle ATP degradation during repeated bouts of maximal voluntary exercise in man. J Physiol. 1994;476:84P. [Google Scholar]
- 28.Birch R, Noble D, Greenhaff PL. The influence of dietary creatine supplementation on performance during repeated bouts of maximal isokinetic cycling in man. Eur J Appl Physiol Occup Physiol. 1994;69:268–276. doi: 10.1007/BF01094800. [DOI] [PubMed] [Google Scholar]
- 29.Dawson B, Goodman C, Lawrence S, et al. Muscle phosphocreatine repletion following single and repeated short sprint efforts. Scand J Med Sci Sports. 1997;7:206–213. doi: 10.1111/j.1600-0838.1997.tb00141.x. [DOI] [PubMed] [Google Scholar]
- 30.Vandenberghe K, Van Hecke P, Van Leemputte M, Vanstapel F, Hespel P. Phosphocreatine resynthesis is not affected by creatine loading. Med Sci Sports Exerc. 1999;31:236–242. doi: 10.1097/00005768-199902000-00006. [DOI] [PubMed] [Google Scholar]
- 31.Kreider RB, Ferreira M, Wilson M, et al. Effects of creatine supplementation on body composition, strength, and sprint performance. Med Sci Sports Exerc. 1998;30:73–82. doi: 10.1097/00005768-199801000-00011. [DOI] [PubMed] [Google Scholar]