

Abstract
Purpose
We compared the prevalence of urinary incontinence by type among white, black, Hispanic and Asian-American women.
Materials and Methods
The RRISK is a population based cohort study of 2,109 randomly selected middle-aged and older women. Incontinence and other variables were assessed by self-report questionnaires and in person interviews. Labor and delivery and surgical data were abstracted from medical records archived since 1946. Logistic regression was used to estimate the OR with 95% CIs for incontinence while adjusting for covariates.
Results
The age adjusted prevalence of weekly incontinence was highest among Hispanic women, followed by white, black and Asian-American women (36%, 30%, 25% and 19%, respectively, p >0.001). Type of incontinence also differed among groups, with weekly stress incontinence prevalence being 18%, 15%, 8% and 8% (p >0.001), and weekly urge incontinence prevalence being 10%, 9%, 14% and 7% (p >0.001). After adjustment for age, parity, hysterectomy, estrogen use, body mass, menopausal status and diabetes, the risk of stress incontinence remained significantly lower in black (adjusted OR 0.36, 95% CI 0.23–0.57) and Asian-American (adjusted OR 0.54, 95% CI 0.34–0.86) women compared to white women. In contrast, the risk of urge incontinence was similar in black (adjusted OR 1.19, 95% CI 0.79–1.81) and Asian-American (adjusted OR 0.86, 95% CI 0.52–1.43) women compared to white women.
Conclusions
Significant differences in the adjusted risk of stress incontinence among Hispanic, white, black and Asian-American women suggest the presence of additional, as yet unrecognized, risk or protective factors for stress incontinence.
Keywords: urinary incontinence, epidemiology, ethnic groups, risk, women's health
Ascertaining the prevalence of female urinary incontinence by frequency, severity and type among different racial/ethnic groups is necessary to more fully understand the scope of incontinence in the United States population. In addition, identifying differences in the prevalence of incontinence among groups may lead to a better understanding of the etiology of incontinence. However, most studies to date have been limited to white women. The few studies comparing incontinence prevalence among racial/ethnic groups have been limited by lack of adjustment for known or suspected risk factors for incontinence,1-3 use of selected populations (eg from referral centers),4,5 comparison of only 2 racial/ethnic groups (eg white vs black)5-7 or lack of differentiation by type of incontinence (stress vs urge).1,8-10 Comparing incontinence prevalence among racial/ethnic groups ascertained in separate studies is problematic since any differences could be due to differences in incontinence definition, population selection or study design. To address these limitations we conducted the RRISK, a population based study of middle-aged and older women, to ascertain differences in incontinence prevalence, overall and by type, among the major racial/ethnic groups.
MATERIALS AND METHODS
The RRISK was conducted within the Kaiser Permanente Medical Care Program of Northern California, an integrated health care delivery system with more than 3 million members or about 25% of the population in the area served. Previous studies have found members to underrepresent the poor and the wealthy, and to be slightly more educated, but to be similar to the population in the geographic area served with respect to other demographic characteristics including race/ethnicity.11
The study cohort was constructed by first identifying women between 40 and 69 years old as of January 1, 1999. Because we required that women had at least half of their births within Kaiser (and therefore would have labor and delivery records available), we identified those women who had been members of Kaiser since age 18 using computerized membership files. From this group of approximately 66,000 female members, we randomly sampled 10,230 women within age and race strata with a goal of obtaining an approximately equal number of women in each 5-year age group with a race/ethnicity composition of 20% black, 20% Hispanic, 20% Asian-American and 40% white (non-Hispanic). Figure 1 shows the recruitment and enrollment process. Among the 8,835 women whose eligibility could be determined, 6,018 (68.9%) were ineligible and 2,817 (31.9%) were eligible (fig. 1). Applying the 31.9% eligible to the 1,326 women of unknown eligibility yielded an estimated additional 423 eligible women, bringing the estimated total of eligible women in the original sample to 3,240, of which we enrolled 2,109 (65.1%).
Fig 1.
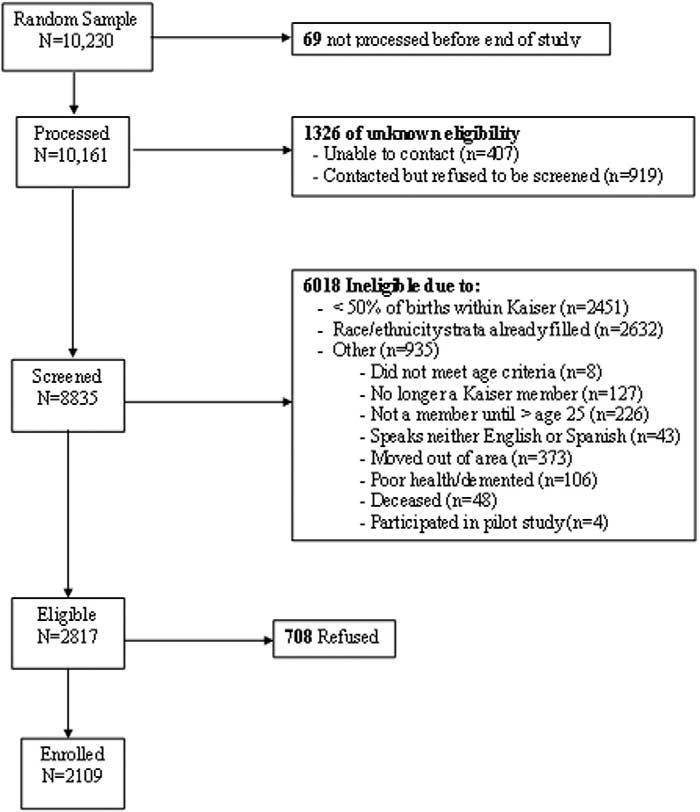
Flowchart showing recruitment of subjects for RRISK
Data were collected by preinterview questionnaire and in person interview. Interviewers were all women, and a bilingual interviewer was available for women who preferred to be interviewed in Spanish. Interviewers made a specific point of reviewing participant answers to questions about incontinence, rephrasing if needed and clarifying response inconsistencies. Women who reported current incontinence at least weekly were asked about incontinence frequency and clinical type. Additional data collected included demographic characteristics, medical and surgical history (including hysterectomy), current medications and history of hormone use. Menopausal status was obtained by self-report, which is considered reliable for these variables,12 rather than using chart derived data. Body mass index (kg/m2) was calculated based on participant weight and height measured at the time of the interview.
Current incontinence was defined as at least 1 episode in the last 12 months, and was further characterized as less than monthly, monthly, weekly and daily. Severity was determined based on incontinence frequency and amount of urine lost per episode using the validated Sandvik Severity score.13,14 Additional incontinence questions to determine incontinence type were similar to those used in a previous large observational study,13 and were validated and shown to be reliable.15,16 Women with at least weekly incontinence were asked to recall the number of incontinence episodes in the last 7 days that occurred “with an activity like coughing, lifting, sneezing or exercise” (stress incontinence) and the number of episodes accompanied by “a physical sense of urgency” (urge incontinence). Incontinence not associated with either an activity or sense of urgency was characterized as “other incontinence.” Women with only other incontinence (34) were excluded from the analyses by incontinence type.
For purposes of risk factor analysis, women were classified as having stress incontinence if they reported only stress incontinence or mixed incontinence with the majority of episodes being stress, and as having urge incontinence if they reported only urge incontinence or mixed incontinence with the majority of the episodes being urge. For these analyses the comparison group was comprised of continent women, defined as participants who reported never having had incontinence at least once per month for at least 3 months in a row.
The prevalence of potential risk factors for incontinence among racial/ethnic groups was age adjusted using direct standardization of the overall RRISK age distribution and compared using logistic models or proportional odds models to adjust for age. The univariate associations of potential risk factors (including all the variables in table 1) for incontinence were investigated using age adjusted logistic or proportional odds models. Variables associated with incontinence at p ≤0.2 in models adjusting only for age were evaluated for inclusion in a multiple logistic regression model. Variables whose inclusion resulted in a meaningful (generally 10% or greater) change in the estimated association between any racial/ethnic group and incontinence were retained in the model.17 Age and parity were included by default in all models. Continuous variables were also assessed as categorical variables to maximize the opportunity for detecting confounding. The largest group, white women, was used as the reference group. Results are presented as OR and 95% CI. All analyses were performed with SAS® version 8.02.
Table 1.
Characteristics of participants by percent
| % White Women (1,003) | %Hispanic Women (350) | % Black Women (383) | % Asian-American Women (345) | |
|---|---|---|---|---|
| Married/living as married | 71.6 | 74.6 | 51.4 | 76.8 |
| Education: | ||||
| High school or less | 18.5 | 35.7 | 13.2 | 15.1 |
| Some college or technical school | 42.5 | 46.0 | 57.4 | 36.8 |
| College graduate | 23.6 | 12.6 | 18.8 | 32.8 |
| Graduate school | 15.3 | 5.4 | 10.4 | 15.4 |
| Age: | ||||
| 40–49 | 23.0 | 31.8 | 30.5 | 36.2 |
| 50–59 | 32.3 | 48.1 | 36.3 | 45.2 |
| 60 Yrs or older | 44.8 | 19.9 | 33.1 | 18.5 |
| Total household income: | ||||
| Less than $40,000 | 22.4 | 22.3 | 29.2 | 14.8 |
| $40,000–$59,999 | 20.3 | 22.0 | 26.9 | 13.6 |
| $60,000–$79,999 | 19.3 | 22.3 | 18.5 | 18.3 |
| $80,000–$99,999 | 30.2 | 26.0 | 20.7 | 42.6 |
| Occupation: | ||||
| Employed full or part-time | 57.1 | 73.4 | 68.2 | 73.9 |
| Retired, student or homemaker | 38.8 | 21.7 | 25.9 | 20.9 |
| Unemployed/other | 3.9 | 4.6 | 6.0 | 5.2 |
| Parity: | ||||
| 0 Births | 19.1 | 14.3 | 17.8 | 20.6 |
| 1 Birth | 8.8 | 8.9 | 14.9 | 12.5 |
| 2 Births | 31.8 | 24.6 | 26.4 | 35.4 |
| 3 or More births | 39.9 | 52.0 | 41.0 | 31.0 |
RESULTS
Demographic characteristics of the 2,109 women in the study are presented in table 1. Slightly less than half of the women self-identified as white, with the remaining half approximately equally divided among black, Hispanic and Asian-American identification. A total of 28 women did not select any of these categories and are not included in the results. Mean age was 56 ± 8.6 years and median household income was $60,000 to $79,000. Data from 489 of the eligible, nonenrolled women showed these women to be similar to enrolled women with respect to mean age (53.8 vs 53.1), years of membership at Kaiser (41.6 vs 41.0), number of births (2.3 vs 2.2) and proportion of births within Kaiser (87% vs 87%). However, nonenrolled women were substantially less likely to be white (28.0% vs 47.6%, p >0.001) and were half as likely to report being incontinent at every frequency level (p >0.001 at all frequencies).
As shown in table 2, the prevalence of incontinence in the last year varied by race/ethnicity. The prevalence of daily incontinence varied 2-fold from 8.5% in Asian-American women to more than 17.2% in Hispanic women (p >0.001). The prevalence of severe incontinence mirrored the pattern shown for daily incontinence (p >0.001).
Table 2.
Prevalence of urinary incontinence in last 12 months by frequency and severity, adjusted for age
| % (95% CI) |
|||||
|---|---|---|---|---|---|
| White Women | Hispanic Women | Black Women | Asian-American Women | p Value | |
| Incontinence frequency: | |||||
| Any incontinence | 73.3 (71.4–75.2) | 74.8 (73.0–76.7) | 64.8 (62.8–66.9) | 68.8 (66.9–70.8) | 0.0068 |
| Monthly or more | 45.0 (42.9–47.1) | 51.0 (48.9–53.1) | 36.8 (34.7–38.9) | 33.7 (31.7–35.8) | <0.0001 |
| Wkly or more | 29.6 (27.7–31.6) | 35.9 (33.9–38.0) | 25.2 (23.3–27.0) | 19.0 (17.3–20.7) | <0.0001 |
| Daily | 12.1 (10.7–13.5) | 17.2 (15.6–18.8) | 11.8 (10.4–13.2) | 8.5 (7.3–9.7) | 0.0077 |
| Incontinence severity:* | |||||
| Moderate† | 21.2 (19.4–23.0) | 24.0 (22.1–25.8) | 17.9 (16.2–19.5) | 13.8 (12.3–15.2) | |
| Severe/very severe‡ | 8.3 (7.1–9.5) | 11.7 (10.3–13.1) | 7.3 (6.2–8.4) | 5.2 (4.3–6.2) | 0.50 |
Severity was determined only for women with at least weekly incontinence.
Moderate refers to daily incontinence of a few drops or weekly incontinence which wets underwear or crotch of pants.
Severe/very severe refers to weekly or daily incontinence which wets pants or floor.
Figure 2 shows the prevalence of stress and urge incontinence in the last week by group. Asian-American women reported relatively low levels of stress and urge incontinence, while white and Hispanic women reported relatively high levels of both. In contrast, black women had less stress incontinence than all other groups but had the highest prevalence of urge incontinence. This pattern was similar when type was defined as stress only, mixed predominately stress, urge only and mixed predominately urge (table 3). Table 4 shows the distribution of potential risk factors for urinary incontinence by racial/ethnic group adjusted for age because white women were slightly older (mean age 58.0 years) than Hispanic (53.5), black (55.0) and Asian-American (53.2 years) women.
Fig 2.
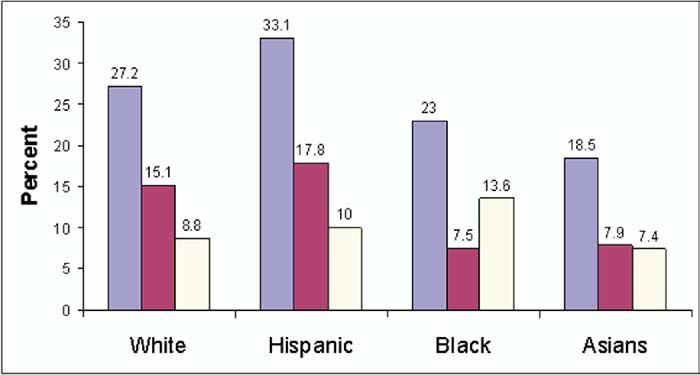
Prevalence of weekly urinary incontinence by type in each racial/ethnic group, adjusted for age. Dark blue indicates any incontinence, red stress incontinence and yellow urge incontinence.
Table 3.
Prevalence of urinary incontinence at least weekly by type, adjusted for age
| % (95% CI) |
|||||
|---|---|---|---|---|---|
| White Women | Hispanic Women | Black Women | Asian-American Women | p Value | |
| Stress only | 7.2 (6.1–8.3) | 9.0 (7.7–10.2) | 2.3 (1.7–3.0) | 3.4 (2.6–4.2) | <0.0001 |
| Mixed, predominately stress | 7.9 (6.7–9.1) | 8.8 (7.6–10.0) | 5.2 (4.3–6.2) | 4.5 (3.6–5.4) | 0.035 |
| Urge only | 4.8 (3.9–5.7) | 5.8 (4.8–6.8) | 7.6 (6.5–8.8) | 3.0 (2.3–3.8) | 0.027 |
| Mixed, predominately urge | 4.0 (3.1–4.8) | 4.2 (3.3–5.0) | 6.0 (5.0–7.1) | 4.4 (3.5–5.2) | Not significant |
| Mixed, equal stress & urge | 3.3 (2.5–4.1) | 5.3 (4.3–6.3) | 1.9 (1.3–2.5) | 3.2 (2.5–4.0) | Not significant |
Table 4.
Frequency of potential risk factors for incontinence by race/ethnicity, adjusted for age
| Potential Risk Factor | White Women | Hispanic Women | Black Women | Asian-American Women | p Value |
|---|---|---|---|---|---|
| % Nulliparous | 21.3 | 13.9 | 17.5 | 19.7 | <0.001 |
| % Parity: | |||||
| 1 | 9.0 | 7.9 | 14.8 | 12.5 | |
| 2 | 32.7 | 22.7 | 26.4 | 32.9 | |
| 3 | 23.2 | 31.8 | 23.9 | 24.0 | |
| 4+ | 13.8 | 23.7 | 17.5 | 11.0 | <0.001* |
| Mean parity ± SD | 2.2 ± 1.6 | 2.5 ± 1.5 | 2.2 ± 1.6 | 1.9 ± 1.4 | <0.001 |
| Mean age at first birth ± SD | 24.3 ± 4.3 | 23.5 ± 4.5 | 23.3 ± 4.9 | 25.5 ± 4.9 | <0.001 |
| % Menopausal | 65.4 | 65.5 | 69.4 | 61.3 | 0.013 |
| % Hysterectomy | 20.8 | 23.9 | 32.1 | 15.8 | <0.001 |
| % Current oral estrogen | 33.9 | 36.4 | 23.5 | 25.6 | <0.001 |
| % Body mass index (kg/m2): | |||||
| Less than 25 | 41.0 | 28.7 | 17.7 | 55.6 | |
| 25–30 | 27.3 | 27.2 | 25.2 | 26.2 | |
| 30 or Greater | 31.7 | 44.1 | 57.1 | 18.3 | <0.001* |
| Mean body mass index ± SD | 28.0 ± 6.7 | 29.6 ± 6.5 | 31.8 ± 7.2 | 25.9 ± 5.2 | <0.001 |
| % Medical conditions: | |||||
| 1 or More urinary tract infections in last yr | 12.7 | 17.6 | 9.8 | 9.4 | 0.003 |
| Diabetes | 4.8 | 13.1 | 11.2 | 11.4 | <0.001 |
| % Other conditions: | |||||
| Smoking (current) | 9.0 | 8.3 | 16.8 | 6.6 | <0.001 |
| Alcohol 1 drink/wk or more | 37.0 | 21.1 | 15.2 | 11.2 | <0.001 |
Differences across all categories.
Multivariate modeling was used to ascertain to what extent differences by racial/ethnic group persisted after adjustment as indicated for the covariates presented in table 4. After adjustment for other covariates (table 5), the risk of weekly incontinence remained significantly lower in Asian-American and black women, and higher among Hispanic women, compared to white women. This difference was largely due to the lower risk of stress incontinence in Asian-American and black women. When the data were examined with stress incontinence defined as stress only and urge incontinence defined as urge only, the results were essentially the same as shown in table 5 (additional data not shown).
Table 5.
Adjusted association between race/ethnicity and weekly incontinence
| Race/Ethnic Group | OR (95% CI)* | OR (95% CI)† |
|---|---|---|
| All incontinence: | ||
| White | Reference | Reference |
| Hispanic | 1.53 (1.15–2.03) | 1.40 (1.03–1.89) |
| Black | 0.78 (0.59–1.04) | 0.61 (0.45–0.83) |
| Asian-American | 0.59 (0.43–0.81) | 0.68 (0.49–0.96) |
| Stress incontinence:‡ | ||
| White | Reference | Reference |
| Hispanic | 1.56 (1.10–2.21) | 1.42 (0.98–2.06) |
| Black | 0.46 (0.30–0.70) | 0.36 (0.23–0.57) |
| Asian-American | 0.46 (0.29–0.72) | 0.54 (0.34–0.86) |
| Urge incontinence:§ | ||
| White | Reference | Reference |
| Hispanic | 1.45 (0.92–2.28) | 1.37 (0.85–2.19) |
| Black | 1.47 (1.00–2.16) | 1.19 (0.79–1.81) |
| Asian-American | 0.78 (0.48–1.26) | 0.86 (0.52–1.43) |
Adjusted for age (5-year increments).
Adjusted for age (5-year increments), parity (0, 1, 2+), prior hysterectomy (Y/N), estrogen use (current/not current), body mass index (continuous), post-menopausal (Y/N), diabetes (Y/N).
Defined as only stress incontinence or mixed incontinence with the majority of episodes being stress.
Defined as only urge incontinence or mixed incontinence with the majority of the episodes being urge.
Comparisons were also made among other racial/ethnic groups. For example, with black women as the referent group, Hispanic women were nearly 4 times as likely to have stress incontinence (adjusted OR 3.9, 95% CI 2.4–6.5). There were no significant differences in risk of incontinence of either type between black and Asian-American women.
Because our sample of eligible but nonenrolled women was less likely to be white and less likely to report incontinence, we conducted additional analyses to estimate the impact of including these women on the prevalence of incontinence. Including these women in our sample would have reduced the prevalence of weekly incontinence from 29.6% to 26.0% in white women, from 36.0% to 25.5% in Hispanic women, from 25.3% to 17.0% in black women and from 19.1% to 14.3% in Asian-American women. Prevalence of incontinence by frequency, recalculated adjusting for the estimated response bias, is shown in figure 3. The prevalence of weekly incontinence was virtually identical in white and Hispanic women, but was significantly lower in black and Asian-American women compared to white and Hispanic women (p <0.001).
Fig. 3.
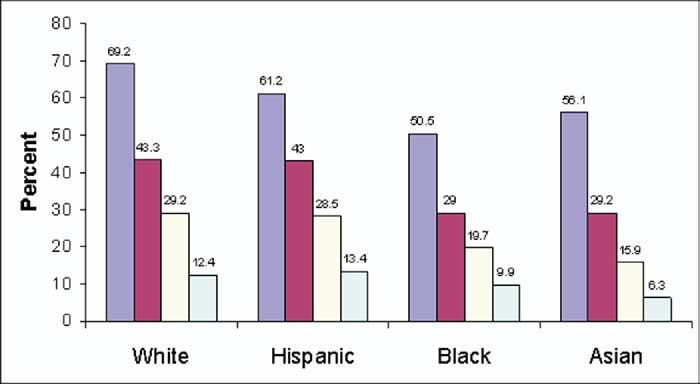
Prevalence of urinary incontinence by frequency in each racial/ethnic group after adjustment for potential effect of response bias. Dark blue indicates any incontinence in last 12 months, red incontinence at least once per month, yellow incontinence at least once per week and light blue daily incontinence.
DISCUSSION
The diversity of our large population based RRISK cohort provides a unique opportunity to examine differences in incontinence among 4 major racial/ethic groups within 1 study. To the best of our knowledge, this report is the first population based study with all major racial/ethnic groups to ascertain incontinence by type, thereby avoiding the problems inherent in comparing incontinence prevalence across studies. We found significant differences in the prevalence of incontinence in the last year with Hispanic women having the highest prevalence, followed by white, black and Asian-American women. After adjustment for multiple risk factors, white women appeared to have almost twice the risk of stress incontinence as Asian-American women, and almost 3 times the risk of black women, while differences in the risk of urge incontinence were relatively small and nonsignificant.
In contrast to our results, other recent studies have reported a lower prevalence of incontinence among Hispanic women.1,8,10 These discrepant findings between other studies and our study may be due to differences in the age of the populations studied, definitions of incontinence, or ascertainment of incontinence. Ethnic group composition may have also contributed to the variation in studies. For example, the composition of our Hispanic population was mostly of Mexican origin while in other studies the Hispanic women were from the Caribbean.8 Further studies of variations within subsets of the same racial/ethnic group would be helpful.
We found incontinence to be more prevalent in white women than in black women, a finding consistent with previous population based studies,2,3,6,7,9,10 including studies that used multivariate analysis to adjust for incontinence risk factors.6,7,9,10 This result is particularly noteworthy in that black women are more likely to have risk factors for incontinence, including obesity, diabetes, smoking and hysterectomy.
We found lower rates of stress incontinence among black women, but higher rates of urge incontinence compared to white women. This finding of a relative predominance of urge incontinence in black patients is consistent with the results of at least 1 other large epidemiological study6 and with studies of patients referred for urogynecological evaluation.4,18 This demonstrates the importance of characterizing incontinence by type in that simply comparing the overall prevalence of incontinence can be misleading when stress and urge incontinence differ in opposite ways.
A few studies have compared physiological parameters between black and white19 or Indian20 women to explain the lower prevalence of stress incontinence in black women. These studies have reported black women to have higher urethral closure pressure, greater urethral length and pubococcygeal muscle strength, larger urethral volume and, paradoxically, greater vesical mobility.19,20 The extent to which these differences, if confirmed, can explain differences in the prevalence of stress incontinence is not yet clear.
We found a substantially lower prevalence of stress and urge incontinence in Asian-American compared to white or Hispanic women. However, in the multivariate model this difference remained significant only for stress incontinence, with Asian-American women having a nearly 50% lower risk than white women. Two studies have reported Asian-American women as having a lower prevalence of incontinence compared to white women, but neither study examined incontinence by type or adjusted for other variables.8,10
While we cannot rule out the possibility of differential underreporting of incontinence among the race/ethnicity groups, we took several steps to minimize underreporting in general. Women were initially asked about accidental leakage of urine on the self-administered questionnaire to minimize underreporting due to embarrassment. Women who reported never having accidentally leaked urine were asked about urine leakage by the interviewer, using medical and vernacular terms, to be sure they understood the question. For women who did report incontinence, the questions to determine frequency and type of incontinence were asked by the interviewer, who clarified the questions if needed and checked answers for consistency.
Our study had several limitations that should be considered when interpreting the results. As in previous large epidemiological studies, incontinence in the current study was defined by self-report. While the questions used to distinguish between stress and urge incontinence have been shown to correlate reasonably well with urodynamic classification15 and to be reproducible,16 there are inevitable differences between self-report, urodynamic classification and clinical diagnosis in characterizing the presence, severity and type of urinary incontinence, as each are effectively measuring different, although related, phenomena. We do not know if using clinical or urodynamic definitions of stress and urge incontinence would result in the same associations with race/ethnicity.
Another limitation was a bias toward enrolling women with incontinence. Correcting for this bias moved the prevalence of incontinence in Hispanic women to that of white women, but it increased the differences between white women and Asian or black women, and did not affect our conclusions. Finally, we enrolled women who had been long-term members of a large prepaid health delivery system. Before initiating the study we determined that women who were members since age 18 were similar to all women members of the same age with respect to multiple characteristics, including the number of office visits in the last 27 months, prior hysterectomy and use of hormone replacement therapy. However, this aspect of our study should be considered in generalizing our results to other populations.
CONCLUSIONS
The differences in the prevalence of stress incontinence found in the current study suggest that additional studies of urodynamic function, anatomical measures and physiological factors in a representative sample of women in each group could be informative. In addition, future studies should search for additional risk of protective factors that vary by race/ethnicity. Identifying additional exposures or physiological factors may help to further our understanding and ultimately reduce the burden of urinary incontinence in the population.
Abbreviations and Acronyms
- CI
confidence interval
- OR
odds ratio
- RRISK
Reproductive Risks of Incontinence Study at Kaiser
Footnotes
RRISK supported by National Institute of Diabetes and Digestive and Kidney Diseases Grant R01-DK53335.
Presented at annual meeting of American Urological Association, San Francisco, California, May 8–13, 2004.
REFERENCES
- 1.Nygaard I, Turvey C, Burns TL, Crischilles E, Wallace R. Urinary incontinence and depression in middle-aged United States women. Obstet Gynecol. 2003;101:149. doi: 10.1016/s0029-7844(02)02519-x. [DOI] [PubMed] [Google Scholar]
- 2.Fultz NH, Herzog AR, Raghunathan TE, Wallace RB, Diokno AC. Prevalence and severity of urinary incontinence in older African American and Caucasian women. J Gerontol A Biol Sci Med Sci. 1999;54:M299. doi: 10.1093/gerona/54.6.m299. [DOI] [PubMed] [Google Scholar]
- 3.Burgio KL, Matthews KA, Engel BT. Prevalence, incidence and correlates of urinary incontinence in healthy, middle-aged women. J Urol. 1991;146:1255. doi: 10.1016/s0022-5347(17)38063-1. [DOI] [PubMed] [Google Scholar]
- 4.Duong TH, Korn AP. A comparison of urinary incontinence among African American, Asian-American, Hispanic and white women. Am J Obstet Gynecol. 2001;184:1083. doi: 10.1067/mob.2001.115221. [DOI] [PubMed] [Google Scholar]
- 5.Mattox TF, Bhatia NN. The prevalence of urinary incontinence or prolapse among white and Hispanic women. Am J Obstet Gynecol. 1996;174:646. doi: 10.1016/s0002-9378(96)70443-x. [DOI] [PubMed] [Google Scholar]
- 6.Brown JS, Grady D, Ouslander JG, Herzog AR, Varner RE, Posner SF. Prevalence of urinary incontinence and associated risk factors in postmenopausal women. Heart & Estrogen/Progestin Replacement Study (HERS) Research Group. Obstet Gynecol. 1999;94:66. doi: 10.1016/s0029-7844(99)00263-x. [DOI] [PubMed] [Google Scholar]
- 7.Jackson RA, Vittinghoff E, Kanaya AM, Miles TP, Resnick HE, Kritchevsky SB, et al. Urinary incontinence in elderly women findings from the Health, Aging, and Body Composition Study. Obstet Gynecol. 2004;104:301. doi: 10.1097/01.AOG.0000133482.20685.d1. [DOI] [PubMed] [Google Scholar]
- 8.Sampselle CM, Harlow SD, Skurnick J, Brubaker L, Bondarenko I. Urinary incontinence predictors and life impact in ethnically diverse perimenopausal women. Obstet Gynecol. 2002;100:1230. doi: 10.1016/s0029-7844(02)02241-x. [DOI] [PubMed] [Google Scholar]
- 9.Thom DH, van den Eeden SK, Brown JS. Evaluation of parturition and other reproductive variables as risk factors for urinary incontinence in later life. Obstet Gynecol. 1997;90:983. doi: 10.1016/s0029-7844(97)00537-1. [DOI] [PubMed] [Google Scholar]
- 10.Grodstein F, Fretts R, Lifford K, Resnick N, Curham G. Association of age, race, obstetric history with urinary symptoms among women in the Nurses' Health Study. Am J Obstet Gynecol. 2003;189:428. doi: 10.1067/s0002-9378(03)00361-2. [DOI] [PubMed] [Google Scholar]
- 11.Krieger N. Overcoming the absence of socioeconomic data in medical records validation and application of a census-based methodology. Am J Public Health. 1992;82:703. doi: 10.2105/ajph.82.5.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Paginini-Hill A, Ross RK. Reliability of recall of drug usage and other health-related information. Am J Epidemiol. 1982;116:114. doi: 10.1093/oxfordjournals.aje.a113386. [DOI] [PubMed] [Google Scholar]
- 13.Rortveit G, Hannestad YS, Daltveit AK, Hunskaar S. Age- and type-dependent effects of parity on urinary incontinence: the Norwegian EPINCONT study. Obstet Gynecol. 2001;98:1004. doi: 10.1016/s0029-7844(01)01566-6. [DOI] [PubMed] [Google Scholar]
- 14.Sandvik H, Seim A, Vanvik A, Hunskaar S. A severity index for epidemiological surveys of female urinary incontinence: comparison with 48-hour pad-weighing tests. Neurourol Urodyn. 2000;19:137. doi: 10.1002/(sici)1520-6777(2000)19:2<137::aid-nau4>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 15.Sandvik H, Hunskaar S, Vanvik A, Bratt H, Seim A, Hermstad R. Diagnostic classification of female urinary incontinence: an epidemiological survey corrected for validity. J Clin Epidemiol. 1995;48:339. doi: 10.1016/0895-4356(94)00147-i. [DOI] [PubMed] [Google Scholar]
- 16.Rohr G, Christensen K, Ulstrup K, Kragstrup J. Reproducibility and validity of simple questions to identify urinary incontinence in elderly women. Acta Obstet Gynecol Scand. 2004;83:969. doi: 10.1111/j.0001-6349.2004.00557.x. [DOI] [PubMed] [Google Scholar]
- 17.Greenland S. Modeling and variable selection in epidemiologic analysis. Am J Pub Health. 1989;79:340. doi: 10.2105/ajph.79.3.340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sze EH, Jones WP, Ferguson JL, Barker CD, Dolezal JM. Prevalence of urinary incontinence symptoms among black, white, and Hispanic women. Obstet Gynecol. 2002;99:572. doi: 10.1016/s0029-7844(01)01781-1. [DOI] [PubMed] [Google Scholar]
- 19.Knobel J. Stress incontinence in the black female. S Afr Med J. 1975;49:430. [PubMed] [Google Scholar]
- 20.Howard D, DeLancey JO, Tunn R, Ashton-Miller JA. Racial differences in the structure and function of the stress urinary continence mechanism. Obstet Gynecol. 2000;95:713. doi: 10.1016/s0029-7844(00)00786-9. [DOI] [PMC free article] [PubMed] [Google Scholar]