

Abstract
It has been hypothesized that neoplastic progression develops as a consequence of an acquired genetic instability and the subsequent evolution of clonal populations with accumulated genetic errors1. Accordingly, human cancers and some premalignant lesions contain multiple genetic abnormalities not present in the normal tissues from which the neoplasms arose2,3. Barrett oesophagus (BE) is a premalignant condition which predisposes to oesophageal adenocarcinoma (EA) that can be biopsied prospectively over time because endoscopic surveillance is recommended for early detection of cancer4,5. In addition, oesophagectomy specimens frequently contain the premalignant epithelium from which the cancer arose6. Neoplastic progression in BE is associated with alterations in TP53 (also known as p53) and CDKN2A (also known as p16) and non-random losses of heterozygosity7-11 (LOH). Aneuploid or increased 4N populations occur in more than 90-95% of EAs, arise in premalignant epithelium and predict progression10,12,13. We have previously shown in small numbers of patients that disruption of TP53 and CDKN2A typically occurs before aneuploidy and cancer10,11,14,15. Here, we determine the evolutionary relationships of non-random LOH, TP53 and CDKN2A mutations, CDKN2A CpG-island methylation and ploidy during neoplastic progression. Diploid cell progenitors with somatic genetic or epigenetic abnormalities in TP53 and CDKN2A were capable of clonal expansion, spreading to large regions of oesophageal mucosa. The subsequent evolution of neoplastic progeny frequently involved bifurcations and LOH at 5q, 13q and 18q that occurred in no obligate order relative to each other, DNA-content aneuploidy or cancer. Our results indicate that clonal evolution is more complex than predicted by linear models.
LOH at 5q, 9p, 13q, 17p and 18q was detected in 54%, 91%, 48%, 100% and 41%, respectively, of patients with aneuploid populations in premalignant epithelium and 66%, 75%, 66%, 100% and 57%, respectively, of patients with cancer. Mutations in exons 5-9 of TP53 were detected in 20 of 21 patients (95%) with 17p LOH, and CDKN2A mutations were present in 11 of 43 patients (26%) with 9p LOH. Patients (24) with 9p LOH were evaluated for both CDKN2A mutations by direct sequencing and for CpG-island methylation by methylation-specific PCR. Most patients (17/24, 71%) had either a mutation (5/24; 21%) or CpG-island methylation (12/24; 50%). CpG-island methylation was not detected in patients (5/5) who retained heterozygosity at 9p21. In addition, we found no evidence for homozygous CDKN2A deletions in our highly purified, flowsorted samples by microsatellite or sequencing analysis.
Premalignant diploid clones with somatic genetic abnormalities involving TP53, or both TP53 and CDKN2A, were frequently found in multiple biopsies extending over large areas (2-11 cm) of Barrett epithelium as early as 6 years before detection of cancer (Fig. 1). Identical TP53 and CDKN2A mutations were present at many levels of the Barrett segment, indicating early clonal expansion (Fig. 1a,b). The progenitor in patient 391 was a 2N (TP53 R306X, CDKN2A R58X) clone whose evolution included bifurcations, multiple aneuploidies and a neoplastic cell lineage that accumulated 13q and 18q LOH before culminating in cancer after 6 years (Fig. 1a). The 2.0N (TP53 R306X, CDKN2A R58X, 13q-), 3.0N (TP53 R306X, CDKN2A R58X, 13q-) and 3.6N (TP53 R306X, CDKN2A R58X, 13q-, 18q-) clones were all potential precursors of the cancer. The 3.0N clone, however, had no evidence of 18q LOH, was not detected before cancer and arose in a region spatially separated from the cancer, suggesting that it was not the precursor. We investigated all premalignant 2.0N clones detected from 1990 to 1996, and none showed 18q LOH. The 3.6N premalignant and 2.0N cancer clones, however, shared the same interstitial deletion of proximal 18q with retention of 18p and distal 18q, based on evaluation by 14 chromosome 18 STRs (data not shown). Thus, the 3.6N clone was the precursor to the cancer. The progenitor in patient 772 was a 2N (TP53 R248E) clone whose evolution was characterized by bifurcations, loss of alternate 5q alleles, multiple aneuploid populations and a neoplastic cell lineage that accumulated 9p and 5q LOH before developing 4N and aneuploid populations (Fig. 1c). An intermediate in the neoplastic lineages leading to 3.6N and 3.4N clones was not detected due to failure of the intermediate to persist or sampling limitations. This case also had a non-progressing 2N clone with loss of an alternate 9p allele not detected after 1991. In patient 779, the progenitor was a 2N (TP53 R306X, CDKN2A E88X) clone present in an endoscopic biopsy taken 3 years before detection of a cancer containing 3 aneuploid populations and a 13q LOH that evolved after cancer (Fig. 1d).
Fig. 1.
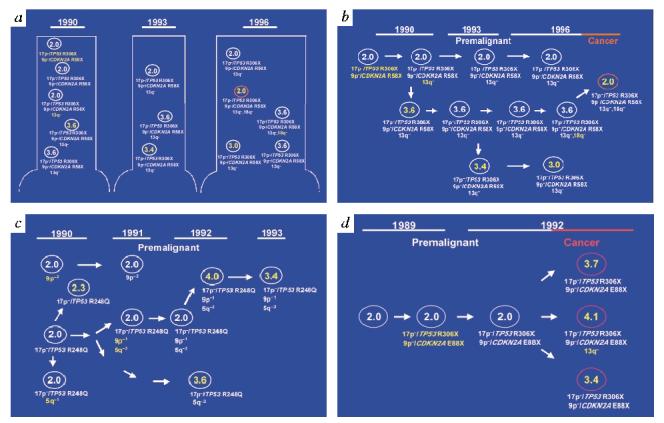
Clonal evolution in patients with BE in vivo. For each cell population, ploidy, LOH (5q-, 9p-, 13q-, 17p-, 18q-) and mutations are given below. LOH of alternate alleles is denoted (-1, -2). Cancer clones are red. Epithelial populations were purified by flow sorting. Ploidies were scored as different if DNA contents differed by 0.2N or more, as described30. The distribution of clones with somatic genetic abnormalities in premalignant epithelium at the baseline endoscopy and the evolution of neoplastic cell lineages are shown. a, In patient 391 (21 samples, 6 years), TP53 (CGA→TGA; R306X) and CDKN2A (CGA→TGA; R58X) mutations were found at all levels of an 8-cm Barrett segment. Endoscopic and surgical biopsies are from 1990-1996. b, Summary of cell lineages. c, In patient 772 (13 samples, three years), TP53 (CGG→CAG; R248E) mutation was found at all levels of an 11-cm Barrett segment. d, In patient 779 (17 samples, three years), TP53 (CGA→TGA; R306X) and CDKN2A (GAG→TAG; E88X) mutations were found in endoscopic and surgical biopsies from 1989 and 1992. Other somatic events may precede TP53 and CDKN2A abnormalities or lead linearly to cancer, but we found no evidence for them among the non-random LOHs detected in our allelotype of EA (ref. 8).
We used clonal ordering to further investigate relationships among genetic events in these neoplastic cell lineages (Table 1). LOH at 17p and 9p typically preceded aneuploidy (P<0.0001 and P<0.001, respectively) and cancer (P<0.0001 and P<0.001, respectively). There was no obligate order of 17p and 9p LOH during neoplastic progression (P=1.000). Mutations in TP53 and CDKN2A were also detected before aneuploidy (7/7 and 7/7 patients, respectively) and cancer (4/4 and 3/3 patients, respectively). Furthermore, patients (7/7) had CDKN2A CpG-island methylation in premalignant diploid as well as aneuploid populations. LOH at 17p was typically detected before and not after 5q (P<0.0001), 13q (P=0.002) and 18q LOH (P=0.004). Although 9p LOH was also typically detected before 5q (P=0.006) and 13q (P=0.004), it showed no obligate order relative to 18q LOH. LOH at 5q, 13q and 18q showed no obligate order relative to each other, although the number of cases in which these were evaluated was small.
| Table 1 • Clonal orders in BE | |||||
|---|---|---|---|---|---|
| Events | A before B patients (%) | A,B together patients (%) | A after B patients (%) | p | |
| A | B | ||||
| 17p LOH | aneuploidy | 19 (79) | 5 (21) | 0 (0) | <0.0001 |
| 9p | 7 (24) | 16 (55) | 6 (21) | 1.000 | |
| 5q | 19 (86) | 3 (14) | 0 (0) | <0.0001 | |
| 13q | 10 (63) | 6 (37) | 0 (0) | 0.002 | |
| 18q | 9 (56) | 7 (44) | 0 (0) | 0.004 | |
| cancer | 23 (96) | 1 (4) | 0 (0) | <0.0001 | |
| 9p LOH | aneuploidy | 20 (80) | 3 (12) | 2 (8) | <0.001 |
| 5q | 11 (73) | 3 (20) | 1 (7) | 0.006 | |
| 13q | 9 (60) | 6 (40) | 0 (0) | 0.004 | |
| 18q | 7 (50) | 3 (21) | 4 (29) | 0.549 | |
| cancer | 20 (87) | 0 (0) | 3 (13) | <0.001 | |
| 18q LOH | aneuploidy | 7 (64) | 0 (0) | 4 (36) | 0.549 |
| 5q | 7 (78) | 1 (11) | 1 (11) | 0.070 | |
| 13q | 4 (44) | 3 (33) | 2 (23) | 0.688 | |
| cancer | 9 (82) | 0 (0) | 2 (18) | 0.065 | |
| 5q LOH | aneuploidy | 4 (20) | 5 (25) | 11 (55) | 0.118 |
| 13q | 2 (25) | 3 (37.5) | 3 (37.5) | 1.000 | |
| cancer | 10 (53) | 3 (15) | 6 (32) | 0.454 | |
| 13q LOH | aneuploidy | 5 (36) | 3 (21) | 6 (43) | 1.000 |
| cancer | 8 (57) | 1 (7) | 5 (36) | 0.581 | |
Our observations of the evolution of neoplastic cell lineages in vivo confirm a pattern of events probably shared by most human neoplasms16-21. A progenitor clone undergoes expansion and, with the development of genetic instability, enters a phase of clonal evolution that begins in premalignant cells, proceeds over a period of years and continues after the emergence of cancer (Fig. 2). There have been reports that some cancers do not contain genetic abnormalities detectable in the premalignant epithelium from which the cancer arose22. Although some such cases may result from inadequate purification of neoplastic cells, others probably represent bifurcations leading to mosaics that include clonal populations not represented on the lineage that progresses to cancer. In addition, most human premalignant tissues do not appear to progress to cancer, even when highly prevalent somatic lesions are present23-26. For example, it is estimated that only 2.5 adenomatous polyps per 1,000 per year progress to colon cancer27. Flow cytometry has detected clonal heterogeneity in many neoplasias, and flow purification may be required to detect minority subclones with different LOHs developing before and after cancer28 (Fig. 1c). Our approach of flow sorting and clonal ordering to relate objective abnormalities (for example aneuploidy, LOH, TP53 and CDKN2A mutations) to each other, rather than histologic abnormalities, can be used to study the evolution of cell lineages in other human neoplasms.
Fig. 2.
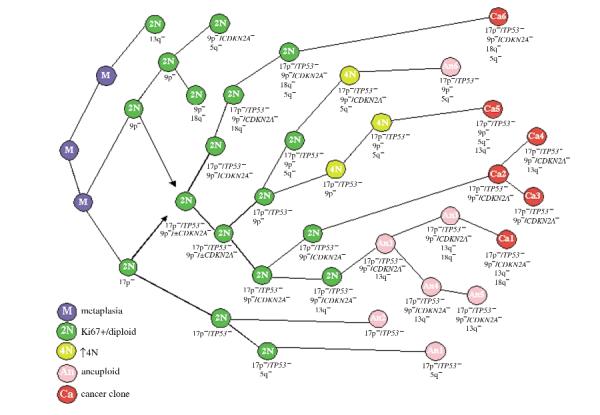
Multiple genetic routes to cancer in BE. Each clone represents a cell population detected in this study, but the figure is not intended to be comprehensive because the lack of obligate orders creates multiple genetic pathways to cancer, only some of which are represented. Although there are multiple pathways to cancer, some general patterns appear to be consistent among many patients. LOH events arise in diploid Ki67-positive populations (2N) in Barrett metaplasia (M). We detected 2N populations that developed LOH without lesions involving either TP53 or CDKN2A in 4 patients, but these clones failed to progress. LOH at either 17p (17p-) or 9p (9p-) can occur in diploid populations and can precede mutations in TP53 and CDKN2A. Although both 17p and 9p LOH develop as early events, they occur in no obligate order. 2N clones with somatic genetic abnormalities involving TP53 (17p-/TP53-) and CDKN2A (9p-/CDKN2A-; 9p-) frequently give rise to populations with elevated 4N fractions (4N) that can evolve aneuploid cell populations (An). Methylation of the CDKN2A CpG island was also detected in diploid cells before the development of aneuploidy. The 4N abnormality was not always detected, possibly from sampling limitations or failure of a genetically unstable intermediate to persist. In some cases, such as patient 391 (Fig. 1), changes in ploidy may result in a clone with a 2N or near-2N DNA content, yet with multiple genetic abnormalities. 5q, 13q and 18q LOH have no obligate order relative to aneuploidy, cancer or each other. During evolution, neoplastic cell lineages may bifurcate, giving rise to mosaics with the same TP53 and CDKN2A abnormalities but different ploidies and additional LOHs. Some clones in these mosaics develop into cancer (Ca), whereas others either are delayed in their progression or represent dead ends. Subsequently, multiple malignant clones (Ca) with different ploidies and additional LOHs evolve as the cancer progresses.
Methods
Patients and tissues. We evaluated flow-sorted samples (n=266) from multiple premalignant and/or cancer biopsies (n=189) from 49 patients who had specialized columnar epithelium in oesophageal biopsies, aneuploidy and a maximum diagnosis of high-grade dysplasia or cancer. None received radiation or chemotherapy before tissue acquisition. The Barrett’s Esophagus Study was approved by the Human Subjects Review Boards at the University of Washington and the Fred Hutchinson Cancer Research Center. Patients were counselled concerning risks and benefits of endoscopic surveillance for BE and informed of potential alternatives, including surgery for high-grade dysplasia. Premalignant biopsies were available from 31 patients, 25 of whom had progressed to cancer. Cancer biopsies were available from 32 patients, including 14 patients who had both premalignant and cancer biopsies available. Normal gastric tissue served as a constitutive control for each patient. This study included 10, 15 and 3 patients for whom the orders of 17p, 9p and 18q LOH, respectively, with cancer or aneuploidy were previously reported11,14,15,29.
Flow-cytometric sorting. DNA content and multiparameter Ki67/DNA-content flow sorting were performed as described10,13. DNA content flow-cytometry for 2N, 4N and aneuploid sorting was performed as follows. Biopsies were minced with scalpel blades in a petri dish (35×100 mm) in NST buffer (146 mM NaCl, 10 mM Tris-HCl, pH 7.5, 1 mM CaCl2, 0.5 mM MgSO4, 21 mM MgCl2, 0.05% bovine serum albumin, 0.2% Nonidet P40 (Sigma)) with 4,6-diamindino-2-phenylindole (DAPI; 10 μg/ml; Boehringer). To disaggregate and enucleate the cells, the suspension was forced through a 1-cc syringe with a 25-gauge needle 7-10 times. After mincing, samples were always kept on ice. Ki67/DNA-content multiparameter flow-cytometric cell sorting was used to purify populations of proliferating diploid epithelial cells. Ki67-R-phycoerythrin is a directly conjugated proliferation-associated monoclonal antibody that identifies cells in late G1, S, G2 and mitosis, but not G0. Biopsies were minced and sheared in NST buffer. Nuclei for Ki67/DNA-content sorting were centrifuged at 2,000 r.p.m. for 10 min at 4 °C, resuspended in NST buffer with 10% normal goat serum (Caltag), divided and incubated with Ki67-RPE (3.75 μg/ml) and IgG1-RPE isotype antibodies (Dako), respectively. After incubation, samples were centrifuged as above and resuspended in NST buffer with 10% NGS and DAPI (10 μg/ml). To disaggregate the nuclei immediately before analysis, the suspension was forced through a 1-cc syringe with 25-gauge needle 7 times and then filtered through a 40-μm mesh filter. All samples were sorted using a Coulter Elite ESP cell sorter.
Microsatellite analysis. LOH was assessed with the following polymorphic markers: D5S107, D5S299, D5S346, D9S942, D9S43, BRCA2, D13S314, TP53, D17S786, D17S261, D18S474, D18S34, D18S46 and D18S53. Retention of heterozygosity was assessed with D9S55, D9S162, IFNA1 and D9S156 in patients heterozygous for 9p21. Data were reviewed in a coded fashion.
DNA sequence analysis. Aneuploid populations from 21 of 48 patients with 17p LOH and from all patients with 9p LOH were screened for TP53 and CDKN2A mutations, respectively, by dye-terminator fluorescent sequencing7,10,11.
Methylation analysis. DNA samples were treated with bisulfite as described9. Briefly, each DNA sample (6 ng, ∼800 cells) was denatured in freshly prepared NaOH (0.3 M, 20 min at 42 °C), treated with sodium bisulfite (3.8 M, pH 5.0)/hydroquinone (1.0 mM; 6-8 h at 55 °C) and desulfonated with NaOH (0.3 M, 20 min at 37 °C). Bisulfite-treated samples were subsequently whole-genome amplified by primer-extension preamplification (PEP) as described8,9. Aliquots of PEP reactions were used for methylation-specific PCR (MSP) analysis using primer pairs p16-M and p16-U as described9.
Acknowledgements
We thank D. Levine, R. Haggitt and P. Blount for contributions to the Seattle Barrett’s Esophagus Study, G. Longton for statistical analysis and L. Hartwell, C. Kemp, M. Groudine and S. Friend for reviewing this manuscript.
Footnotes
Supported by NIH Grants RO1CA61202, DK07742-03 (T.G.P.), ACS Grant RPG-87-0060120CCE and Poncin Scholarship Fund (D.J.W.).
References
- 1.Nowell PC. The clonal evolution of tumor cell populations. Science. 1976;194:23–28. doi: 10.1126/science.959840. [DOI] [PubMed] [Google Scholar]
- 2.Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–767. doi: 10.1016/0092-8674(90)90186-i. [DOI] [PubMed] [Google Scholar]
- 3.Boland CR, Sato J, Appelman HD, Besalier RS, Feinberg AP. Microallelotyping defines the sequence and tempo of allelic losses at tumor suppressor gene loci during colorectal cancer progression. Nature Med. 1995;1:902–909. doi: 10.1038/nm0995-902. [DOI] [PubMed] [Google Scholar]
- 4.Spechler SJ. Endoscopic surveillance for patients with Barrett esophagus: does the cancer risk justify the practice. Ann. Intern. Med. 1987;106:902–904. doi: 10.7326/0003-4819-106-6-902. [DOI] [PubMed] [Google Scholar]
- 5.Levine DS, et al. An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology. 1993;105:40–50. doi: 10.1016/0016-5085(93)90008-z. [DOI] [PubMed] [Google Scholar]
- 6.Rabinovitch PS, Reid BJ, Haggitt RC, Norwood TH, Rubin CE. Progression to cancer in Barrett’s esophagus is associated with genomic instability. Lab. Invest. 1989;60:65–71. [PubMed] [Google Scholar]
- 7.Neshat K, et al. p53 mutations in Barrett’s adenocarcinoma and high-grade dysplasia. Gastroenterology. 1994;106:1589–1595. doi: 10.1016/0016-5085(94)90415-4. [DOI] [PubMed] [Google Scholar]
- 8.Barrett MT, Galipeau PC, Sanchez CA, Emond MJ, Reid BJ. Determination of the frequency of loss of heterozygosity in esophageal adenocarcinoma by cell sorting, whole genome amplification and microsatellite polymorphisms. Oncogene. 1996;12:1873–1878. [PubMed] [Google Scholar]
- 9.Wong DJ, Barrett MT, Stoger R, Emond MJ, Reid BJ. p16INK4a promoter is hypermethylated at a high frequency in esophageal adenocarcinomas. Cancer Res. 1997;57:2619–2622. [PubMed] [Google Scholar]
- 10.Galipeau PC, et al. 17p (p53) allelic losses, 4N (G2/tetraploid) populations, and progression to aneuploidy in Barrett’s esophagus. Proc. Natl Acad. Sci. USA. 1996;93:7081–7084. doi: 10.1073/pnas.93.14.7081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barrett MT, et al. Allelic loss of 9p21 and mutation of the CDKN2/p16 gene develop as early lesions during neoplastic progression in Barrett’s esophagus. Oncogene. 1996;13:1867–1873. [PubMed] [Google Scholar]
- 12.Reid BJ, Haggitt RC, Rubin CE, Rabinovitch PS. Barrett’s esophagus. Gastroenterology. 1987;93:1–11. [PubMed] [Google Scholar]
- 13.Reid BJ, et al. Flow-cytometric and histological progression to malignancy in Barrett’s esophagus: prospective endoscopic surveillance of a cohort. Gastroenterology. 1992;102:1212–1219. [PubMed] [Google Scholar]
- 14.Blount PL, et al. Clonal ordering of 17p and 5q allelic losses in Barrett dysplasia and adenocarcinoma. Proc. Natl Acad. Sci. USA. 1993;90:3221–3225. doi: 10.1073/pnas.90.8.3221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Blount PL, et al. 17 p allelic losses in diploid cells of patients with Barrett’s esophagus who develop aneuploidy. Cancer Res. 1994;54:2292–2295. [PubMed] [Google Scholar]
- 16.Mao L, et al. Clonal genetic alterations in the lungs of current and former smokers. J. Natl Cancer Inst. 1997;89:857–862. doi: 10.1093/jnci/89.12.857. [DOI] [PubMed] [Google Scholar]
- 17.Bedi GC, Westra WH, Gabrielson E, Koch W, Sidransky D. Multiple head and neck tumors: evidence for a common clonal origin. Cancer Res. 1996;56:2484–2487. [PubMed] [Google Scholar]
- 18.Califano J, et al. Genetic progression model for head and neck cancer: implications for field cancerization. Cancer Res. 1996;56:2488–2492. [PubMed] [Google Scholar]
- 19.Sidransky D, et al. Clonal expansion of p53 mutant cells is associated with brain tumour progression. Nature. 1992;355:846–847. doi: 10.1038/355846a0. [DOI] [PubMed] [Google Scholar]
- 20.Gazdar AF, et al. Molecular genetic changes found in human lung cancer and its precursor lesions. Cold Spring Harb. Symp. Quant. Biol. 1994;59:565–572. doi: 10.1101/sqb.1994.059.01.063. [DOI] [PubMed] [Google Scholar]
- 21.Kuukasjarvi T, et al. Genetic heterogeneity and clonal evolution underlying development of asynchronous metastasis in human breast cancer. Cancer Res. 1997;57:1597–1604. [PubMed] [Google Scholar]
- 22.Wu T, et al. Genetic alterations in Barrett esophagus and adenocarcinomas of the esophagus and esophagogastric junction region. Am. J. Pathol. 1998;153:287–294. doi: 10.1016/S0002-9440(10)65570-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.van der Burgh A, Dees J, Hop WCJ, van Blankenstein M. Oesophageal cancer is an uncommon cause of death in patients with Barrett’s oesophagus. Gut. 1996;39:5–8. doi: 10.1136/gut.39.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mao L, et al. Clonal genetic alterations in the lungs of current and former smokers. J. Natl Cancer Inst. 1997;89:857–862. doi: 10.1093/jnci/89.12.857. [DOI] [PubMed] [Google Scholar]
- 25.Correa P, et al. Gastric precancerous process in a high risk population: cohort follow-up. Cancer Res. 1990;50:4737–4740. [PubMed] [Google Scholar]
- 26.Rozen P, Baratz M, Fefer F, Gilat T. Low incidence of significant dysplasia in a successful endoscopic surveillance program of patients with ulcerative colitis. Gastroenterology. 1995;108:1361–1370. doi: 10.1016/0016-5085(95)90683-5. [DOI] [PubMed] [Google Scholar]
- 27.Eide TJ. Risk of colorectal cancer in adenoma-bearing individuals within a defined population. Int. J. Cancer. 1985;38:173–176. doi: 10.1002/ijc.2910380205. [DOI] [PubMed] [Google Scholar]
- 28.Petersen SE, Lorentzen M, Bichel P. A mosaic subpopulation structure of human colorectal carcinomas demonstrated by flow cytometry. Flow Cytometry. 1980;IV:412–416. [Google Scholar]
- 29.Barrett MT, Schutte M, Kern SE, Reid BJ. Allelic loss and mutational analysis of the DPC4 gene in esophageal adenocarcinoma. Cancer Res. 1996;56:4351–4353. [PubMed] [Google Scholar]
- 30.Levine DS, et al. Distribution of aneuploid cell populations in ulcerative colitis with dysplasia or cancer. Gastroenterology. 1991;101:1198–1210. doi: 10.1016/0016-5085(91)90068-v. [DOI] [PubMed] [Google Scholar]