

Abstract
β-adrenoceptor-mediated relaxation was investigated in ring preparations of rat isolated thoracic aorta. Rings were pre-constricted with a sub-maximal concentration of noradrenaline (1 μM) and relaxant responses to cumulative concentrations of β-adrenoceptor agonists obtained.
The concentration-response curve (CRC) to isoprenaline was shifted to the right by propranolol (0.3 μM) with a steepening of the slope. Estimation of the magnitude of the shift from EC50 values gave a pA2 of 7.6. Selective β1- and β2-adrenoceptor antagonists, CGP 20712A (0.1 μM) and ICI 118551 (0.1 μM), respectively, produced 4 and 14 fold shifts of the isoprenaline CRC.
Atypical β-adrenoceptor agonists also produced concentration-dependent relaxation of aortic rings. The order of potency of the β-adrenoceptor agonists was (−log EC50): isoprenaline (6.25)>cyanopindolol (5.59)>isoprenaline+propranolol (5.11)>CGP 12177A (4.40)>ZD 2079 (4.24)>ZM 215001 (4.07)>BRL 37344 (3.89). Relaxation to CGP 12177A and ZM 215001 was unaffected by propranolol (0.3 μM).
SR 59230A (⩽1 μM) and cyanopindolol (1 μM), β3-adrenoceptor antagonists, had no effect on the isoprenaline (in the presence of propranolol) or CGP 12177A CRCs. Bupranolol and CGP 20712A, at μM concentrations (β4-adrenceptor antagonists), inhibited responses to isoprenaline (in the presence of propranolol) and CGP 12177A.
In conclusion, atypical β-adrenoceptors co-exist with β1- and β2-adrenoceptors in rat aorta. Although non-conventional partial agonists and selective β3-adrenoceptor agonist cause relaxation, the vascular atypical β-adrenoceptor does not appear to correspond to the β3-adrenoceptor. There are, however, similarities with the putative β4-adrenoceptor.
Keywords: Atypical β-adrenoceptors, β3-adrenoceptors, β4-adrenoceptors, β1-adrenoceptors, β2-adrenoceptors, vascular smooth muscle, rat aorta
Introduction
β-adrenoceptor-mediated vasodilation is thought to play an important physiological role in the regulation of vascular tone. Vascular β-adrenoceptors were originally classified as β2- (Lands et al., 1967) and this appears to be the predominant subtype in most vascular smooth muscles, although β1-adrenoceptors may also contribute to vasodilation (O'Donnell & Wanstall, 1985). In a few vessels β1-adrenoceptors appear to predominate e.g. coronary arteries (Macdonald et al., 1987; O'Donnell & Wanstall, 1985) and cerebral arteries (Edvinsson & Owman, 1974). More recently, a number of reports suggest the presence of atypical β-adrenoceptors, not conforming to the β1-/β2- subclassification, in blood vessels (Oriowo, 1994; 1995; Sooch & Marshall, 1996; Tamaoki et al., 1998; MacDonald et al., 1999).
Atypical β-adrenoceptors include the β3-adrenoceptor, first identified functionally in adipose tissue and the gastrointestinal tract (reviewed by Arch & Kaumann, 1993). β3-adrenoceptors are characterized by (i) low affinity of classical β-adrenoceptor antagonists, such as propranolol, (ii) activation by selective β3-adrenoceptor agonists, such as BRL 37344 (Arch, 1989; Arch & Kaumann, 1993), (iii) activation by ‘non-conventional partial agonists' (β1-/β2-adrenoceptor antagonists with agonist activity at higher concentrations (Kaumann, 1989)), such as CGP 12177A (Mohell & Dicker, 1989) and (iv) blockade with selective β3-adrenoceptor antagonists such as SR 59230A (Manara et al., 1996). Further atypical β-adrenoceptor subtypes may exist: e.g. there is evidence for a putative β4-adrenoceptor in cardiac and adipose tissue which shares properties (i) and (iii) above but not (ii) and (iv) (Malinowska & Schlicker, 1996; Kaumann & Molenaar, 1996; Galitzky et al., 1997).
In rat isolated common carotid artery responses to isoprenaline were antagonized by propranolol in a non-competitive manner suggesting both high affinity (β1-/β2-) and low affinity (atypical β-) β-adrenoceptors (Oriowo, 1994). BRL 37344 and CGP 12177A also produced vasorelaxation and this relaxation was not antagonized by propranolol (Oriowo, 1994). Similar findings of a propranolol-resistant component to isoprenaline-induced relaxation and relaxant responses to atypical β-adrenoceptor agonists have been reported in rat mesenteric artery (Sooch & Marshall, 1995) and in rat aorta and pulmonary artery (Sooch & Marshall, 1996). The vascular atypical β-adrenoceptors may be different from the well-characterized atypical β-adrenoceptors of gastro-intestinal smooth muscle (β3-adrenoceptors) (McLaughlin & MacDonald, 1990; 1991) however, since atypical β-adrenoceptor-mediated relaxations in rat thoracic aorta and carotid artery were not desensitized by BRL 37344 or antagonized by cyanopindolol in contrast to relaxations of colon and fundus strips (Oriowo, 1995).
The present study was carried out to further characterize the β-adrenoceptor subtypes mediating relaxation in rat aorta using selective agonists and antagonists. Preliminary accounts of some of this work have been presented previously (Brawley et al., 1997; 1998).
Methods
Tissue preparation
Male Wistar rats (150–300 g), were stunned and killed by cervical dislocation followed by exsanguination. The thoracic aorta was isolated, removed carefully to prevent endothelium damage and cleared of fat and connective tissue. The thoracic aorta was cut into 3 mm ring segments which were mounted on stainless steel wires in 20 ml organ baths containing Krebs' medium with the following composition (mM): NaCl, 119; KC1, 4.7; CaCl2, 2.5; MgSO4, 1.2; NaHCO3, 25; KH2PO4, 1.2; D-glucose, 11.1. The Krebs' medium also contained ethylene diamine tetra-acetic acid (EDTA: 30 μM) and ascorbic acid (30 μM) to prevent oxidation of catecholamines. The medium was maintained at 37°C and gassed continuously with 95% O2 and 5% CO2. Each tissue was placed under an initial resting tension of 1 g and allowed to equilibrate for 60 min prior to the execution of experimental protocols. Muscle tension was recorded with Grass transducers and displayed on a Goerz Servogor 400 oscillograph.
Concentration-response curves (CRCs)
After the equilibration period artery rings were constricted with a sub-maximal concentration of noradrenaline (1 μM) and the contraction allowed to stabilize over a period of 10 min. The integrity of the endothelium was tested with acetylcholine (1 and 10 μM). Preparations failing to produce greater than 50% relaxation with acetylcholine (10 μM) were discarded. After washout, some tissues were incubated with the appropriate antagonist for 30 min with control tissues receiving no treatment. The rings were then contracted again with noradrenaline (1 μM) and cumulative concentration-response curves to agonists were conducted. After washing, tissues were contracted with noradrenaline for a third time before challenging with acetylcholine (1 and 10 μM) to monitor endothelium function.
Drugs used
The following were dissolved in distilled water, with exception of SR 59230A which was dissolved in 20% ethanediol: (±) noradrenaline bitartrate (Sigma), acetylcholine chloride (Sigma), (−)-isoprenaline bitartrate (Sigma), (±)-propranolol hydrochloride (Sigma), CGP 12177A hydrochloride ((±)-4-(3-tbutylamino-2-hydroxypropoxy)-benzimidazol-2-one hydrochloride, gift from Novartis Pharma), BRL 37344 ((R*,R*)-(±)-4-[2-[(3-chlorophenyl)-2-hydroxyethyl) amino]propyl]phenoxyacetic acid (Tocris Cookson), (±)-cyanopindolol hemifumarate (Tocris Cookson), ZD 2079 ((R)-N-(2-[4-(carboxymethyl)phenoxy]ethyl) - N - (β-hydroxyphenethyl)ammonium chloride, gift from Zeneca), ZM 215001 ((S)-4-(2–hydroxy-3 -phenoxypropylaminoethoxy)-N-(2-methoxyethyl)phenoxyacetic acid, gift from Zeneca), CGP 20712A (2-hydroxy-5(2-((2-hydroxy-3-4((1-methyl-4-trifluoromethyl)1H-imidazole - 2 - yl) - phenoxy)propyl)amino)ethoxy) - benzamide monomethane sulphonate, gift from Novartis Pharma AG), (−)-bupranolol hydrochloride (gift from Schwartz Pharma), SR 59230A (3-(2-ethylphenoxy)-1-[(1S)-1,2,3,4-tetrahydronaphth-1-ylamino]-2S-2-propanol oxalate, gift from Sanofi, Italy), and ICI 118551 ((±)-1-[2,3-(dihydro-7-methyl-1H-inden-4-yl)oxy]-3-[(1-methylethyl)amino]-2-butanol, Tocris Cookson).
Calculations and statistical analysis
Responses to agonists were calculated as % inhibition of the noradrenaline-induced contraction and expressed as mean±s.e.mean. Mean concentration response curves (CRCs) to agonists were analysed by fitting to a four parameter logistic equation using non-linear regression (Graph Pad Prism). Maximum responses and −log EC50 values were obtained where EC50 is the concentration (M) of agonist that produces 50% of its maximum response. Agonist concentration ratios (CR) were determined from EC50 values and estimates of pA2 obtained from the equation, pA2=log(agonist CR - 1)−log[antagonist].
Statistical analyses were performed using Student's or paired t-tests to compare two groups and one-way analysis of variance followed by the Bonferroni multiple comparison post test for comparison of three or more groups.
Results
Noradrenaline contraction
Noradrenaline (1 nM–300 μM) produced a concentration-dependent contraction of rat thoracic aortic rings (−log EC50=5.96±0.02, n=5). A sub-maximal concentration, 1 μM, approximately equivalent to the EC50 was chosen for subsequent experiments. This concentration of noradrenaline produced sustained constriction against which agonist-induced relaxations could be suitably obtained.
Acetylcholine relaxation
Noradrenaline-constricted endothelium-intact rings relaxed to acetylcholine (1 and 10 μM) with 10 μM producing a significantly greater relaxation than 1 μM (% relaxation: 1 μM, 56±6; 10 μM, 76±7, P<0.05). Endothelium-intact tissues failing to produce over 50% relaxation to acetylcholine (10 μM) were not included.
Isoprenaline and propranolol
Isoprenaline produced a concentration-dependent relaxation of noradrenaline preconstricted aortic rings (−log EC50=6.25±0.08; % maximum relaxation, 101±3, n=19) (Figure 1a). Propranolol (0.3 μM) shifted the isoprenaline CRC to the right with no reduction in the maximum response (−log EC50=5.11±0.03; % maximum relaxation, 96±2, n=37) (Figure 1a). The shift was greater at the lower concentrations of isoprenaline, resulting in a steepening of the slope of the isoprenaline CRC (Hill slopes: control, 0.46±0.02; propranolol, 0.82±0.03, P<0.001). Estimation of the magnitude of the shift from the EC50 values gave a 13.8 fold shift, which corresponds to a pA2 value of 7.61. Propranolol treatment had no effect on subsequent noradrenaline pre-contraction or acetylcholine-induced relaxation (results not shown).
Figure 1.
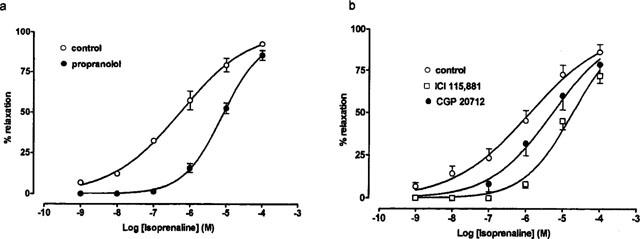
The effect of β-adrenoceptor antagonists on relaxation induced by isoprenaline in rat thoracic aortic rings preconstricted with noradrenaline (1 μM). Results are expressed as percentage relaxation of tone induced by noradrenaline. Values are mean±s.e.mean of n observations (a) Effect of propranolol (0.3 μM) (n=19–37). (b) Effect of CGP 20712A (0.1 μM) and ICI 118551 (0.1 μM) (n=6).
Isoprenaline and selective β1-/β2-antagonists
The β1- and β2-adrenoceptor selective antagonists, CGP 20712A (0.1 μM) and ICI 118551 (0.1 μM) respectively, shifted the isoprenaline CRC to the right (−log EC50 values: control, 5.88±0.06, n=6; ICI 118551, 4.73±0.08, P<0.001, n=6; CGP 20712A, 5.27±0.08, P<0.001, n=6) (Figure 1b). ICI 118551, but not CGP 20712A, also produced a significant steepening of the isoprenaline CRC (Hill slopes: control, 0.42±0.02; ICI 118551, 0.66±0.08, P<0.05; CGP 20712A, 0.52±0.05, P>0.05). ICI 118551 produced a greater shift of the isoprenaline CRC than CGP 20712A (shifts estimated from EC50 values: ICI 118551, 14 fold; CGP 20712A, 4 fold). Pre-incubation with CGP 20712A or ICI 118551 had no effect on the size of subsequent noradrenaline pre-constriction or acetylcholine-induced relaxation (results not shown).
Atypical β-adrenoceptor agonists
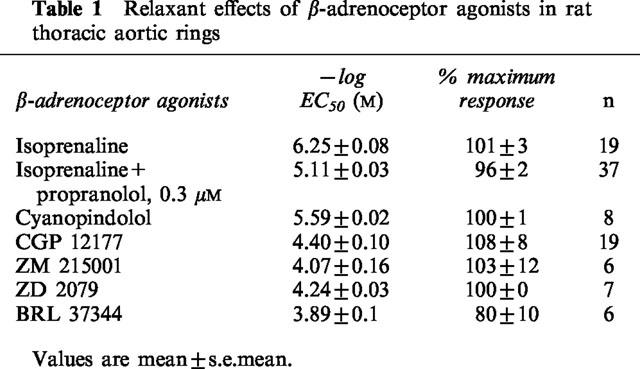
CGP 12177A, cyanopindolol, BRL 37344, ZD 2079 and ZM 215001 also produced concentration-dependent relaxations of pre-constricted rat aortic rings with an order of potency: isoprenaline≈thinsp;4 cyanopindolol > isoprenaline + propranolol, 0.3 μM>CGP 12177A>ZD 2079>ZM 215001>BRL 37344 (Figure 2a, Table 1). Propranolol (0.3 μM) had no effect on CGP 12177A- or ZM 215001-induced relaxations (Figure 2b,c).
Figure 2.
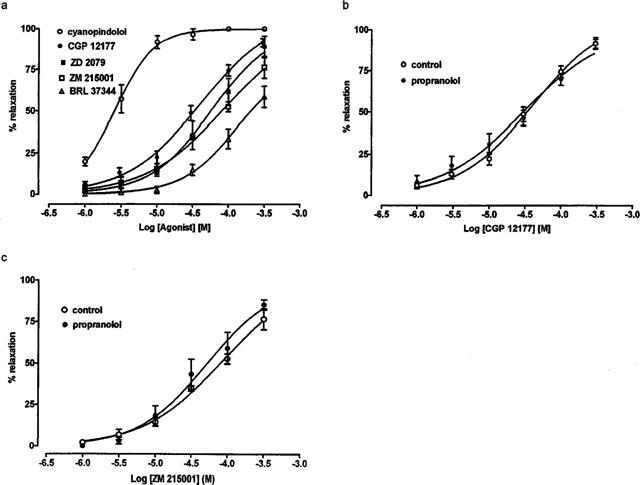
The effect of atypical β-adrenoceptor agonists in rat thoracic aorta. Results are expressed as percentage relaxation of tone induced by noradrenaline. Values are mean±s.e.mean of n observations. (a) Effects of cyanopindolol, CGP 12177A, ZD 2079, ZM 215001 and BRL 37344 (n=6–19). (b) Effect of propranolol (0.3 μM) on relaxation induced by CGP 12177A (n=8–19). (c) Effect of propranolol (0.3 μM) on relaxation induced by ZM 215001 (n=4–6).
Table 1.
Relaxant effects of β-adrenoceptor agonists in rat thoracic aortic rings
SR 59230A
In the presence of propranolol (0.3 μM), isoprenaline-induced relaxations were unaltered following pretreatment with the selective β3-adrenoceptor antagonist, SR 59230A (10 nM–1 μM) (Figure 3a). Similarly, SR 59230 (10 nM–1 μM) failed to displace the CGP 12177A CRC (Figure 3b). SR 59230A did not affect acetylcholine relaxation or noradrenaline constriction (results not shown).
Figure 3.
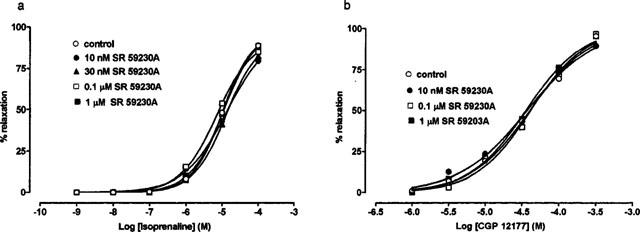
The effect of SR 59230A (10 nM–1 μM) on β-adrenoceptor agonist-induced relaxation in rat thoracic aorta. Results are expressed as percentage relaxation of tone induced by noradrenaline (1 μM). Values are mean±s.e.mean of n observations. (a) Effect of SR 59230A (10 nM–1 μM) on relaxation induced by isoprenaline (in the presence of 0.3 μM propranolol) (n=5–19). (b) Effect of SR 59230A (10 nM–1 μM) on relaxation induced by CGP 12177A (n=4–5).
Cyanopindolol
Cyanopindolol (1 μM) reduced responses to isoprenaline with an apparent reduction in slope of the CRC, although the difference in Hill slopes was not significantly different (Hill slopes: control, 0.42±0.05, n=8, cyanopindolol, 0.32±0.06, n=8, P>0.05) (Figure 4a). The shift of the isoprenaline CRC was no greater than seen before with propranolol and a combination of cyanopindolol and propranolol produced no further antagonism than either antagonist alone (−log EC50s: control; 5.66±0.21; cyanopindolol, 4.78±0.76; cyanopindolol+propranolol, 4.62±0.08, n=8–11). Pretreatment with cyanopindolol (1 μM) produced significant reductions in the noradrenaline-induced constriction (constriction to noradrenaline, g tension: control, 0.70±0.07, n=8, cyanopindolol, 0.45±0.06, n=8, P<0.05). Cyanopindolol had no effect on acetylcholine-induced relaxation (results not shown). Cyanopindolol (1 μM) produced no significant reduction in the response to CGP12177A (−log EC50s: control, 4.49±0.03; cyanopindolol, 4.28±0.04, n=9–19, P>0.05) (Figure 4b).
Figure 4.
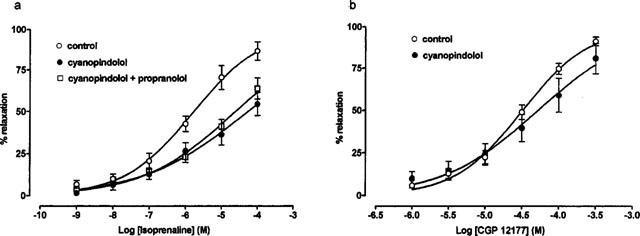
The effect of cyanopindolol (1 μM) and propranolol (0.3 μM) on β-adrenoceptor agonist-induced relaxation in rat thoracic aortic rings preconstricted with noradrenaline (1 μM). Results are expressed as percentage relaxation of tone induced by noradrenaline. Values are mean±s.e.mean of n observations. (a) Effect of cyanopindolol (1 μM) and propranolol (0.3 μM) on relaxation induced by isoprenaline (n=8–11). (b) Effect of cyanopindolol (1 μM) on relaxation induced by CGP 12177A (n=9–19).
Bupranolol
In the presence of propranolol (0.3 μM), bupranolol shifted the isoprenaline CRC to the right with a lowering of the maximum response (Figure 5a). It was not possible to obtain −log EC50 values in the presence of the higher concentrations of bupranolol.
Figure 5.
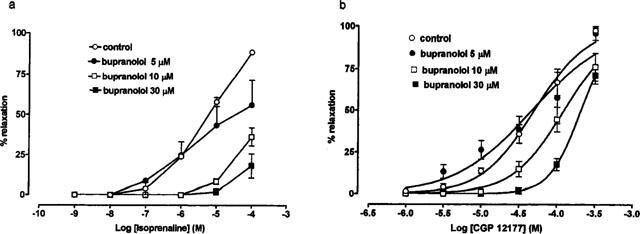
The effect of bupranolol (5–30 μM) on β-adrenoceptor agonist-induced relaxation in rat thoracic aortic rings preconstricted with noradrenaline (1 μM). Results are expressed as percentage relaxation of tone induced by noradrenaline. Values are mean±s.e.mean of n observations. (a) Effect of bupranolol (5–30 μM) on relaxation induced by isoprenaline (in the presence of 0.3 μM propranolol) (n=4–9). (b) Effect of bupranolol (5–30 μM) on relaxation induced by CGP 12177A (n=3–8).
Bupranolol pretreatment shifted the CGP 12177 CRC rightward with no depression in the maximum response (−log EC50s: control, 4.31±0.04, n=8; bupranolol 5 μM, 4.34±0.11, n=3, P>0.05; bupranolol 10 μM, 3.91±0.02, n=7, P<0.001; bupranolol 30 μM, 3.68±0.01, n=6, P<0.001 (Figure 5b). Bupranolol (10 and 30 μM) produced 2.5 and 4.2 fold shifts, respectively which correspond to pA2 values of 5.2 and 5.0 respectively.
Bupranolol (⩽30 μM) had no significant effect on noradrenaline contractions or acetylcholine-induced relaxations (results not shown).
CGP 20712A
In the presence of propranolol (1 μM), CGP 20712A (1 and 10 μM) shifted the isoprenaline CRC 4.8 and 5.8 fold to the right with no significant reduction in maximum response (−log EC50s: control, 5.72±0.15, n=4; CGP 20712A, 1 μM, 5.04±0.06, n=4, P<0.001; CGP 20712A, 10 μM, 4.96±0.01, n=4, P<0.001) (Figure 6a). A further increase in concentration of CGP 20712A to 100 μM produced little or no further shift of the isoprenaline CRC (−log EC50: 4.83±0.01, n=5, P<0.001). A pA2 estimated from the shift produced by 1 μM gave a value of 6.6.
Figure 6.
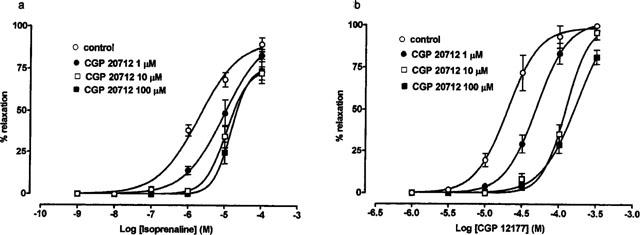
The effect of CGP 20712A (1–100 μM) on β-adrenoceptor agonist-induced relaxation in rat thoracic aortic rings preconstricted with noradrenaline (1 μM). Results are expressed as percentage relaxation of tone induced by noradrenaline. Values are mean±s.e.mean of n observations. (a) Effect of CGP 20712A (1–100 μM) on relaxation induced by isoprenaline (in the presence of 1 μM propranolol) (n=4–5). (b) Effect of CGP 20712A (1–100 μM) on relaxation induced by CGP 12177A (n=4).
CGP 20712A, 1 and 10 μM, produced 2.5 fold and 6.2 fold rightward shifts respectively of the CGP 12177A CRC (−log EC50s: control: 4.70±0.01, n=4; CGP 20712A, 1 μM, 4.31±0.01, P<0.001; CGP 20712A, 10 μM, 3.91±0.02, n=4, P<0.001) (Figure 6b). Increasing the concentration of CGP 20712A to 100 μM produced little further shift in the CGP 12177A CRC (−log EC50: 3.77±0.01, n=4, P<0.001). A pA2 estimated from the shift produced by 1 μM gave a value of 6.2.
Pretreatment with CGP 20712A (⩽100 μM) had no significant effect on acetylcholine-induced relaxation or noradrenaline preconstriction (not shown).
Discussion
Isoprenaline produced concentration-dependent relaxation of pre-constricted rat thoracic aorta. The non-selective β1- and β2-adrenoceptor antagonist, propranolol, shifted the isoprenaline CRC to the right supporting the presence of β1-/β2-adrenoceptors in this preparation. However, the shift produced by isoprenaline (estimated pA2 of 7.6) was considerably less than would be predicted for on action of propranolol at classical β-adrenoceptors. With a pA2 of 8.2–8.8 at classical β-adrenoceptors (Wilson et al., 1984), propranolol would have been expected to shift the isoprenaline curve by 50–200 fold as opposed to the 14 fold shift achieved. In addition, the shift was not parallel, with a greater shift at lower concentrations of isoprenaline, suggesting propranolol-sensitive (low concentrations of isoprenaline) and insensitive (high concentrations of isoprenaline) components of the isoprenaline CRC. These results suggest that atypical β-adrenoceptors, resistant to propranolol, co-exist with classical β-adrenoceptors in this preparation. Gray & Marshall (1992) reported a similar low affinity estimate for propranolol in rat aorta (pKb 7.5). Sooch & Marshall (1997) also found evidence for propranolol-sensitive and insensitive components of the response to isoprenaline in rat aorta. Similar findings of a propranolol-resistant component in the response to isoprenaline have been reported in rat carotid artery (Oriowo, 1994), rat mesenteric artery (Sooch & Marshall, 1995) and rat pulmonary artery (Sooch & Marshall, 1996).
The β1- and β2- selective antagonists, CGP 20712A and ICI 118551 also shifted the isoprenaline CRC rightward. ICI 118551 produced a larger shift and a significant steepening of the isoprenaline CRC, suggesting that β2-adrenoceptors play a greater role than β1-adrenoceptors in relaxation. These findings agree with those of O'Donnell & Wanstall (1984) who reported that rat aorta contains both β1- and β2-adrenoceptors, with β2-adrenoceptors being the predominant subtype.
Relaxation was also produced by the atypical β-adrenoceptor agonists, CGP 12177A, cyanopindolol, BRL 37344, ZM 215001 and ZD 2079. CGP 12177A and cyanopindolol are described as non-conventional partial agonists (Kaumann, 1989): they are β1- and β2-adrenoceptor antagonists (Staehelin et al., 1983; Engel et al., 1981) which stimulate atypical β-adrenoceptors at higher concentrations (Mohell & Dicker, 1989; Engel et al., 1981). The CGP 12177A-induced relaxation was shown to be resistant to blockade by propranolol, confirming an action at atypical β-adrenoceptors and in agreement with the findings of Oriowo in rat carotid artery (Oriowo, 1994) and aorta (Oriowo, 1995). Relaxation was also produced by selective β3-adrenoceptor agonists, BRL 37344 (Arch et al., 1984), ZD 2079 (Grant et al., 1994) and ZM 215001 (Tesfamariam & Allen, 1994). Propranolol had no effect on ZM 215001-induced relaxation, confirming previous observations that the effects of selective β3-agonists on vascular smooth muscle are unaffected by propranolol (Oriowo, 1994; Sooch & Marshall, 1997). Thus it is unlikely that any of the relaxant effects produced by the atypical β-adrenoceptor agonists seen in the present study were mediated via classical β-adrenoceptors.
The order of potency obtained, with the unconventional partial agonists more potent than the selective β3-adrenoceptor agonists, is contrary to that obtained at β3-adrenoceptors in other rat tissues e.g. white fat cells (Langin et al., 1991), ileum (Hoey et al., 1996), gastric fundus (McLaughlin & MacDonald, 1991) and colon (Kaumann & Molenaar, 1996), suggesting that the atypical β-adrenoceptors in rat aorta are not identical to β3-adrenoceptors. The order of potency is in agreement with Oriowo (1994) who also found CGP 12177A to be more potent than BRL 37344. The potency order raises the possibility that the atypical β-adrenoceptor in rat aorta is similar to the putative β4-adrenoceptor, which is also stimulated by unconventional partial agonists (Malinowska & Schlicker, 1996; Kaumann & Molenaar, 1996; Galitzky et al., 1997). Against this, however, is the evidence that selective β3-agonists such as BRL 37344 are reported to have no activity at the β4-adrenoceptor (Malinowska & Schlicker, 1996; Kaumann & Molenaar, 1996; Galitzky et al., 1997). In addition, cyanopindolol, which was more potent than CGP 12177A in rat aorta in this study, is reported to have lower potency (Malinowska & Schlicker, 1996), or lower efficacy (Kaumann, 1996; Malinowska & Schlicker, 1996) than CGP 12177A at the putative β4-adrenoceptor. Thus the agonist characterization, while corresponding to an atypical β-adrenoceptor, does not fully conform to either β3- or β4-adrenoceptor subtypes.
The novel selective β3-adrenoceptor antagonist, SR 59230A (Manara et al., 1996), in the presence of propranolol to block β1- and β2-adrenoceptors, failed to modify the isoprenaline CRC. In addition, relaxant responses induced by CGP 12177A were resistant to blockade by SR 59230A. Therefore, the atypical β-adrenoceptors in rat aorta do not appear to correspond to the β3-adrenoceptor.
Further evidence to support this comes from the results using cyanopindolol as an antagonist. Although cyanopindolol is a non-conventional partial agonist (see above), it has been used as a relatively potent β3-adrenoceptor antagonist in gut tissues, with a pKb of 7.1–7.5 (Blue et al., 1989; McLaughlin & MacDonald, 1990; 1991; Oriowo, 1994; Kelly & Houston, 1996; MacDonald & Watt, 1999). In the present study cyanopindolol was used as an antagonist at a concentration of 1 μM. This concentration also produced some agonist activity at atypical β-adrenoceptors (approximately 20% relaxation). This agonist activity is reflected in a reduction in the size of the noradrenaline pre-constriction and possibly in a lowering of the slope of the isoprenaline CRC. The antagonist effects of cyanopindolol against isoprenaline were similar to, and not additive with, the effects of propranolol suggesting that the antagonism is due to blockade of β1- and/or β2-adrenoceptors. The lack of effect of cyanopindolol on CGP 12177A confirms the lack of effect on atypical β-adrenoceptor-mediated responses in rat aorta in this study. This is in agreement with the findings of Oriowo (1994) who showed that cyanopindolol did not inhibit effects of isoprenaline in rat aorta although it had the expected effect against isoprenaline at β3-adrenoceptors in the distal colon and fundic strip.
Responses to isoprenaline (in the presence of propranolol) and CGP 12177A were inhibited by bupranolol. Bupranolol is a potent β1- and β2-adrenoceptor antagonist with weaker blocking activity at β3- (Langin et al., 1991; Blin et al., 1994; Gauthier et al., 1996; Kaumann & Molenaar, 1996; Malinowska & Schlicker, 1997) and β4- (Kaumann & Molenaar, 1996; Kaumann, 1996; Malinowska & Schlicker, 1996; 1997) adrenoceptors. Taken together with the lack of effect of SR 59230A, these results support the presence of a β4-adrenoceptor. However, the antagonism of isoprenaline by bupranolol appeared to be non-competitive, with a lowering of the maximum response. In addition, the antagonism of CGP 12177A gave low estimates of affinity for bupranolol of 5.2–5.5 which is an order of magnitude lower than reported by most authors for β3- and β4-adrenoceptors (e.g. 6.3 and 6.4–6.8 respectively (Kaumann & Molenaar, 1996)) although Malinowska & Schlicker (1996; 1997) reported similar estimates of affinity.
Responses to isoprenaline (in the presence of propranolol) and CGP 12177A were also inhibited by μM concentrations of CGP 20712A. High concentrations of CGP 20712A are reported to block β4-adrenoceptors in preference to β3-adrenoceptors (Kaumann & Molenaar, 1996; Galitzky et al., 1997; Malinowska & Schlicker, 1997) and thus this provides further support for the presence of β4-adrenoceptors. The pA2 estimates obtained with the lowest concentration of CGP 20712A (6.6, 6.2) are in good agreement with the values obtained at cardiac β4-adrenoceptors (Kaumann & Molenaar, 1996; Malinowska & Schlicker, 1997). Again, however, the evidence is not unequivocal since the antagonism was not simple competitive, with no further shifts at the higher concentration of 100 μM. The lack of simple competitive antagonism of CGP 20712A (and bupranolol) may be due to other actions at the high concentrations which have to be employed to block β4-adrenoceptors. However, at the concentrations used, there were no effects seen on the size of noradrenaline constriction or on acetylcholine relaxation.
The present study has not addressed the role of endothelium in the relaxant responses mediated by atypical β-adrenoceptors. However, we have shown elsewhere that removal of endothelium or treatment with the nitric oxide synthase inhibitor, L-NAME, attenuated relaxant responses to isoprenaline to a greater extent than responses to atypical β-adrenoceptor agonists (Brawley et al., 1998; MacDonald et al., 1999). In addition, after L-NAME treatment or removal of endothelium, relaxant responses to isoprenaline were unaffected by propranolol, suggesting that they were mediated only by atypical β-adrenoceptors (Brawley et al., 1998). Thus it appears that the endothelium/nitric oxide pathway modulates responses mediated via classical β-adrenoceptors to a greater extent than responses mediated via atypical β-adrenoceptors. This may be explained by a different distribution of receptors, with the classical β-adrenoceptors located mainly on endothelial cells, or by a differential effect of nitric oxide on the classical and atypical β-adrenoceptor signalling pathways (Brawley, Shaw & MacDonald, unpublished).
In conclusion, our results have confirmed that atypical β-adrenoceptors are present in rat aorta. Although β3-adrenoceptor-selective agonists produce relaxation, the receptor does not appear to correspond to the β3-adrenoceptor. There are similarities with the putative β4-adrenoceptor although the lack of a potent, selective antagonist makes any conclusion tentative at this stage. The vascular atypical β-adrenoceptor has the following properties: (a) stimulation by non-conventional partial agonists such as CGP 12177A; (b) resistant to blockade by propranolol; (c) moderate potency for selective β3-adrenoceptor agonists such as BRL 37344; (d) resistant to blockade by selective β3-adrenoceptor antagonists such as SR 59230A and (e) weak blockade by bupranolol and CGP 20712A at μM concentrations.
Acknowledgments
L. Brawley was supported by a Glasgow Caledonian University studentship. We are grateful to Novartis Pharma A.G. (CGP 20712A, CGP 12177A), Sanofi Reserche (SR 59230A) and Schwarz Pharma A.G. (bupranolol) for gifts of drugs.
Abbreviations
- CR
agonist concentration ratio
- CRC
concentration-response curve
References
- ARCH J.R.S. The brown adipocyte β-adrenoceptor. Proc. Nutr. Soc. 1989;48:215–223. doi: 10.1079/pns19890032. [DOI] [PubMed] [Google Scholar]
- ARCH J.R.S., AINSWORTH A.T., CAWTHORNE M.A., PIERCY V., SENITT M.V., THODY V.E., WILSON S. Atypical β-adrenoceptor on brown adipocytes as target for anti-obesity drugs. Nature. 1984;309:163–165. doi: 10.1038/309163a0. [DOI] [PubMed] [Google Scholar]
- ARCH J.R.S., KAUMANN A.J. β3 and atypical β-adrenoceptors. Med. Res. Rev. 1993;13:663–729. doi: 10.1002/med.2610130604. [DOI] [PubMed] [Google Scholar]
- BLIN N., NAHMIAS C., DRUMARE M.F., STROSBERG A.D. Mediation of most atypical effects by species homologues of the β3-adrenoceptor. Br. J. Pharmacol. 1994;112:911–919. doi: 10.1111/j.1476-5381.1994.tb13167.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BLUE D.R., BOND R.A., ADHAM N., DELMONDO R., MICHEL A., EGLEN R.M., WHITING R.L., CLARKE D.E.Interaction of dihydroalprenolol and cyanopindolol with atypical β-adrenoceptors in guinea-pig ileum Br. J. Pharmacol. 198996242P [PubMed] [Google Scholar]
- BRAWLEY L., MACDONALD A., SHAW A.M.Influence of L-NAME and removal of endothelium on noradrenaline contraction and isoprenaline relaxation in rat isolated thoracic aorta Br. J. Pharmacol. 1997122395P [Google Scholar]
- BRAWLEY L., MACDONALD A., SHAW A.M.Role of endothelium in classical and atypical β-adrenoceptor-mediated vasorelaxation in rat isolated aorta Br. J. Pharmacol. 199812518P [Google Scholar]
- EDVINSSON L., OWMAN C. Pharmacological characterization of adrenergic alpha and beta receptors mediating the vasomotor responses of cerebral arteries in vitro. Circ. Res. 1974;35:835–849. doi: 10.1161/01.res.35.6.835. [DOI] [PubMed] [Google Scholar]
- ENGEL G., HOYER D., BERTOLD R., WAGNER H. (±)[125Iodo]cyanopindolol, a new ligand for β-adrenoceptors: identification and quantification of subclasses of β-adrenoceptors in guinea pig. Naunyn-Schmiedebergs Arch. Pharmacol. 1981;317:277–285. doi: 10.1007/BF00501307. [DOI] [PubMed] [Google Scholar]
- GALITZKY J., LANGIN D., VERWAERDE P., MONTASTRUC J.-L., LAFONTAN M., BERLAN M. Lipolytic effects of conventional β3-adrenoceptor agonists and of CGP 12,177 in rat and human fat cells: preliminary pharmacological evidence for a putative β4-adrenoceptor. Br. J. Pharmacol. 1997;122:1244–1250. doi: 10.1038/sj.bjp.0701523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GAUTHIER C., TAVERNIER G., CHARPENTIER F., LANGIN D., LEMAREC H. Functional beta3-adrenoceptor in the human heart. J. Clin. Invest. 1996;98:556–562. doi: 10.1172/JCI118823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GRANT T.L., MAYERS R.M., QUAYLE S.P., BRISCOE M.G., HOWE R., RAO B.S.J.G., HOLLOWAY B.R.Zeneca ZD2079 is a novel β3-adrenoceptor agonist Br. J. Pharmacol. 1994112213P [Google Scholar]
- GRAY D.W., MARSHALL I. Novel signal transduction pathway mediating endothelium-dependent β-adrenoceptor vasorelaxation in rat thoracic aorta. Br. J. Pharmacol. 1992;107:684–690. doi: 10.1111/j.1476-5381.1992.tb14507.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HOEY A.J., JACKSON C.M., PEGG G.G., SILLENCE M.N. Atypical responses of rat ileum to pindolol, cyanopindolol and iodocyanopindolol. Br. J. Pharmacol. 1996;117:712–716. doi: 10.1111/j.1476-5381.1996.tb15248.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KAUMANN A.J. Is there a third heart β-adrenoceptor. Trends Pharmacol. Sci. 1989;10:316–320. doi: 10.1016/0165-6147(89)90065-5. [DOI] [PubMed] [Google Scholar]
- KAUMANN A.J. (−)-CGP 12177-induced increase of human atrial contraction through a putative third β-adrenoceptor. Br. J. Pharmacol. 1996;117:93–98. doi: 10.1111/j.1476-5381.1996.tb15159.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KAUMANN A.J., MOLENAAR P. Differences between the third cardiac β-adrenoceptor and the colonic β3-adrenoceptor in the rat. Br. J. Pharmacol. 1996;118:2085–2098. doi: 10.1111/j.1476-5381.1996.tb15648.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KELLY J., HOUSTON G. β3-adrenoceptors mediating relaxation of the oesophageal tunica muscularis mucosae and distal colon in the rat: comparative pharmacology and their desensitization by BRL 37344. J. Autonom. Pharmacol. 1996;16:205–211. doi: 10.1111/j.1474-8673.1996.tb00424.x. [DOI] [PubMed] [Google Scholar]
- LANDS A.M., ARNOLD A., MCAULIFF J.P., LUDUENA F.P., BROWN JUN T.G. Differentiation of receptor systems activated by sympathomimetic amines. Nature. 1967;214:597–598. doi: 10.1038/214597a0. [DOI] [PubMed] [Google Scholar]
- LANGIN D., PORTILLO M.P., SAULNIER-BLACHE J.-S., LAFONTAN M. Coexistence of three β-adrenoceptor subtypes in white fat cells of various mammalian species. Eur. J. Pharmacol. 1991;199:291–301. doi: 10.1016/0014-2999(91)90492-9. [DOI] [PubMed] [Google Scholar]
- MACDONALD A., MCLEAN M., MACAULAY L., SHAW A.M. Effects of propranolol and L-NAME on β-adrenoceptor-mediated relaxation in rat carotid artery. J. Autonom. Pharmacol. 1999;19:145–149. doi: 10.1046/j.1365-2680.1999.00128.x. [DOI] [PubMed] [Google Scholar]
- MACDONALD A., WATT K. Characterisation of the atypical β-adrenoceptor in rabbit isolated jejunum using BRL 37344, cyanopindolol and SR 59230A. J. Autonom. Pharmacol. 1999;19:91–96. doi: 10.1046/j.1365-2680.1999.00121.x. [DOI] [PubMed] [Google Scholar]
- MACDONALD P.S., DUBBIN P.N., DUSTING G.J. β-Adrenoceptors on endothelial cells do not influence release of relaxing factor in dog coronary arteries. Clin. Exper. Pharmacol. Physiol. 1987;14:525–534. doi: 10.1111/j.1440-1681.1987.tb01508.x. [DOI] [PubMed] [Google Scholar]
- MALINOWSKA B., SCHLICKER E. Mediation of the positive chronotropic effect of CGP 12177 and cyanopindolol in the pithed rat by atypical β-adrenoceptors, different from β3-adrenoceptors. Br. J. Pharmacol. 1996;117:943–949. doi: 10.1111/j.1476-5381.1996.tb15285.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MALINOWSKA B., SCHLICKER E. Further evidence for differences between cardiac atypical β-adrenoceptors and brown adipose tissue β3-adrenoceptors in the pithed rat. Br. J. Pharmacol. 1997;122:1307–1314. doi: 10.1038/sj.bjp.0701516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MANARA L., BADONE D., BARONI M., BOCCARDI G., CECCHI R., CROCI T., GIUDICE A., GUZZI U., LANDI M., LE FUR G. Functional identification of rat atypical β-adrenoceptors by the first β3-selective antagonists, aryloxypropanolaminotetralines. Br. J. Pharmacol. 1996;117:435–442. doi: 10.1111/j.1476-5381.1996.tb15209.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MCLAUGHLIN D.P., MACDONALD A. Evidence for the existence of ‘atypical' β-adrenoceptors (β3-adrenoceptors) mediating relaxation in the rat distal colon in vitro. Br. J. Pharmacol. 1990;101:569–574. doi: 10.1111/j.1476-5381.1990.tb14122.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MCLAUGHLIN D.P., MACDONALD A. Characterization of catecholamine-mediated relaxations in rat gastric fundus – evidence for an atypical β-adrenoceptor. Br. J. Pharmacol. 1991;103:1351–1356. doi: 10.1111/j.1476-5381.1991.tb09792.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MOHELL N., DICKER A. The β-adrenergic radioligand [3H]CGP-12177, generally classified as an antagonist, is a thermogenic agonist in brown adipose tissue. Biochemical Journal. 1989;261:401–405. doi: 10.1042/bj2610401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'DONNELL S.R., WANSTALL J.C. Beta-1 and Beta-2 adrenoceptor -mediated responses in preparations of pulmonary artery and aorta from young and aged rats. J. Pharmacol. Exp. Ther. 1984;228:733–738. [PubMed] [Google Scholar]
- O'DONNELL S.R., WANSTALL J.C. Responses to the β2-selective agonist procaterol of vascular and atrial preparations with different functional β-adrenoceptor populations. Br. J. Pharmacol. 1985;84:227–235. [PMC free article] [PubMed] [Google Scholar]
- ORIOWO M.A. Atypical beta-adrenoceptors in the rat isolated common carotid artery. Br. J. Pharmacol. 1994;113:699–702. doi: 10.1111/j.1476-5381.1994.tb17049.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ORIOWO M.A. Different atypical β-adrenoceptors mediate isoprenaline-induced vascular relaxation in vascular and non-vascular smooth muscles. Life Sci. 1995;56:PL269–PL275. doi: 10.1016/0024-3205(95)00076-3. [DOI] [PubMed] [Google Scholar]
- SOOCH S., MARSHALL I.An atypical β-adrenoceptor mediates relaxation of the rat isolated mesenteric artery Br. J. Pharmacol. 199511422P [Google Scholar]
- SOOCH S., MARSHALL I.Evidence for atypical β-adrenoceptors in rat vasculature Br. J. Pharmacol. 1996117261P [Google Scholar]
- SOOCH S., MARSHALL I. Atypical β-adrenoceptors in the rat vasculature. Ann. N.Y. Acad. Sci. U.S.A. 1997;812:211–212. doi: 10.1111/j.1749-6632.1997.tb48178.x. [DOI] [PubMed] [Google Scholar]
- STAEHELIN M., SIMONS P., JAEGGI K., WIGGER N. CGP 12177 A hydrophilic β-adrenergic radioligand reveals high affinity binding of agonists to intact cells. J. Biol. Chem. 1983;258:3496–3502. [PubMed] [Google Scholar]
- TAMAOKI J., TAGAYA E., ISONO K., NAGAI A. Atypical adrenoceptor-mediated relaxation of canine pulmonary artery through a cAMP-dependent pathway. Biochem. Biophys. Res. Comm. 1998;248:722–727. doi: 10.1006/bbrc.1998.9047. [DOI] [PubMed] [Google Scholar]
- TESFAMARIAM B., ALLEN G.T. β1- and β2-adrenoceptor antagonist activities of ICI-215001, a putative β3-adrenoceptor agonist. Br. J. Pharmacol. 1994;112:55–58. doi: 10.1111/j.1476-5381.1994.tb13028.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WILSON C., WILSON S., PIERCY V., SENNIT M.V., ARCH J.R.S. The rat lipolytic β-adrenoceptor: studies using novel β-adrenoceptor agonists. Eur. J. Pharmacol. 1984;100:309–319. doi: 10.1016/0014-2999(84)90007-4. [DOI] [PubMed] [Google Scholar]