

Abstract
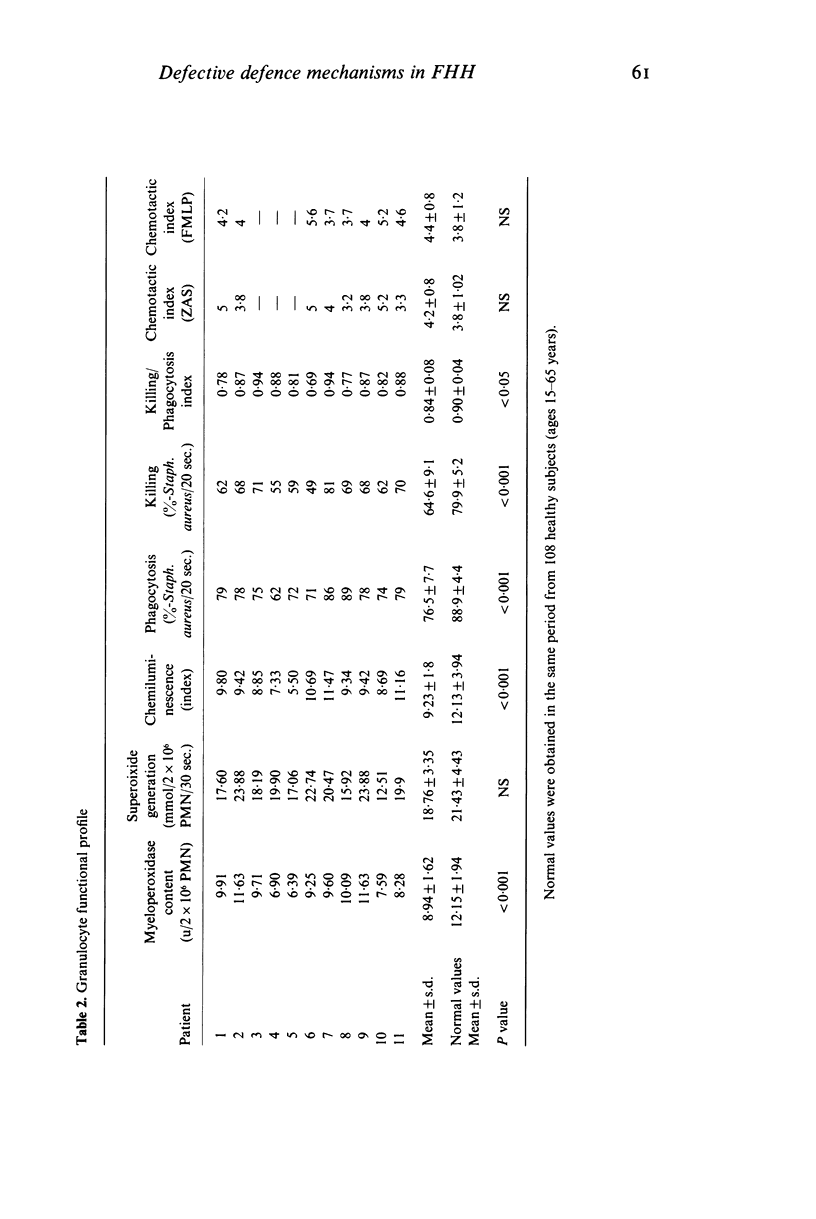
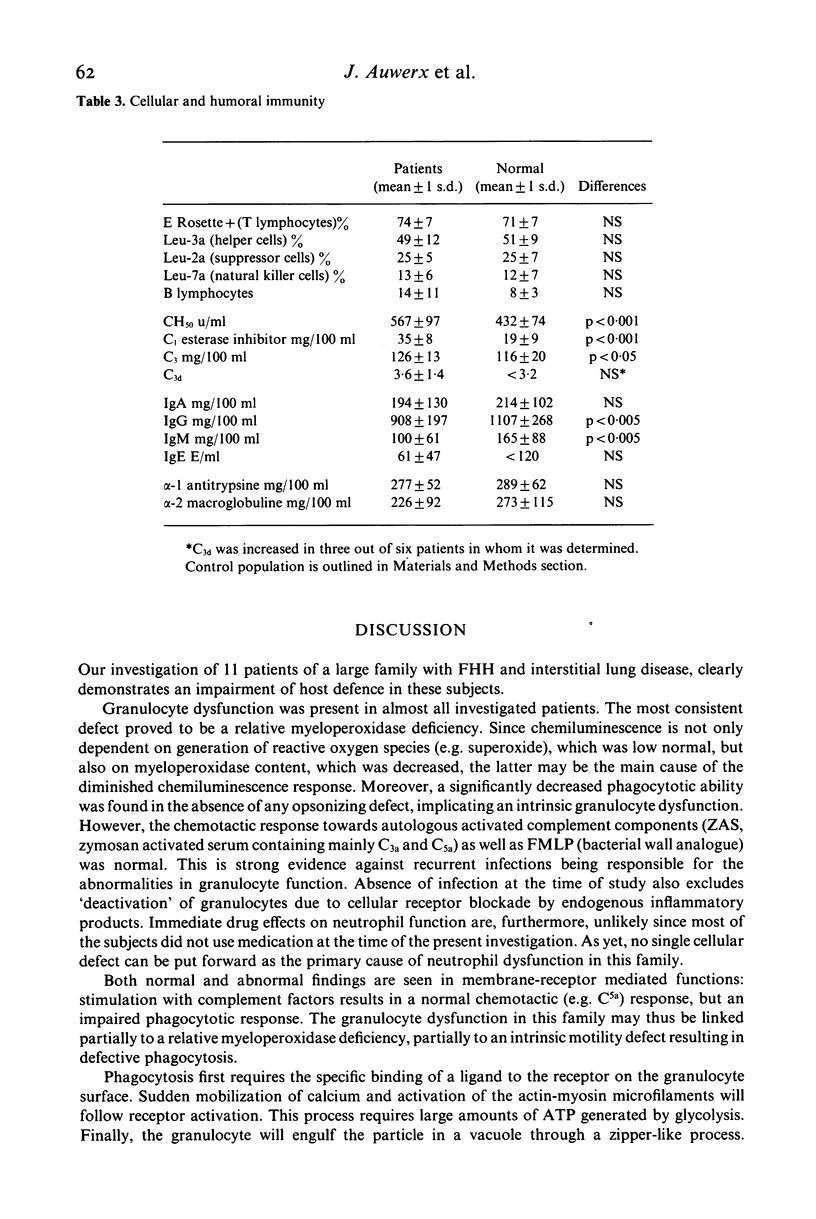
An extensive in vitro investigation of the host defence system was performed in 11 sibs of a large kindred with unexplained combination of familial hypocalciuric hypercalcaemia (FHH), interstitial lung disease and increased susceptibility to respiratory infections. The impairment of host defence mechanism was most likely related to granulocyte dysfunction. A severe myeloperoxidase deficiency was the most consistent granulocyte defect (P less than 0.001) and it was associated with a relatively diminished chemiluminescence (P less than 0.001). Moreover, a significantly diminished antistaphylococcal phagocytic (P less than 0.001) and killing (P less than 0.001) activity was found which in the absence of any opsonizing defect implicates an intrinsic granulocyte dysfunction. We found no abnormalities in number of B and T lymphocytes nor in the balance between helper and suppressor cells determined with monoclonal antibodies. Despite the recurrent infections no elevations of the immunoglobulin subclasses were found. The relationship between the inherited FHH, interstitial lung disease and susceptibility to respiratory infections remains obscure. It is, however, clear that impairment of the host defence might contribute to a decreased life expectancy in this family.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Abo T., Balch C. M. A differentiation antigen of human NK and K cells identified by a monoclonal antibody (HNK-1). J Immunol. 1981 Sep;127(3):1024–1029. [PubMed] [Google Scholar]
- Auwerx J., Demedts M., Bouillon R., Desmet J. Coexistence of hypocalciuric hypercalcaemia and interstitial lung disease in a family: a cross-sectional study. Eur J Clin Invest. 1985 Feb;15(1):6–14. doi: 10.1111/j.1365-2362.1985.tb00136.x. [DOI] [PubMed] [Google Scholar]
- Boogaerts M. A., Nelissen V., Roelant C., Goossens W. Blood neutrophil function in primary myelodysplastic syndromes. Br J Haematol. 1983 Oct;55(2):217–227. doi: 10.1111/j.1365-2141.1983.tb01241.x. [DOI] [PubMed] [Google Scholar]
- Demedts M., Auwerx J., Goddeeris P., Bouillon R., Gyselen A., Lauweryns J. The inherited association of interstitial lung disease, hypocalciuric hypercalcemia, and defective granulocyte function. Am Rev Respir Dis. 1985 Mar;131(3):470–475. doi: 10.1164/arrd.1985.131.3.470. [DOI] [PubMed] [Google Scholar]
- Fehr J., Jacob H. S. In vitro granulocyte adherence and in vivo margination: two associated complement-dependent functions. Studies based on the acute neutropenia of filtration leukophoresis. J Exp Med. 1977 Sep 1;146(3):641–652. doi: 10.1084/jem.146.3.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foley T. P., Jr, Harrison H. C., Arnaud C. D., Harrison H. E. Familial benign hypercalcemia. J Pediatr. 1972 Dec;81(6):1060–1067. doi: 10.1016/s0022-3476(72)80232-4. [DOI] [PubMed] [Google Scholar]
- Heath H., 3rd, Purnell D. C. Urinary cyclic 3',5'-adenosine monophosphate responses to exogenous and endogenous parathyroid hormone in familial benign hypercalcemia and primary hyperparathyroidism. J Lab Clin Med. 1980 Dec;96(6):974–984. [PubMed] [Google Scholar]
- Ledbetter J. A., Evans R. L., Lipinski M., Cunningham-Rundles C., Good R. A., Herzenberg L. A. Evolutionary conservation of surface molecules that distinguish T lymphocyte helper/inducer and cytotoxic/suppressor subpopulations in mouse and man. J Exp Med. 1981 Feb 1;153(2):310–323. doi: 10.1084/jem.153.2.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marx S. J., Spiegel A. M., Brown E. M., Koehler J. O., Gardner D. G., Brennan M. F., Aurbach G. D. Divalent cation metabolism. Familial hypocalciuric hypercalcemia versus typical primary hyperparathyroidism. Am J Med. 1978 Aug;65(2):235–242. doi: 10.1016/0002-9343(78)90814-8. [DOI] [PubMed] [Google Scholar]
- Marx S. J., Spiegel A. M., Sharp M. E., Brown E. M., Gardner D. G., Downs R. W., Jr, Attie M. F., Stock J. L. Adenosine 3',5'-monophosphate response to parathyroid hormone: familial hypocalciuric hypercalcemia versus typical primary hyperparathyroidism. J Clin Endocrinol Metab. 1980 Mar;50(3):546–548. doi: 10.1210/jcem-50-3-546. [DOI] [PubMed] [Google Scholar]
- Nelson R. D., Herron M. J., Schmidtke J. R., Simmons R. L. Chemiluminescence response of human leukocytes: influence of medium components on light production. Infect Immun. 1977 Sep;17(3):513–520. doi: 10.1128/iai.17.3.513-520.1977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson R. D., Quie P. G., Simmons R. L. Chemotaxis under agarose: a new and simple method for measuring chemotaxis and spontaneous migration of human polymorphonuclear leukocytes and monocytes. J Immunol. 1975 Dec;115(6):1650–1656. [PubMed] [Google Scholar]
- Perrin L. H., Lambert P. H., Miescher P. A. Complement breakdown products in plasma from patients with systemic lupus erythematosus and patients with membranoproliferative or other glomerulonephritis. J Clin Invest. 1975 Jul;56(1):165–176. doi: 10.1172/JCI108065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tan J. S., Watanakunakorn C., Phair J. P. A modified assay of neutrophil function: use of lysostaphin to differentiate defective phagocytosis from impaired intracellular killing. J Lab Clin Med. 1971 Aug;78(2):316–322. [PubMed] [Google Scholar]