

Abstract
Background
The main goal of physical therapy treatment (PT) in the clinical stage following total knee arthroplasty (TKA) is to prepare patients for discharge from the hospital as soon as possible after their operation. Although aggressive rehabilitation is believed to be important, evidence of effects of different exercise programmes following TKA is limited. This led to the question whether the intensity of PT (once versus twice daily) following TKA affects short-term recovery, measured as range of motion.
Methods
A randomised controlled trial compared an exercise regimen of two sessions per day with a similar programme administered once daily. Primary outcome measure was ROM.
Results
At the time of hospital discharge, there was no difference between the experimental and control groups in range of motion.
Conclusion
This study shows that in our setting twice daily PT sessions do not produce different results as daily PT sessions. It may be questioned whether multiple daily therapy sessions are needed as an in-hospital PT regimen in OA total knee patients.
Background
Recent trends in the treatment of patients following orthopaedic surgery in the Netherlands encourage early discharge from hospitals, which implies increasing the intensity of treatment during the in-hospital phase. The strategy of choice involves mobilisation of the joints, starting on the day of surgery as well as shortening the bed rest phase and early ambulation. Physical therapy treatment (PT) plays an important role in this strategy.
In 2000 a 'Joint Care' programme was implemented at the University Hospital Maastricht. This is a clinical pathway in which the activities of physicians, nurses, physical therapists and other staff inside as well as outside the hospital are coordinated to provide the best overall care for patients with a particular diagnosis or procedure[1].
Clinical pathways are used in many institutions for patients undergoing total knee arthroplasty (TKA) and total hip arthroplasty (THA). These procedures lend themselves very well to a pathway approach, because the process of care is relatively standardized. Clinical pathways have been successful in reducing costs and length of stay in acute care hospitals, while not compromising patient outcomes [1-7]. The contents of the individual treatments are hospital-specific to create an optimal regimen of care tailored to that specific institution. The main goal in the clinical stage is to prepare patients for discharge from the hospital as soon as possible after their operation. Discharge depends primarily on restoring sufficient functional range of motion (ROM)[8].
Various authors [9-12] have described aggressive rehabilitation schemes incorporating more than one PT treatment session per day in the clinical phase following total knee surgery. Aggressive rehabilitation is believed to be important in preventing postoperative contracture of the soft tissue and in gaining better flexion. Nevertheless evidence of effects of different exercise programs following TKA is limited[13]. Our current PT programme is based on these rehabilitation schemes, as well as on the outcome of a nonrandomised controlled trial[14] comparing usual care with a 'Joint Care' clinical pathway. This trial found the length of hospital stay to be significantly shorter in the 'Joint Care' group. The author concluded that this was mainly caused by the greater stimulation to exercise and the number of minutes of PT per day. Patients were not only stimulated by their physical therapists to exercise, but the nursing staff also stimulated the patients to exercise and perform daily life activities themselves. Based on this result we doubled the time spent on in-hospital PT from 20 minutes to 40 minutes per patient per day, thus increasing treatment intensity to fulfil one of the goals of the programme; shortening hospital stay to four days after surgery. Patients are scheduled for discharge the fourth day after surgery if their passive flexion ROM exceeds 65°, when they are able to transfer from sitting to standing, walk independently, and are able to climb stairs, if necessary.
After two years of experience with the high intensity approach, the mean hospital stay was reduced to approximately four days after the operation. In 2003, however budget considerations meant that continuation of the extra PT sessions was being reconsidered. This led to a debate within the PT department whether or not the extra time investment should be maintained, i.e. whether the second daily visit was essential in reaching the short-term PT goals and whether having only one session of PT a day would lead to poorer range of motion (ROM) and function.
This resulted in the following research question. Does the intensity of PT treatment (once versus twice daily) in patients following TKA affect their short-term recovery, measured as range of motion?
To answer this question, a randomised controlled in-hospital trial was conducted in which a regimen consisting of four days with 40 minutes of PT a day was compared with one involving 20 minutes of PT a day.
Methods
The medical ethics committee of the Maastricht University Hospital and Maastricht University approved this prospective, randomised controlled trial.
The design of the trial is depicted in figure 1.
Figure 1.
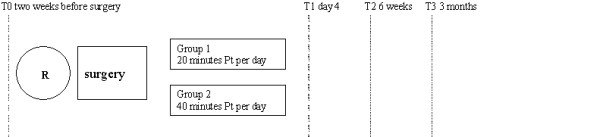
research design and outcome assessment. T0 baseline assessment, two weeks before surgery, T1 assessment 4 days after surgery, T2 assessment 6 weeks after surgery, T3 assessment 3 months after surgery. R = Randomisation.
Subjects
A consecutive series of patients who received a primary TKA at the University Hospital Maastricht, the Netherlands, was invited to participate between 1 January and 1 June, 2004. Subjects were considered eligible for the study if they were scheduled in the 'Joint Care' programme and signed an informed consent form.
Patients undergoing knee revision surgery were excluded as were patients over 85 years of age, patients with co-morbidity influencing gait and patients who did not understand or speak Dutch.
Randomisation
An independent research assistant performed concealed randomization using a computer generated randomisation schedule in which patients were allocated according to a weekly treatment regimen. All patients are admitted into hospital on Monday evening, surgery is on Tuesdays and hospital leave is planned the next Saturday. By randomising clusters of treatment weeks instead of individual randomisation we made sure that patients within the same treatment week all received the same postoperative treatment regime, thus avoiding contamination, which might occur when patients receive different regimes in the same week of admission at the same ward.
Information on the particular treatment intensity was given on the day of surgery. In this way we prevented foreknowledge of treatment assignment and thus shielded those who enrolled participants from being influenced by this knowledge because enrolment into the study was conducted two weeks before surgery.
Interventions
Clinical phase
During the in-hospital phase daily PT was administered to all participating patients. Patients in the experimental group were treated twice daily (totalling 40 minutes per day), patients in the control group once daily (20 minutes per day). The treatment content was similar in both groups and consisted of active and passive mobilisation of the knee, strengthening of the quadriceps muscle and functional exercises including transfers from a supine position to sitting and from sitting to standing, walking and stair climbing. As a rule, patients left hospital after the morning PT sessions on the fourth day after surgery, leading to a total number of PT sessions in the experimental group of seven sessions compared to four sessions in the control group.
A detailed description of the treatment protocol following total knee surgery is available at the website of the Physical Therapy department of the Maastricht University Hospital[15] We divided the treating physical therapists into two groups. One group treated all patients in the morning, while the optional second treatment sessions were administered by other physical therapists, leaving the group of therapists who treated the patients in the morning sessions unaware whether or not patients were receiving a second PT session. Therapist received weekly work schedules. During the study period therapist shifted from morning to afternoon groups randomly over treatment weeks. These changes were introduced to balance the work load of the participating therapist rather than for study purposes.
Hospital discharge followed when patients showed wound healing, they were ambulant using a walking frame or crutches and passive flexion ROM of the knee was above 65 degrees.
Outcome measures
Primary outcome measure in this study was passive flexion ROM.
Secondary outcome measures were active ROM and passive extension ROM, functional status, length of stay (LOS) after surgery, pain over the last 24 hours (using an 11 point scale), satisfaction with treatment (using an 11 point scale from totally dissatisfied to completely satisfied)[16], satisfaction with the intermediate treatment results and global perceived effect.
ROM was measured actively as well as passively using a large goniometer following the method described by Brosseau[17]. Intratester reliability for knee flexion is 0.99, for active extension 0.97. Criterion validity for knee flexion 0.98, for extension 0.42[17].
Functional status was measured using two scales, the disease specific Western Ontario and McMaster University Osteoarthritis index (WOMAC)[18] and the joint specific Knee Society Scale (KSS)[19].
The WOMAC is a disease specific questionnaire developed specifically for people with osteoarthritis of the hip and knee. Using visual analog scales, its 24 items probe 3 dimensions – pain (5 items), stiffness (2 items), and functional difficulty (17 items). Scale sum scores were standardised (0–100), with high values indicating less pain or better physical functioning[20].
The WOMAC questionnaire is well recognized for its good validity, reliability and responsiveness. We used the Dutch version of WOMAC[20].
The KSS is concise and easy to use. It represents a clear attempt to separate knee function from overall patient functional status. Bach et al[21] reported that reproducibility of the knee score is poor whilst the function score shows good reproducibility. The construct validity of the KSS is good[22].
At follow-up, patients were asked to judge the effect of the surgery on a 7-point likert scale from 'worse than ever' status to 'completely recovered'[23].
The primary effect measurement was scheduled for the fourth day after surgery, while follow-up measurements were scheduled at 6 weeks and 3 months after surgery.
Table 1 shows the timing and measurement tools used. The outcome assessor was blinded with regard to the a clinical intervention regime administered.
Table 1.
outcome measures and timing ROM = Range of Motion
| T0 | T1 | T2 | T3 | |
| ROM | X | X | X | X |
| Functional status WOMAC | X | X | X | |
| Functional status KSS | X | X | X | X |
| Length of stay | X | |||
| Pain | X | X | X | X |
| Treatment satisfaction | X | X | X | |
| Satisfaction with intermediate results | X | X | X | |
| Number of PT sessions | X | |||
| Global perceived effect of total treatment by the patient | X | X | X |
T0, 14 days prior to surgery
T1, 4 days after surgery
T2, 6 weeks after surgery
T3, 3 months after surgery
We selected the KSS score as functional outcome on day four because several items in the WOMAC are not applicable during the in-hospital period. The WOMAC was assessed during the outpatient period because psychometric properties of the WOMAC are superior to the KSS.
Sample size
A 10° of passive ROM difference between groups was considered clinically important enough to eventually raise treatment frequency. The sample size needed to detect a significant difference (2-sided, α <. 05) of at least 10° ROM between groups (primary outcome) with an assumed standard deviation (SD) of 10° and a power of 0.8, was 16 subjects per group. To compensate for a maximally acceptable 20% loss of subjects between baseline and follow-up, 20 subjects per group (40 in total) were required.
Analyses
Data were checked for completeness and normality. Statistical analyses were blinded and performed according to the 'intention-to-treat' principle. Descriptive statistics were calculated of both group statuses at baseline. Post treatment scores as well as differences between pre- and post treatment scores were compared with regard to all outcome measures. Group differences and 95% confidence intervals (CI) were computed for all outcome measures. The scores on global perceived effect were dichotomized to examine the ratio of improved versus unimproved patients. Patients were scored as improved if they felt much better or had recovered completely. Student's t-test was used for continuous data to determine differences between the two treatment groups. Chi-square tests were used for analyses of categorical data and when continuous data were not normally distributed. All data were analysed using SPSS version 11.0[24].
Results
Of the 55 subjects who were scheduled for surgery between January and June 2004, 43 were included in the study. 9 patients refused to participate and 3 were excluded because they had relevant co-morbidities. Twenty-one patients were randomly assigned to the experimental group, 22 to the control group.
The baseline characteristics of the patients in the two groups were similar in terms of clinical and demographic characteristics. They also showed comparable levels of functional ability and Quality of Life (table 2).
Table 2.
patient's baseline characteristics
| Variable | Experimental group n = 21 | Control group n = 22 | ||
| Female/Male | 15/6 | 17/5 | ||
| Mean | sd | |||
| age | 70 | (8.5) | 67 | (7) |
| active ROM extension (degrees) | 8° | (6°) | 8° | (5°) |
| passive ROM extension (degrees) | 5° | (5°) | 5° | (5°) |
| active ROM flexion (degrees) | 106° | (19°) | 102° | (20°) |
| passive ROM flexion (degrees) | 110° | (19°) | 114° | (15°) |
| functional status WOMAC | 44 | (16.7) | 40 | (16.6) |
| WOMAC subscale pain | 9.2 | (2.7) | 8.3 | (3.5) |
| WOMAC subscale stiffness | 3.7 | (1.1) | 3.3 | (1.4) |
| WOMAC subscale difficulty | 31.1 | (9.3) | 28.2 | (11.8) |
| functional status KSS knee | 49 | (18) | 43 | (21) |
| KSS function | 53 | (18) | 52 | (21) |
| Pain (11 point scale) | 3,7 | (2,8) | 3,5 | (3,3) |
All 43 patients were assessed two weeks before surgery (T0) and four days after surgery (T1).
Six weeks after the operation (T2) 2 patients of the control group failed to attend the follow-up measurement, thus data from 41 patients were available for intention to treat analyses. All participants attended the follow-up measurements at 3 months.
Outcome 4 days after surgery
As can be seen from table 3, there was no detectable difference in the primary outcome measure ROM between the experimental and control groups four days after surgery. Patients in the control group all received 4 treatment sessions. Two patients in the experimental group received six of the seven possible treatment sessions. One of these patients did not feel well enough to participate in a second PT session on the second day after surgery. The other patient left the hospital on the third day after surgery. The surgeon approved his discharge since he had reached the short-term treatment goals and asked to return home for personal reasons. Length of stay was similar in both groups. One patient in the control group was transferred to the cardiology department because of cardiac complaints. He left the hospital 15 days after surgery.
Table 3.
between group differences at day 4 after surgery (scheduled hospital discharge) T1 and differences between status 14 days prior to surgery and 4 days after surgery
| Variable | Experimental group n = 21 | Control group n = 22 | Mean difference | 95%CI | P-value | Differences between t0 and t1 | Mean difference | 95%CI | P-value | |||||
| Experimental group | Control group | |||||||||||||
| Mean | sd | Mean | sd | Mean | sd | Mean | sd | |||||||
| ROM active extension (degrees) | 8.4 | 5.1 | 7.8 | 5.6 | 0.56 | -2.7 – 3.8 | 0.73 | 0.71 | 8.6 | 0.14 | 5.2 | 0.57 | -3.9 – 5.0 | 0.46 |
| ROM passive extension (degrees) | 5.5 | 4.5 | 5.8 | 4.9 | -0.3 | -3.2 – 2.6 | 0.81 | 0.1 | 7.2 | 0.4 | 4.7 | -0.3 | -4.2 – 3.2 | 0.78 |
| Rom active flexion (degrees) | 69.8 | 11.9 | 70.4 | 13.3 | -0.5 | -8.3 – 7.3 | 0.90 | 36.1 | 22.0 | 31.5 | 17.8 | 4.6 | -7.8 -16.9 | 0.79 |
| ROM passive flexion (degrees) | 77.7 | 11.2 | 77.9 | 12.8 | -0.2 | -7.7 – 7.2 | 0.95 | 36.6 | 17.9 | 32.1 | 18.4 | 4.5 | -6.8 – 15.6 | 0.43 |
| Functional status KSS knee | 54.3 | 15.2 | 52.2 | 17.8 | 1.1 | -8.7 – 12.3 | 0.68 | 9.3 | 22.7 | 4.4 | 26.3 | 4.9 | -20 – 10.2 | 0.52 |
| Functional status KSS function | 29.3 | 10.7 | 22.9 | 13.2 | -6.4 | -1.1 – 13.8 | 0.09 | -24 | 23.4 | -29 | 19.3 | -5 | -18 – 7.9 | 0.43 |
| Length of stay | 4.1 | 0.9 | 4.5 | 1.3 | 0.4 | -0.3 – 1.0 | 0.34 | - | - | - | - | |||
| Pain (11 point scale) | 3.6 | 2.3 | 3.6 | 2.8 | 0 | -1.6 – 1.6 | 0.97 | -0.14 | 3.1 | 0.1 | 3.5 | 0.04 | -1.8 – 2.3 | 0.82 |
| Satisfaction with treatment (11-point scale) | 9.1 | 0.8 | 9.1 | 0.7 | 0 | -0.5 – 0.5 | 0.99 | - | - | - | - | |||
Flexion contracture was about 8° in both groups and active flexion ROM was about 70° Functional status results on day four were also similar between groups.
Six-weeks and three-months follow-up
There were no significant or clinically relevant differences in the secondary outcome measures at any of the other follow-up moments (table 4). Follow-up data were comparable to those at day four after surgery. ROM in extension seemed to be a little better in the control group, as was satisfaction with the overall treatment. Recovery of flexion range of motion as well as functional status is similar in both groups.
Table 4.
Six weeks and three months follow-up
| 6 weeks | 3 months | |||||||||||
| Exp n = 21 | Control n = 20 | Mean difference | 95%CI | Exp n = 21 | Control n = 22 | Mean difference | 95% CI | |||||
| mean | sd | mean | sd | mean | sd | mean | sd | |||||
| ROM active extension (Degrees) | 6.8 | 5.0 | 10.3 | 6.6 | -3.5 | -7.3 – 1.8 | 5.3 | 5.1 | 8.3 | 5.5 | -3 | -6.7 – 0.3 |
| ROM passive extension (Degrees) | 4.3 | 3.4 | 7.6 | 6.8 | -3.3 | -6.8 – 0.7 | 3.8 | 4.3 | 5.5 | 4.6 | -1.7 | -4.5 – 1.03 |
| Rom active flexion (Degrees) | 97.8 | 16.0 | 98 | 14.2 | -0.2 | -9.8 – 9.4 | 103.7 | 13 | 105.1 | 15 | -1.4 | -10.0 – 7.3 |
| ROM passive flexion (Degrees) | 102.6 | 16.4 | 102.5 | 14.2 | 0.1 | -9.5 – 9.8 | 109 | 13 | 109.3 | 14.8 | -0.3 | -8.9 – 8.3 |
| Functional status WOMAC | 68.6 | 18.3 | 74.7 | 12.1 | -5.9 | -15.8 – 3.7 | 73.4 | 14.9 | 78.0 | 11.3 | -4.6 | -13 8 – 3.9 |
| WOMAC subscale pain | 14.2 | 3.9 | 15.6 | 2.5 | -1.4 | -3.4 – 0.69 | 15.2 | 3.0 | 16.2 | 2.4 | -1 | -2.7 – 0.7 |
| WOMAC subscale stiffness | 5.7 | 1.6 | 6.3 | 1.1 | -0.6 | -1.4 – 0.25 | 6.1 | 1.2 | 6.5 | 1.1 | -0.4 | -1.04 – 0.32 |
| WOMAC subscale difficulty | 48.6 | 12.9 | 52.9 | 8.4 | -4.3 | -11.2 – 2.5 | 51.9 | 10.6 | 55.3 | 8.3 | -3.4 | -9.2 – 2.5 |
| Functional status KSS knee | 71 | 18 | 77 | 13 | -6 | -16.1 – 4.1 | 80 | 17 | 80 | 18 | 0 | -11.3 – 11.3 |
| Functional status KSS function | 60 | 14 | 58 | 18 | 2 | -8.3 – 12.1 | 69 | 15 | 69 | 20 | 0 | -11. -11.0 |
| Pain (11-point scale) | 1.8 | 2.5 | 2.4 | 2.5 | -0.6 | -2.2 – 0.9 | 1.3 | 1.9 | 0.8 | 1.5 | 0.5 | -0.6 – 1.6 |
| Satisfaction with treatment (11-point scale) | 8.5 | 2.0 | 9.3 | 0.9 | -0.8 | -1.8 – 0.2 | 8.7 | 1.6 | 9.4 | 0.9 | -0.7 | -1.5 – .15 |
| Perceived effect Improved/not | 18/2 | 18/3 | 21/1 | 18/3 | ||||||||
Discussion
This trial did not detect any differences in the effects on any of the outcome parameters between regimens involving one or two physical therapy sessions a day in the clinical phase following TKA.
Remarkably, patients seemed to be very satisfied with PT treatment, irrespective of the number of sessions. Three months after surgery, the perceived effect of the total treatment was high, with 39 out of 43 patients stating that they had vastly improved or were completely cured.
De Jong[14] reported similar numbers of PT sessions and comparable hospital stay (4.97 days) after surgery compared to our experimental group (4.1 days). De Jong did not report on ROM and functional capacity was measured using a scale of unknown reliability and validity.
Since we did not find any other studies on the effects of different PT treatment intensities following TKA, it is only possible to compare the results of the total group with those of other studies with known treatment intensity.
Most studies on rehabilitation after TKA have focussed on the use of continuous passive motion treatment.
Several recent studies [9,25-27] incorporated high intensity basic PT rehabilitation programmes and describe outcomes comparable to our data. Two studies employed standardized PT treatments twice daily, whilst Kumar et al. reported 90 minutes to two hours of PT daily and Beaupre et al. did not standardize the treatment duration but reported on six treatment sessions during the first four days after surgery.
Three [9,25,26] studies described short-term results on range of motion.
The ROM we found four days after surgery is comparable to the values reported in these studies. The level of pain found in our study is in agreement with those reported by Bennett whereas the length of stay in Bennett's sample was longer (8.8 compared to 5 days), and KSS scores at 3-months follow-up were slightly better in our sample (mean KSS function score of 52 versus 69).
Our study only collected Womac data preoperative and at six-weeks and three-months follow- up. No WOMAC data were collected at hospital discharge because several items of the WOMAC score are not valid during hospital stay, items like getting in and out of a car, shopping, getting in and out of a bath and doing domestic chores are not applicable in this phase.
Study limitations
We chose cluster randomization of treatment weeks over individual randomization. By clustering in treatment weeks we made sure that all patients operated in a week were receiving the same amount of daily treatment sessions. We believe that this led to less bias than introduced by contamination in individual randomization. Patients receive PT treatment in the 'living room' of the orthopaedic ward in which they stay during daytime. We believe contamination is likely to occur when one patient would receive a second treatment in the afternoon whilst the patient sitting next to him/her is not. Conversation is overheard and just seeing treatment might encourage the patient to exercise them self, therewith diminishing contrast between both groups.
Though randomizing in clusters theoretically might inflict bias, we believed in this case it does not have a lot of influence. It is accepted that clustering may result in P values and confidence intervals which are sufficiently biased to have a major effect if any of the following are true: the cluster size is large, the number of clusters is small, or the intra-cluster correlation coefficient is large[28]. Our study contained 22 clusters, cluster sizes were small with a mean of two patients per cluster and intracluster correlation was very small, (icc = 0,171), leading up to a design effect of 1.171[29].
In combination with the fact that clusters were merely different weeks in a four months period in the same hospital with the same staff etc. makes us believe that clustering did not introduce a major bias in our study.
We chose passive flexion ROM as primary outcome measure because passive ROM is the only measure of function involved in hospital discharge in our situation. Therefore we based our sample size calculation on between group differences in passive flexion ROM.
When designing the study the therapists and orthopaedic surgeons involved discussed what effect would justify the effort of extra PT sessions daily. We had no information on possible effect sizes or minimally important clinical differences out of the literature, since we are unaware of a single similar study in this field. However we had some information on the effects of CPM in this same setting[30]. In this study we found an 8 degrees difference in flexion ROM when using CPM in the in hospital phase after total knee arthroplasty.
We agreed on a 10 degrees between group difference to be a result worth the extra PT effort. Although we did not detect a between group difference at all, one may state that our study was designed to find a large difference. Sample size was calculated to find this effect and therefore may be to small to detect smaller differences. Our study is underpowered to detect significantly smaller between group differences. For example, to detect a 5 degree difference sample size would a sample size of over 120 participants.
Although our study could not detect differences between groups receiving PT once or twice daily, this does not mean that individual patients might not benefit from more intensive PT. One of the primary issues in treating patients with TKA is to identify those patients that may require more intensive rehabilitation. Unfortunately, secondary analyses yielded no variables at baseline that predicted short-term postoperative recovery.
Different therapists treated patients in the morning and afternoon sessions as well as over different treatment days. This is a common procedure in our hospital which in itself might increase treatment variation. However, treatments were standardized and applied following a protocol.
In this study, PT treatment was standardized in terms of content as well as duration of the treatment sessions. Although almost every study in this field has done the same, one might question whether this is the appropriate way to handle patient care. It might be wiser to set treatment goals per day. As soon as the target for that day has been achieved no further treatment might be necessary. This would mean that the number of treatments can be individualized according to the goals set for each day.
Although blinding therapists is very difficult, we attempted to blind at least the physical therapists attending the morning session. Blinding was not successful in every case, because some patients gave information about the second session during the morning sessions.
Participating physical therapists stated that not knowing whether a patient would receive a second treatment session probably raised their awareness about achieving clinical goals during the morning sessions. Although they were aware that this attitude might bias study results, their attitude towards giving optimal patient care overruled the urge to follow the treatment protocol. In this sense one might say that treating patients once daily is just as good as twice daily if the physical therapists are more focussed.
Conclusion
This study shows that in our setting twice daily PT sessions do not produce different results as daily PT sessions. It may be questioned whether multiple daily therapy sessions are needed as an in-hospital PT regimen in OA total knee patients.
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
AFL participated in the design of the study, exercise intervention, assessments and follow-ups, statistical analyses and writing. YHFC, EMHW, MJAvS and RAdB participated in the study design and the interpretation of the data, and critically revised the article. RGTG and PAvdB participated in the interpretation of the data and critically revised the article. All authors read and approved the final manuscript.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Figure 2.
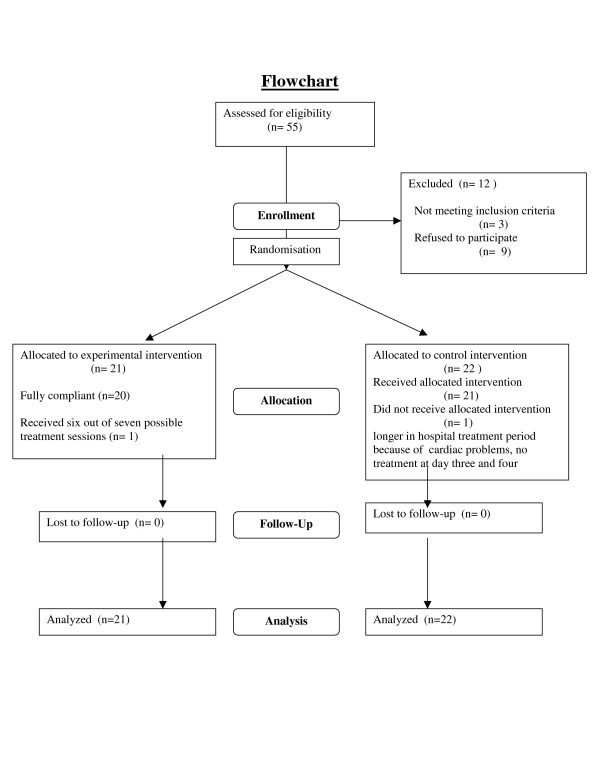
Flow chart of subjects through the trial.
Acknowledgments
Acknowledgements
We thank all our co workers of the Orthopaedic and Physical therapy department for their support during the trial. We thank all the patients who participated in the study for their valuable input.
Contributor Information
Anton F Lenssen, Email: alen@pmzl.azm.nl.
Yvonne HF Crijns, Email: Ycrij@pmzl.azm.nl.
Eddie MH Waltjé, Email: ewal@pmzl.azm.nl.
Mike JA van Steyn, Email: Mst@sort.azm.nl.
Ruud JT Geesink, Email: RGE@sort.azm.nl.
Piet A van den Brandt, Email: pa.vandenBrandt@epid.unimaas.nl.
Rob A de Bie, Email: ra.debie@epid.unimaas.nl.
References
- Macario A, Horne M, Goodman S, Vitez T, Dexter F, Heinen R, Brown B. The effect of a perioperative clinical pathway for knee replacement surgery on hospital costs. Anesth Analg. 1998;86:978–984. doi: 10.1097/00000539-199805000-00012. [DOI] [PubMed] [Google Scholar]
- Pennington JM, Jones DP, McIntyre S. Clinical pathways in total knee arthroplasty: a New Zealand experience. J Orthop Surg (Hong Kong) 2003;11:166–173. doi: 10.1177/230949900301100211. [DOI] [PubMed] [Google Scholar]
- Mabrey JD, Toohey JS, Armstrong DA, Lavery L, Wammack LA. Clinical pathway management of total knee arthroplasty. Clin Orthop Relat Res. 1997:125–133. doi: 10.1097/00003086-199712000-00017. [DOI] [PubMed] [Google Scholar]
- Harlan K, Meiring A. Total knee arthroplasty clinical pathway. Hosp Case Manag. 1999;7:49–53. [PubMed] [Google Scholar]
- Healy WL, Iorio R, Ko J, Appleby D, Lemos DW. Impact of cost reduction programs on short-term patient outcome and hospital cost of total knee arthroplasty. J Bone Joint Surg Am. 2002;84-A:348–353. doi: 10.2106/00004623-200203000-00003. [DOI] [PubMed] [Google Scholar]
- Pearson S, Moraw I, Maddern GJ. Clinical pathway management of total knee arthroplasty: a retrospective comparative study. Aust N Z J Surg. 2000;70:351–354. doi: 10.1046/j.1440-1622.2000.01819.x. [DOI] [PubMed] [Google Scholar]
- Kim S, Losina E, Solomon DH, Wright J, Katz JN. Effectiveness of clinical pathways for total knee and total hip arthroplasty: literature review. J Arthroplasty. 2003;18:69–74. doi: 10.1054/arth.2003.50030. [DOI] [PubMed] [Google Scholar]
- Oldmeadow LB, McBurney H, Robertson VJ. Hospital stay and discharge outcomes after knee arthroplasty: implications for physiotherapy practice. Aust J Physiother. 2002;48:117–121. doi: 10.1016/s0004-9514(14)60205-1. [DOI] [PubMed] [Google Scholar]
- Bennett LA, Brearley SC, Hart JA, Bailey MJ. A comparison of 2 continuous passive motion protocols after total knee arthroplasty: a controlled and randomized study. J Arthroplasty. 2005;20:225–233. doi: 10.1016/j.arth.2004.08.009. [DOI] [PubMed] [Google Scholar]
- Davies DM, Johnston DW, Beaupre LA, Lier DA. Effect of adjunctive range-of-motion therapy after primary total knee arthroplasty on the use of health services after hospital discharge. Can J Surg. 2003;46:30–36. [PMC free article] [PubMed] [Google Scholar]
- Mauerhan DR, Mokris JG, Ly A, Kiebzak GM. Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty. 1998;13:896–900. doi: 10.1016/S0883-5403(98)90196-6. [DOI] [PubMed] [Google Scholar]
- Mokris JG, Smith SW, Anderson SE. Primary total knee arthroplasty using the Genesis Total Knee Arthroplasty System: 3- to 6-year follow-up study of 105 knees. J Arthroplasty. 1997;12:91–98. doi: 10.1016/S0883-5403(97)90053-X. [DOI] [PubMed] [Google Scholar]
- Roos EM. Effectiveness and practice variation of rehabilitation after joint replacement. Curr Opin Rheumatol. 2003;15:160–162. doi: 10.1097/00002281-200303000-00014. [DOI] [PubMed] [Google Scholar]
- Jong de JA. Reactivatie van een THA patient volgens een óud'of een 'nieuw'protocol. MSc thesis, Maastricht University, Faculty of Health Sciences. 1999.
- http://www.azm.nl/professionals/overige+afdelingen/overzicht+overige+afdelingen/fysiotherapie/onderzoek/treatmentprotocoltkpshortenglish.pdf
- Bullens PH, van Loon CJ, de Waal Malefijt MC, Laan RF, Veth RP. Patient satisfaction after total knee arthroplasty: a comparison between subjective and objective outcome assessments. J Arthroplasty. 2001;16:740–747. doi: 10.1054/arth.2001.23922. [DOI] [PubMed] [Google Scholar]
- Brosseau L, Balmer S, Tousignant M, O'Sullivan JP, Goudreault C, Goudreault M, Gringras S. Intra- and intertester reliability and criterion validity of the parallelogram and universal goniometers for measuring maximum active knee flexion and extension of patients with knee restrictions. Arch Phys Med Rehabil. 2001;82:396–402. doi: 10.1053/apmr.2001.19250. [DOI] [PubMed] [Google Scholar]
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stit LW. Validation study of the WOMAC: a health status instrument for measuring clinically important patient relevant outcomes following total hip or knee arthroplasties in osteoarthritis. J Orthop Rheumatology. 1988;1:95–108. [PubMed] [Google Scholar]
- Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989:13–14. [PubMed] [Google Scholar]
- Roorda LD, Jones CA, Waltz M, Lankhorst GJ, Bouter LM, van der Eijken JW, Willems WJ, Heyligers IC, Voaklander DC, Kelly KD, Suarez-Almazor ME. Satisfactory cross cultural equivalence of the Dutch WOMAC in patients with hip osteoarthritis waiting for arthroplasty. Ann Rheum Dis. 2004;63:36–42. doi: 10.1136/ard.2002.001784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bach CM, Nogler M, Steingruber IE, Ogon M, Wimmer C, Gobel G, Krismer M. Scoring systems in total knee arthroplasty. Clin Orthop Relat Res. 2002:184–196. doi: 10.1097/00003086-200206000-00022. [DOI] [PubMed] [Google Scholar]
- Lingard EA, Katz JN, Wright RJ, Wright EA, Sledge CB. Validity and responsiveness of the Knee Society Clinical Rating System in comparison with the SF-36 and WOMAC. J Bone Joint Surg Am. 2001;83-A:1856–1864. doi: 10.2106/00004623-200112000-00014. [DOI] [PubMed] [Google Scholar]
- Guyatt GH, Townsend M, Berman LB, Keller JL. A comparison of Likert and visual analogue scales for measuring change in function. J Chronic Dis. 1987;40:1129–1133. doi: 10.1016/0021-9681(87)90080-4. [DOI] [PubMed] [Google Scholar]
- Norusis MJ. SPSS 9.0 guide tot data analyses. Chicago: SPSS Inc.1999
- Beaupre LA, Davies DM, Jones CA, Cinats JG. Exercise combined with continuous passive motion or slider board therapy compared with exercise only: a randomized controlled trial of patients following total knee arthroplasty. Phys Ther. 2001;81:1029–1037. [PubMed] [Google Scholar]
- Kumar PJ, McPherson EJ, Dorr LD, Wan Z, Baldwin K. Rehabilitation after total knee arthroplasty: a comparison of 2 rehabilitation techniques. Clin Orthop Relat Res. 1996:93–101. doi: 10.1097/00003086-199610000-00013. [DOI] [PubMed] [Google Scholar]
- MacDonald SJ, Bourne RB, Rorabeck CH, McCalden RW, Kramer J, Vaz M. Prospective randomized clinical trial of continuous passive motion after total knee arthroplasty. Clin Orthop Relat Res. 2000:30–35. doi: 10.1097/00003086-200011000-00005. [DOI] [PubMed] [Google Scholar]
- Bland JM. Cluster randomised trials in the medical literature: two bibliometric surveys. BMC Med Res Methodol. 2004;4:21. doi: 10.1186/1471-2288-4-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell MK, Elbourne DR, Altman DG. CONSORT statement: extension to cluster randomised trials. Bmj. 2004;328:702–708. doi: 10.1136/bmj.328.7441.702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lenssen AF, Bie de RA, Bulstra SK, Steijn van MJA. Continuous passive motion in rehabilitation following total knee arthroplasty: a Randomised controlled trial. Physical Therapy Reviews. 2003;8:123–129. doi: 10.1179/108331903225003019. [DOI] [Google Scholar]