

Abstract
Objectives. We compared the prevalence of risk factors for Black and White suicide decedents in Fulton County, Georgia, from 1988–2002.
Methods. We used data from the Fulton County Medical Examiner’s Office to compile information on suicides that occurred in Fulton County between 1988 and 2002. We used the χ2 test and logistic regression to identify associations between suicide risk factors and race.
Results. Black suicide decedents were more likely than White suicide decedents to be male (odds ratio [OR]=2.06; 95% confidence interval [CI]=1.38, 3.09), to be younger, (≤24 y [OR = 4.74; 95% CI = 2.88, 7.81]; 25–34 y [OR = 2.79; 95% CI = 1.74, 4.47]; 35–44 y [OR = 1.86; 95% CI = 1.13, 3.07]), and to hurt others in a suicide (OR = 4.22; 95% CI = 1.60, 11.15) but less likely to report depression (OR=0.63; 95% CI=0.48, 0.83), to have a family history of suicide (OR=0.08; 95% CI=0.01, 0.61), or to leave a suicide note (OR=0.37; 95% CI=0.26, 0.52).
Conclusions. Future research should consider that Black suicide decedents are less likely to report depression than White suicide decedents. This suicide risk difference is important when developing effective suicide prevention programs.
Between 2001 and 2002, suicide was the 11th leading cause of death in the United States, with more than 30000 fatalities per year.1–3 Because suicide rates are higher among Whites than among Blacks, research on suicide risk factors has primarily been focused on White decedents.1,4,5 However, suicide among Blacks is an important problem. Suicides among young Blacks has been increasing.6–9 Among Blacks aged 15–24 years in the United States, the age-specific suicide rates were 49% higher in 1995 than in 1981 (10 vs 6.7 per 100 000), whereas the rate for Whites in the same age group was 5% higher (13.7 vs 13.1 per 100 000).10 With a substantial proportion of the Black population aged younger than 24 years, the high suicide rates affecting the younger generation might have future repercussions for the Black population, both economically and sociologically.11–12
The recent rise in suicide rates among young Blacks has prompted researchers to reevaluate whether risk factors among White suicide decedents are relevant predictors of suicides among Blacks. Studies have identified several suicide risk factors among Blacks. These factors include male gender,1,6–8,11 young age,1,6–9 mental health service use,13 substance abuse,14,15 firearm availability,8,14,16 geographic residence (i.e., Northeast),9,11,14 higher economic status,17 and threatening behavior toward others.14,18 These risk factors also apply to Whites, with the exception of young age, geographic residence, and higher economic status.1,6,7,13 For Blacks, however, these findings are from a limited number of studies that are often hindered by small sample sizes.1,6,7,14
The substantial proportion of Blacks in the Fulton County, Georgia, population provides an opportunity to study differences between Black and White suicide decedents. In 2000, a total of 12% of the US population was Black and 75% was White. In Fulton County, Georgia, 45% of the population was Black and 48% of the population was White.19 The Fulton County Medical Examiner’s Office (FCMEO) collects demographic information on all persons who commit suicide in Fulton County, as well as information on the circumstances surrounding the suicides. Our examination of the FCMEO database to identify characteristics of suicide associated with race between 1988 and 2002 makes this study one of the largest population-based studies of Black and White suicide decedents.
METHODS
Data Collection
We used information in the FCMEO database to study suicide decedents and the characteristics of their suicides between 1988 and 2002. In Fulton County, injury-related deaths, sudden deaths, and deaths of persons who are not under the care of a physician are reported to FCMEO. For each decedent, a standardized form is completed by an FCMEO investigator and includes information on the circumstances surrounding the death (characteristics of suicide) based on interviews with family or friends of the decedent. All FCMEO investigators use the form; however, the method by which the information is collected from family and friends is at the discretion of the investigator. The form lists several presumptive contributing causes for suicide (i.e., grief, depression, money problems, legal problems, relationship problems, loneliness, family history, and current psychiatric care) and several behaviors or characteristics related to the suicide itself (i.e., suicide committed at home, a suicide note left, injury to others during the suicide, previous talk or gestures of suicide). The investigator marks those that are reported by the decedent’s family to apply to the decedent or event; no time frames for these behaviors or characteristics are specified in the form. The decedent’s medical history (i.e., heart disease, myocardial infarction, hypertension, emphysema, asthma, diabetes, seizures, chronic ethanol abuse, dementia, Alzheimer disease, strokes, renal disease, terminal illness, cancer, metastatic cancer, and drug abuse) is also coded separately by investigators. The cause, date, time of death, and manner of death of the decedent is determined by the medical examiner. A suicide determination is based on an approach developed by the National Association of Medical Examiners described in 2 previous publications, “Operational Criteria for the Determination of Suicide” and the Guide for Manner of Death Classification.20–21
Analysis
For analyses, we identified suicide decedents from the standardized forms that were marked as suicide under “manner of death.” We classified deaths as firearm suicides if a firearm was noted in the field “describe how injury occurred.” We collapsed the codes for ethanol abuse and drug abuse into 1 category for substance abuse and all other medical conditions into 1 category for chronic disease.
We used χ2 tests to evaluate the associations between the characteristics of suicide and race. Crude odds ratios (OR) were calculated by using SAS version 9.1 (SAS Institute Inc., Cary, NC). Variables associated with race in the univariate analysis were put into a logistic regression model to determine independent associations between the characteristics of suicide decedents and decedent’s race. The statistical significance of interaction terms for age, gender, depression and suicide note was determined through use of the “chunk” test.22
We calculated age-specific suicide rates per 100000 population among Blacks and Whites in Fulton County by using the 1990 US Census population (bridged) as the denominator for suicides that occurred between 1988 and 1992, the 1995 US Census estimates (bridged) as the denominator for suicides that occurred during between 1993 and 1997, and the 2000 US Census population as the denominator for suicides that occurred between 1998 and 2002. We age adjusted suicide rates by using the 2000 US standard population.
RESULTS
Suicide Rates
Between 1988 and 2002, a total of 1300 persons who had committed suicide were reported to the FCMEO, including 862 (66%) Whites, 399 (31%) Blacks, and 39 (3%) persons of another race. Of the 1261 Black and White suicide decedents, 80% were male and 59% were aged ≤44 years (Table 1 ▶). A higher percentage of Black suicide decedents (87%) than White suicide decedents (76%) were male. A higher percentage of Black suicide decedents (76%) than White suicide decedents (52%) were aged ≤44 years. Firearms accounted for 60% of the suicides and were the principal method of suicide among both Black (62%) and White (59%) decedents.
TABLE 1—
Characteristics of Black and White Suicide Decedents, Fulton County, Georgia (n = 1261), 1988–2002
| Characteristics | Total (N = 1261) No. (%) | Black (n = 399) No. (%) | White (n = 862) No. (%) |
| Gender | |||
| Male | 1008 (80) | 349 (87) | 659 (76) |
| Female | 253 (20) | 50 (13) | 203 (24) |
| Age, y | |||
| 0–14 | 9 (< 1) | 6 (< 2) | 3 (< 1) |
| 15–24 | 207 (16) | 110 (28) | 97 (11) |
| 25–34 | 298 (24) | 114 (29) | 184 (21) |
| 35–44 | 244 (19) | 75 (19) | 169 (20) |
| 45–64 | 303 (24) | 57 (14) | 246 (28) |
| ≥65 | 198 (16) | 36 (9) | 162 (19) |
| Unknown | 2 (< 1) | 1 (< 1) | 1 (< 1) |
| Firearm Use | 758 (60) | 246 (62) | 512 (59) |
Note. From this analysis, 39 suicide decedents with race other than White or Black were excluded.
During the 15-year period, age-adjusted suicide rates for both Blacks and Whites in Fulton County decreased (Figure 1 ▶). Suicide rates among Blacks were consistently lower than those among Whites. Suicide rates among Whites decreased 21% from 17.7 in the period 1988–1992 to 14.0 per 100 000 in the period 1998–2002, and suicide rates among Blacks decreased 30%, from 8.9 to 6.2 per 100 000 between 1988 and 2002. In addition, firearm suicide rates decreased approximately 25% for both Whites (from 10.7 to 8.0 per 100 000) and for Blacks (from 5.3 to 4.0 per 100 000). However, among persons aged 15–24 years, firearm suicide rates decreased 50% for Whites (from 10 to 5 per 100 000) but remained virtually unchanged (from 8 to 8 per 100 000) among Blacks during the 15-year study period.
FIGURE 1—
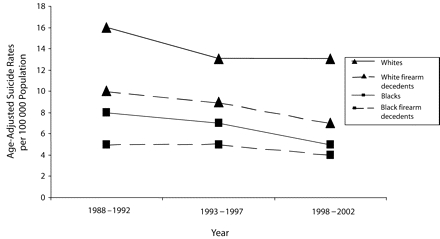
Age-adjusted suicide rates by race in Fulton County, Georgia, 1988–2002.
Data sources. Fulton County Medical Examiner Files (number of suicides) and US Census Bureau (population).
The difference in suicide rates between Blacks and Whites was substantially greater for older persons (aged 45–65 y) (Figure 2 ▶). Suicide rates among Blacks and Whites were similar among persons aged 15–24 years. Among Whites, suicide rates were highest in persons aged 65 years or older years. However, among Blacks, suicide rates were highest among persons aged 15–24 and 25–34 years.
FIGURE 2—
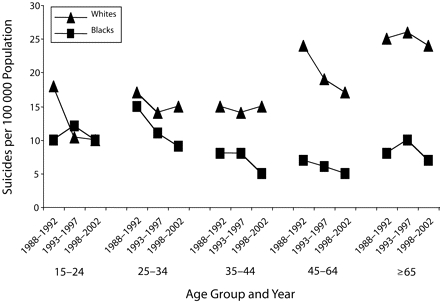
Age-adjusted suicide rates by race and age group in Fulton County, Georgia, 1988–2002.
Data sources. Fulton County Medical Examiner Files (number of suicides) and US Census Bureau (population).
Characteristics of Suicide Decedents
Of the 1261 Black and White suicide decedents, 1132 (90%) had complete information in the FCMEO database regarding the circumstances of suicide. Depression was the most frequently reported characteristic that might have contributed to the suicide (Table 2 ▶). Greater than half of the suicide decedents were reported to have suffered from depression (57%). Relationship problems were reported to be a contributing factor for 26% of the suicides. Of the suicide decedents, 68% were found at home, 29% of the suicide decedents were reported to have left a suicide note, and 27% were reported to have spoken about suicide before their death. Characteristics of suicide less frequently reported included grief (4%), a family history of suicide (2%), and hurting others during the suicide (2%).
TABLE 2—
Characteristics of Suicide, Fulton County, Georgia (n = 1132), 1988–2002
| Suicide characteristics | Total (N = 1132) No. (%) | Black (n = 348) No. (%) | White (n = 784) No. (%) | Pa |
| Contributing | ||||
| Depression | 642 (57) | 147 (42) | 495 (63) | < .0001 |
| Relationship problems | 292 (26) | 101 (29) | 191 (24) | .10 |
| Chronic disease | 192 (17) | 36 (10) | 156 (20) | < .0001 |
| Money problems | 184 (16) | 45 (13) | 139 (18) | .04 |
| Under psychiatric care | 134 (12) | 29 (8) | 105 (13) | .02 |
| Substance abuse | 128 (11) | 29 (8) | 99 (13) | .04 |
| Legal problems | 78 (7) | 24 (7) | 54 (7) | .99 |
| Loneliness | 64 (6) | 13 (4) | 51 (7) | .06 |
| Grief | 49 (4) | 13 (4) | 36 (5) | .51 |
| Family history of suicide | 28 (2) | 1 (< 1) | 27 (3) | .002 |
| Event associated | ||||
| At home | 772 (68) | 204 (58) | 568 (72) | < .0001 |
| Suicide note left | 331 (29) | 52 (15) | 279 (36) | < .0001 |
| Prior talk | 309 (27) | 74 (21) | 235 (30) | .002 |
| Prior gestures | 154 (14) | 34 (10) | 120 (15) | .01 |
| Others hurt during suicide | 25 (2) | 19 (6) | 6 (< 1) | < .0001 |
Note. Data were missing for 129 suicide decedents.
From this analysis, 39 suicide decedents with race other than White or Black were excluded.
a2-sided χ2 test
Black suicide decedents were less likely than White suicide decedents to experience depression and money problems; be under psychiatric care; and have a chronic disease, substance abuse problem, and a family history of suicide (Table 2 ▶). Black suicide decedents were also less likely than their White counterparts to be found at home, leave a suicide note, or to have talked or gestured about suicide; however, they were more likely to hurt others during a suicide.
Multivariate analysis indicated that Black suicide decedents were more likely than White suicide decedents to be male, to be young, and to hurt others in a suicide; however, they were less likely to be reported to have a history of depression, a family history of suicide, or to leave a suicide note (Table 3 ▶). Interaction terms were not significantly associated with race.
TABLE 3—
Characteristics Independently Associated with Black Suicide Decedents, Fulton County, Georgia (n= 1130), 1988–2002
| Characteristics | AOR | 95% CI |
| Male | 2.06 | (1.38, 3.09) |
| Age, y | ||
| < 24 | 4.74 | (2.88, 7.81) |
| 25–34 | 2.79 | (1.74, 4.47) |
| 35–44 | 1.86 | (1.13, 3.07) |
| 45–64 | 1.24 | (0.75, 2.05) |
| ≥65 | reference | |
| Depression | 0.63 | (0.48, 0.83) |
| Family history of suicide | 0.08 | (0.01, 0.61) |
| Suicide note left | 0.37 | (0.26, 0.52) |
| Others hurt during suicide | 4.22 | (1.60, 11.15) |
Note. AOR= adjusted odds ratio; CI=confidence interval.
DISCUSSION
The age-adjusted suicide rate trends between 1988 and 2002 observed in Fulton County, Georgia, were consistent with national data during the same time period.1,22 Furthermore, by 2002, in Fulton County and in the United States, age-specific suicide rates for young Black suicide decedents were as high as rates among young White suicide decedents. As in other suicide studies, Black suicide decedents in Fulton County were more likely to be young and male compared with their White counterparts.6,7,9,22 Information from family and friends of the suicide decedent also indicate that Black and White suicide decedents have different suicide risk factors. Black suicide decedents were more likely than White suicide decedents to injure others at the time of their suicide, but the former were less likely to be reported as having depression, as having a family history of suicide, or as leaving a suicide note. Similar to our study, one recent national study also showed that Black suicide decedents report fewer symptoms of depression before their deaths than White suicide decedents.24 Such racial differences have important implications for prevention efforts. School counselors and mental health professionals should be aware of the lack of tell-tale suicide signs and should not assume a lower risk of suicide if these risk factors are not apparent among Blacks.
These findings are important, because current risk factors for suicide have been identified mainly from studies involving predominantly White suicide decedents.1,4 Studies of suicides among Blacks lack generalizability since many of the studies have been restricted by limited sample populations.6,14,25 Other studies of suicides among Blacks have focused on populations of suicide attempters rather than suicide completers.26 Only a few studies have reported suicide risk factors among Black and White suicide decedents by using a nationally representative study population.13,14,18 One of the strengths of our study is that we had a greater proportion of Black suicide decedents than other similar studies. Furthermore, Garlow15 demonstrated that suicide decedents in Fulton County, Georgia, (1994–1999) were similar to the national sample of suicide decedents in the 1986 and 1993 National Mortality Follow-back Survey (NMFS).13,18,24
Several studies suggest that, because of culture or spiritual beliefs, stronger negative perceptions exist toward suicide or suicide risk factors among Blacks compared with Whites, which can potentially lead to underreporting of both suicide and suicide risk factors.6,27,28 Misclassification of suicides has been reported to occur more frequently among minorities.29 Studies also have suggested that Blacks, in particular, regard suicide as a dishonorable act and therefore might misreport a suicide as another type of injury-related death (e.g., homicide, unintentional death) to avoid the stigma of suicide.28,30,31 The FCMEO follows a standard procedure for determining suicide as the cause of death that should minimize racial bias.
The lower odds ratios we observed for depression among Black suicide decedents might be strongly influenced by negative cultural perceptions toward depression that exist within the Black community.32 These negative perceptions toward depression might directly influence access to or utilization of medical or psychiatric care, family support, awareness of depression by family or decedent, or a combination of these.6,13,31 Although depression and other mental illnesses have been less well studied among Blacks than among Whites,1,33,34 the available evidence supports that Blacks, in general, have a lower lifetime estimated prevalence of major depression after confounders are controlled.33–35 Whether Blacks are truly less depressed compared with Whites or whether the lower prevalence is a result of the underreporting caused by cultural stigmas associated with depression remains a significant question to be studied.
Our analysis had certain limitations. The information on characteristics of suicide was collected from family members or friends and was not verified by medical records or diagnostic testing. Although all FCMEO investigators undergo training on how to complete a case form, the method by which the suicide information is collected is at the discretion of the FCMEO investigator. Underreporting characteristics of the suicide might occur if the investigator does not ask or if a family member or friend does not mention a specific characteristic of the suicide. Finally, our suicide rates are not “true” rates because the numerator represents the number of suicides that occurred in Fulton County and the denominator represents residents of Fulton County. Data available from 1998 through 2002 indicate that suicide rates calculated from the FCMEO database were lower than those calculated by using number of suicides by Fulton County residents (6.2 per 100000 compared with 6.4 per 100000 for Blacks and 14 per 100000 compared with 16.9 per 100000 for Whites, respectively). This discrepancy suggests White residents of Fulton County might be more likely to commit suicide in another county.
Our study examined a unique set of suicide characteristics among Fulton County suicide decedents by race, using the large Black population in Fulton County. Identification of Black individuals at high risk for suicide would appear to be more difficult than identification of White individuals because the most common contributing factor, depression, was significantly more commonly reported among White suicide decedents. Therefore, prevention efforts may need to place relatively greater emphasis on communitywide activities to establish supportive environments and build coping skills. Both Blacks and Whites also may benefit from safer firearm storage practices in households that choose to have a firearm, because use of firearms was the principal method in more than 50% of suicides by Blacks and Whites. Future years will determine whether the suicide rates and the predominant risk factors for Black and White youth have converged.36 Will the suicide rates among this cohort of Black youth follow the upward trend of White suicide rates or will the suicide rates decrease as observed among older Blacks as these youth age? Will the reporting of predominant risk factors for suicide (e.g., depression) also increase among Blacks over time if a continued upward suicide trend occurs similar to that of Whites? Further research is necessary to identify whether the converging of the suicide rates results in the convergence of suicide risk factors among Blacks and Whites. Such studies should provide useful information when developing the appropriate suicide prevention programs targeted to both Blacks and Whites.
Acknowledgments
We thank David Callahan MD, Walter Daley, DVM, MPH, and Anindya De, PhD for their thoughtful comments on the article.
Human Participant Protection No protocol approval was needed for this study.
Peer Reviewed
Contributors K. Abe, K. Mertz, and K. Powell conceived and designed the study. K. Abe performed the data analysis and led the writing of this article. K. Mertz and K. Powell conceptualized ideas, participated in the writing, and supervised data analysis. R. Hanzlick compiled the data, maintained the database, outlined the methodology, and was available for consultation. All the authors helped formulate ideas, interpret findings, and reviewed drafts of the article.
References
- 1.Goldsmith SK. Reducing Suicide: A National Imperative. Washington, DC: The National Academies Press; 2002. Available at: http://books.nap.edu/books/0309083214/html. Accessed October 14, 2005. [PubMed]
- 2.Arias E, Anderson RN, Kung HC, Murphy SL, Kochanek KD. Deaths: final data for 2001. Natl Vital Stat Rep. 2003;52:1–115. [PubMed] [Google Scholar]
- 3.Kochanek KD, Murphy SL, Anderson RN, Scott C. Deaths: final data for 2002. Natl Vital Stat Rep. 2004; 53:1–115. [PubMed] [Google Scholar]
- 4.Moscicki EK. Epidemiology of suicidal behavior. Suicide Life Threat Behav. 1995;25:22–35. [PubMed] [Google Scholar]
- 5.United States Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, Office of Analysis, Epidemiology, and Health Promotion, Compressed Mortality File [CDC-Wonder on-line database]. Available at: http://wonder.cdc.gov. Accessed May 11, 2005.
- 6.Gibbs JT. African-American suicide: a cultural paradox. Suicide Life Threat Behav. 1997;27:68–79. [PubMed] [Google Scholar]
- 7.Joe S, Kaplan MS. Suicide among African-American men. Suicide Life Threat Behav. 2001;31(Suppl): 106–121. [DOI] [PubMed] [Google Scholar]
- 8.Willis LA, Coombs DW, Cockerham WC, Frison SL, Garlow SJ. Ready to die: a postmodern interpretation of the increase of African-American adolescent male suicide. Soc Sci Med. 2002;55:907–920. [DOI] [PubMed] [Google Scholar]
- 9.Centers for Disease Control and Prevention. Suicide among Black youths—United States, 1980–1995. MMWR Morb Mortal Wkly Rep. 1998;47:193–196. [PubMed] [Google Scholar]
- 10.United States Department of Health and Human Services, Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. [WISQARS online database]. Available at: http://webappa.cdc.gov/sasweb/ncipc/mortrate.html. Accessed January 10, 2005.
- 11.Davis R. Black suicide in the seventies: current trends. Suicide Life Threat Behav. 1979;9:131–140. [PubMed] [Google Scholar]
- 12.US Bureau of the Census, 2003. Table 4: Annual Estimates of the Population by Sex and Age of Black or African-American Alone for the United States: April 1, 2000 to July 1, 2003 (NC-EST2003–04-03) Release date: June 14, 2004. Available at: http://www.census.gov. Accessed October 14, 2005.
- 13.Kung KC, Liu X, Juon HS. Risk factors for suicide in Caucasians and in African Americans: a matched case-control study. Soc Psychiatry Psychiatr Epidemiol. 1998;33:155–161. [DOI] [PubMed] [Google Scholar]
- 14.Willis LA, Coombs DW, Drentea P, Cockerham WC. Uncovering the mystery: factors of African-American suicide. Suicide Life Threat Behav. 2003;33:412–429. [DOI] [PubMed] [Google Scholar]
- 15.Garlow SJ. Age, gender, and ethnicity differences in patterns of cocaine and ethanol use preceding suicide. Am J Psychiatry. 2002;159:615–619. [DOI] [PubMed] [Google Scholar]
- 16.Kaplan MS, Geling O. Firearm suicides and homicides in the United States: regional variations and patterns of gun ownership. Soc Sci Med. 1998;46: 1227–1233. [DOI] [PubMed] [Google Scholar]
- 17.Burr JH, JT Matteson DW. Black suicide in US metropolitan areas: an examination of the racial inequality and social integration regulation hypotheses. Social Forces. 1999;77:1049–1081. [Google Scholar]
- 18.Castle K, Duberstein PR, Meldrum S, Conner KR, Conwell Y. Risk factors for suicide in Blacks and Whites: an analysis of data from the 1993 National Mortality Followback Survey. Am J Psychiatry. 2004; 161:452–458. [DOI] [PubMed] [Google Scholar]
- 19.US Census Bureau, 2000 Census; ePodunk. Available at: http://www.epodunk.com/cgi-bin/popInfo/php?locIndex=7956 Accessed January 10, 2005.
- 20.Rosenberg ML, Davidson LE, Smith JC, et al. Operational criteria for the determination of suicide. J Forensic Sci. 1988;33:1445–56. [PubMed] [Google Scholar]
- 21.Hanzlick R, Hunsaker JC, Davis GJ. Guide for Manner of Death Classification. National Association of Medical Examiners. Available at: http://www.charlydmiller.com/LIB03/2002NAMEmannerofdeath.pdf. Accessed July 10, 2006.
- 22.Kleinbaum D. Logistic regression: a self-learning text. Springer-Verlag TELOS, New York, NY: 1994.
- 23.Bingham CR, Bennion LD, Openshaw DK, Adams GR. An analysis of age, gender and racial differences in recent national trends of youth suicide. Adolesc. 1994;17:53–71. [Google Scholar]
- 24.Kung HC, Pearson JL, Wei R. Substance use, firearm availability, depressive symptoms, and mental health service utilization among White and African American suicide decedents aged 15 to 64 years. Ann Epidemiol. 2005;15:614–621. [DOI] [PubMed] [Google Scholar]
- 25.Joe S, Marcus SC. Datapoints: trends by race and gender in suicide attempts among US adolescents, 1991–2001. Psychiatr Serv. 2003;54:454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Roy A. African-American and Caucasian attempters compared for suicide risk factors: a preliminary study. Suicide Life Threat Behav. 2003;33: 443–447. [DOI] [PubMed] [Google Scholar]
- 27.Early K. Religion and Suicide in the African-American Community. Westport, Conn: Greenwood Press; 1992.
- 28.Gibbs JT. Conceptual, methodological, and socio-cultural issues in Black youth suicide: implications for assessment and early intervention. Suicide Life Threat Behav. 1988;18:73–89. [DOI] [PubMed] [Google Scholar]
- 29.Sorenson SB, Shen H. Youth suicide trends in California: an examination of immigrant and ethnic group risk. Suicide Life Threat Behav. 1996;26:143–154. [PubMed] [Google Scholar]
- 30.Peck D. Official documentation of the Black suicide experience. Omega. 1983;14:21–31. [Google Scholar]
- 31.Wyche K, Rotheram-Borus M. Suicide Behavior Among Minority Youth in the United States. Newbury Park, Calif: Sage; 1990.
- 32.National Mental Health Association. Depression and African-Americans Fact Sheet. Alexandria, Va: National Mental Health Association; 2000.
- 33.Kessler RC, McGonagle KA, Zhao S. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8–19. [DOI] [PubMed] [Google Scholar]
- 34.Dunlop DD, Song J, Lyons JS, Manheim LM, Chang RW. Racial/ethnic differences in rates of depression among preretirement adults. Am J Public Health. 2003;93:1945–1952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Blazer DG, Kessler RC, McGonagle KA, Swartz MS. The prevalence and distribution of major depression in a national community sample: the National Comorbidity Survey. Am J Psychiatry. 1994;151:979–986. [DOI] [PubMed] [Google Scholar]
- 36.Prudhomme C. The problem of suicide in the American Negro. Psychoanal Rev. 1938;25:187–204, 372–391. [Google Scholar]