

Abstract
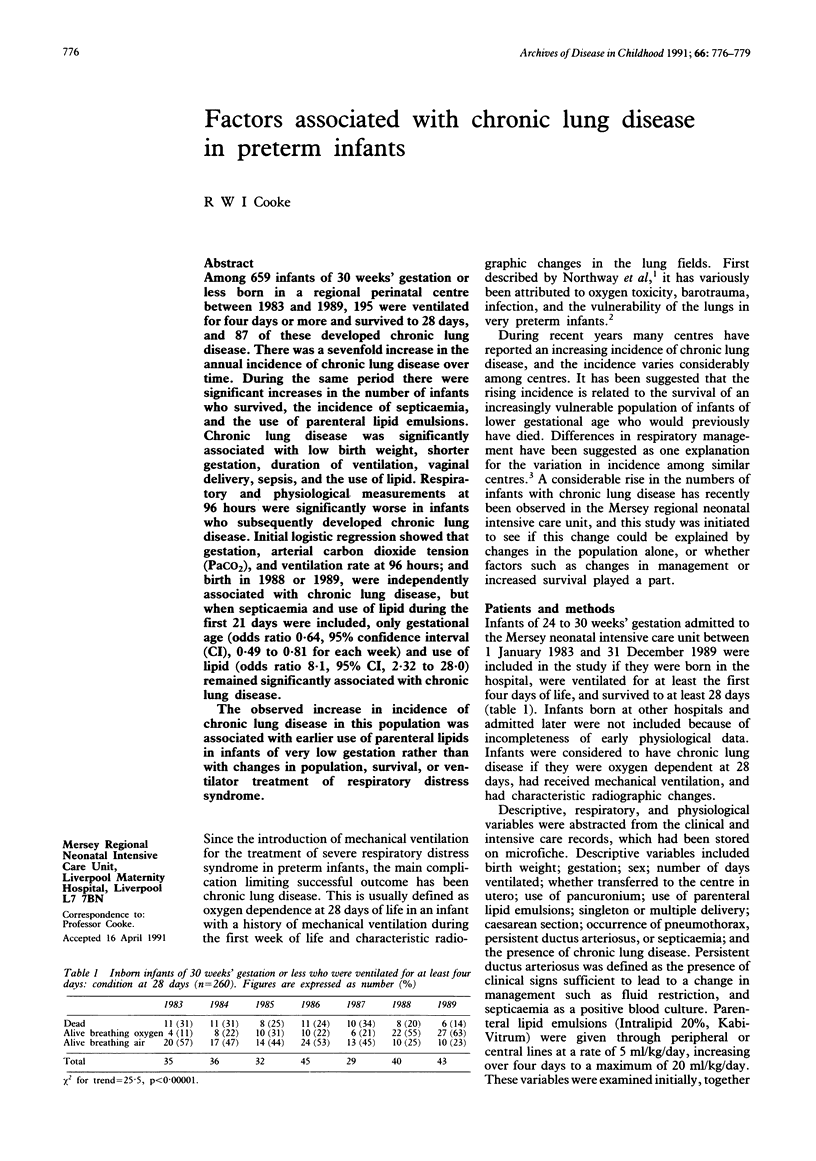
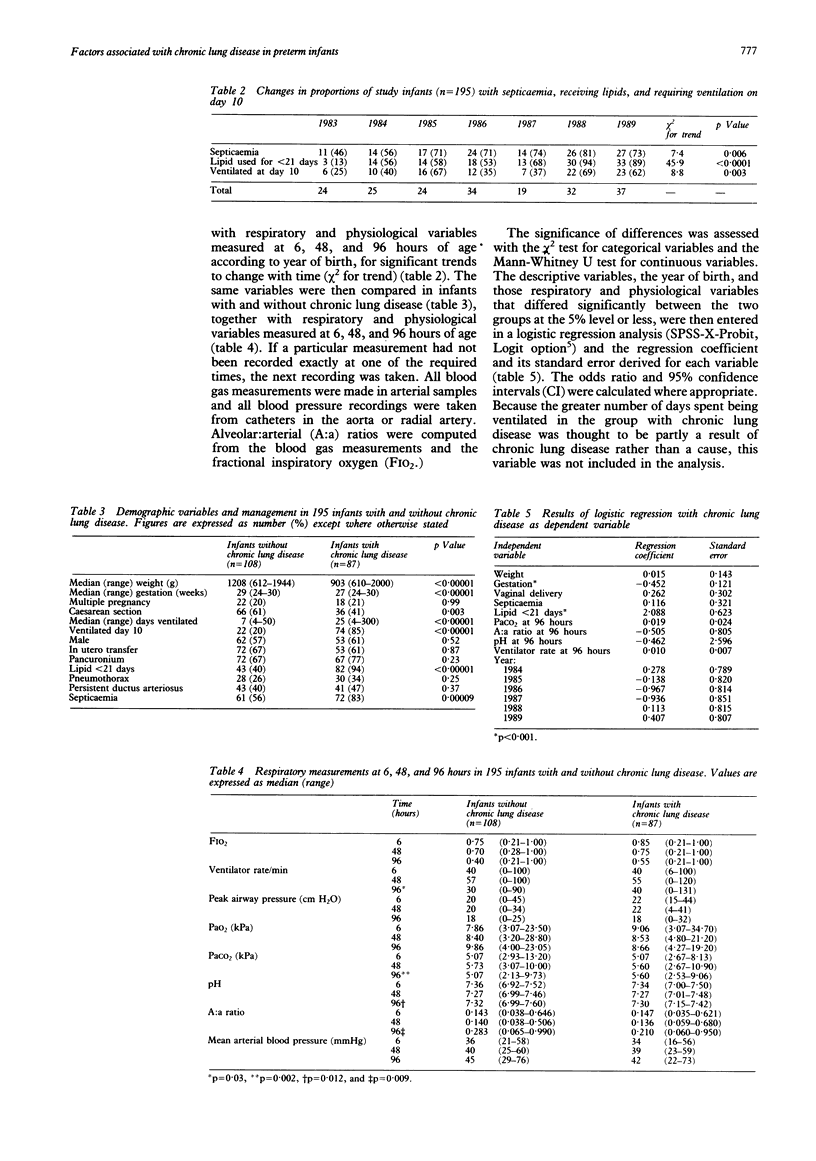
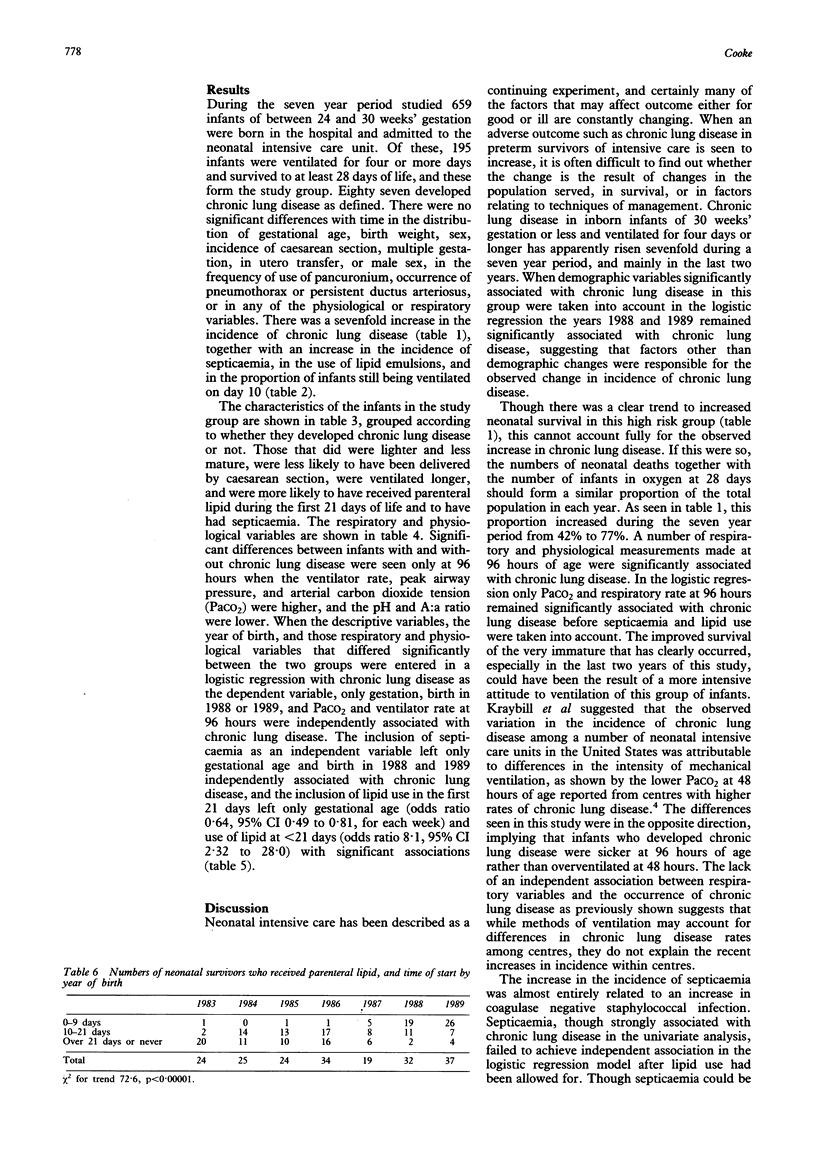
Among 659 infants of 30 weeks' gestation or less born in a regional perinatal centre between 1983 and 1989, 195 were ventilated for four days or more and survived to 28 days, and 87 of these developed chronic lung disease. There was a sevenfold increase in the annual incidence of chronic lung disease over time. During the same period there were significant increases in the number of infants who survived, the incidence of septicaemia, and the use of parenteral lipid emulsions. Chronic lung disease was significantly associated with low birth weight, shorter gestation, duration of ventilation, vaginal delivery, sepsis, and the use of lipid. Respiratory and physiological measurements at 96 hours were significantly worse in infants who subsequently developed chronic lung disease. Initial logistic regression showed that gestation, arterial carbon dioxide tension (PaCO2), and ventilation rate at 96 hours; and birth in 1988 or 1989, were independently associated with chronic lung disease, but when septicaemia and use of lipid during the first 21 days were included, only gestational age (odds ratio 0.64, 95% confidence interval (CI), 0.49 to 0.81 for each week) and use of lipid (odds ratio 8.1, 95% CI, 2.32 to 28.0) remained significantly associated with chronic lung disease. The observed increase in incidence of chronic lung disease in this population was associated with earlier use of parenteral lipids in infants of very low gestation rather than with changes in population, survival, or ventilator treatment of respiratory distress syndrome.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Avery M. E., Tooley W. H., Keller J. B., Hurd S. S., Bryan M. H., Cotton R. B., Epstein M. F., Fitzhardinge P. M., Hansen C. B., Hansen T. N. Is chronic lung disease in low birth weight infants preventable? A survey of eight centers. Pediatrics. 1987 Jan;79(1):26–30. [PubMed] [Google Scholar]
- Freeman J., Goldmann D. A., Smith N. E., Sidebottom D. G., Epstein M. F., Platt R. Association of intravenous lipid emulsion and coagulase-negative staphylococcal bacteremia in neonatal intensive care units. N Engl J Med. 1990 Aug 2;323(5):301–308. doi: 10.1056/NEJM199008023230504. [DOI] [PubMed] [Google Scholar]
- Hammerman C., Aramburo M. J. Decreased lipid intake reduces morbidity in sick premature neonates. J Pediatr. 1988 Dec;113(6):1083–1088. doi: 10.1016/s0022-3476(88)80587-0. [DOI] [PubMed] [Google Scholar]
- Kraybill E. N., Runyan D. K., Bose C. L., Khan J. H. Risk factors for chronic lung disease in infants with birth weights of 751 to 1000 grams. J Pediatr. 1989 Jul;115(1):115–120. doi: 10.1016/s0022-3476(89)80345-2. [DOI] [PubMed] [Google Scholar]
- Northway W. H., Jr, Rosan R. C., Porter D. Y. Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N Engl J Med. 1967 Feb 16;276(7):357–368. doi: 10.1056/NEJM196702162760701. [DOI] [PubMed] [Google Scholar]
- Periera G. R., Fox W. W., Stanley C. A., Baker L., Schwartz J. G. Decreased oxygenation and hyperlipemia during intravenous fat infusions in premature infants. Pediatrics. 1980 Jul;66(1):26–30. [PubMed] [Google Scholar]
- Saugstad O. D. Hypoxanthine as an indicator of hypoxia: its role in health and disease through free radical production. Pediatr Res. 1988 Feb;23(2):143–150. doi: 10.1203/00006450-198802000-00001. [DOI] [PubMed] [Google Scholar]