

Abstract
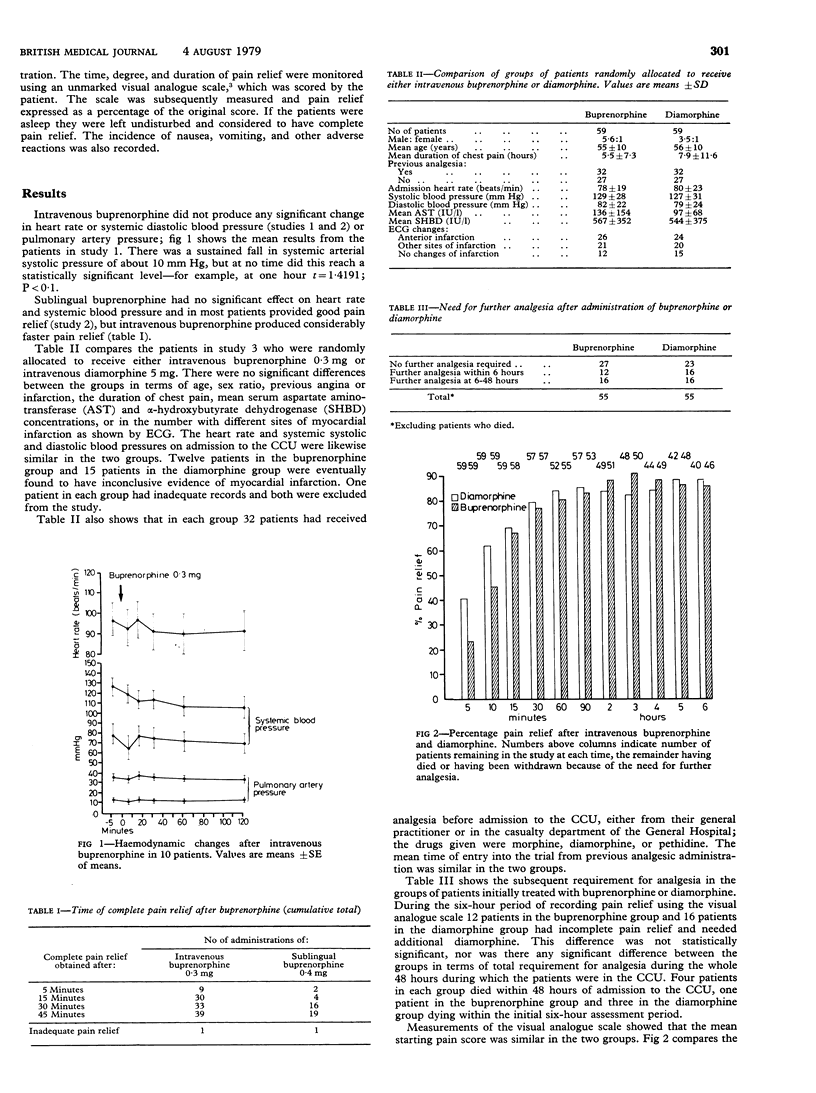
Buprenorphine, a new powerful analgesic agent, was used to treat chest pain in patients with suspected myocardial infarction. Initial studies showed no significant changes in systemic or pulmonary artery blood pressure or in heart rate after intravenous buprenorphine. Sublingual buprenorphine also appeared effective in relieving pain, but its onset of action was considerably delayed compared with the intravenous route. A randomised double-blind controlled trial of equivalent doses of buprenorphine and diamorphine showed no significant difference between the drugs in terms of pain relief and duration of action. The occurrence of nausea, vomiting, and other side effects was similar in the two groups. The onset of action of buprenorphine was slightly but significantly slower than that of diamorphine. Since buprenorphine seems to be comparable with diamorphine in action and is not a controlled drug, it may prove useful in both general and hospital practice.
Full text
PDF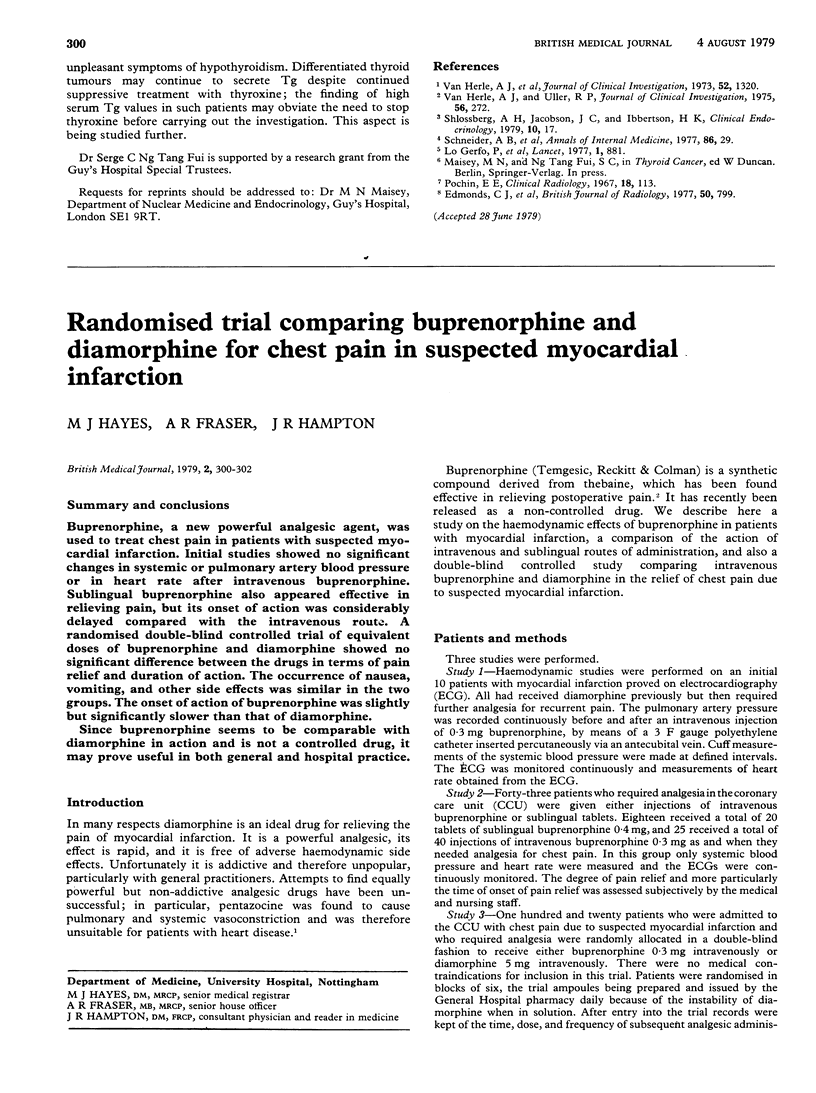

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Hovell B. C. Comparison of buprenorphine, pethidine and pentazocine for the relief of pain after operation. Br J Anaesth. 1977 Sep;49(9):913–916. doi: 10.1093/bja/49.9.913. [DOI] [PubMed] [Google Scholar]
- Huskisson E. C. Measurement of pain. Lancet. 1974 Nov 9;2(7889):1127–1131. doi: 10.1016/s0140-6736(74)90884-8. [DOI] [PubMed] [Google Scholar]
- Jewitt D. E., Maurer B. J., Hubner P. J. Increased pulmonary arterial pressures after pentazocine in myocardial infarction. Br Med J. 1970 Mar 28;1(5699):795–796. doi: 10.1136/bmj.1.5699.795. [DOI] [PMC free article] [PubMed] [Google Scholar]