

Abstract
A peak period of hyperglycaemia in insulin-dependent diabetics occurs after breakfast. A randomised crossover study was performed on nine diabetic children at home to study the effect of varying the time of their morning mixed injection of Monotard and Actrapid insulin on this hyperglycaemic peak. Performing the study at home minimised the children's stress.
After diabetic control had been improved children injected their insulin 30 minutes (early injection) or five minutes (late injection) before breakfast on two consecutive Saturday mornings. Blood samples were taken at 30-minute intervals over 3½ hours and analysed for concentrations of glucose, insulin, C-peptide, pyruvate, lactate, alanine, and ketones. Diet, insulin dose, and exercise were kept the same on both test days.
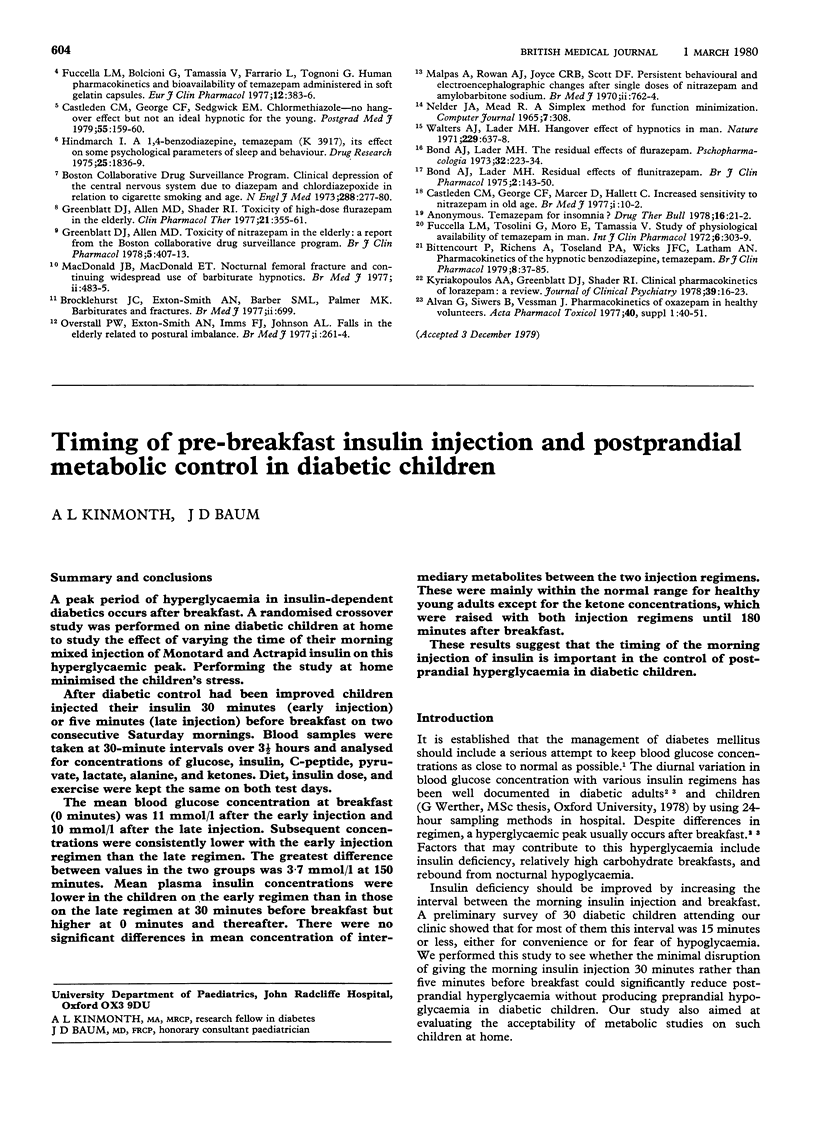
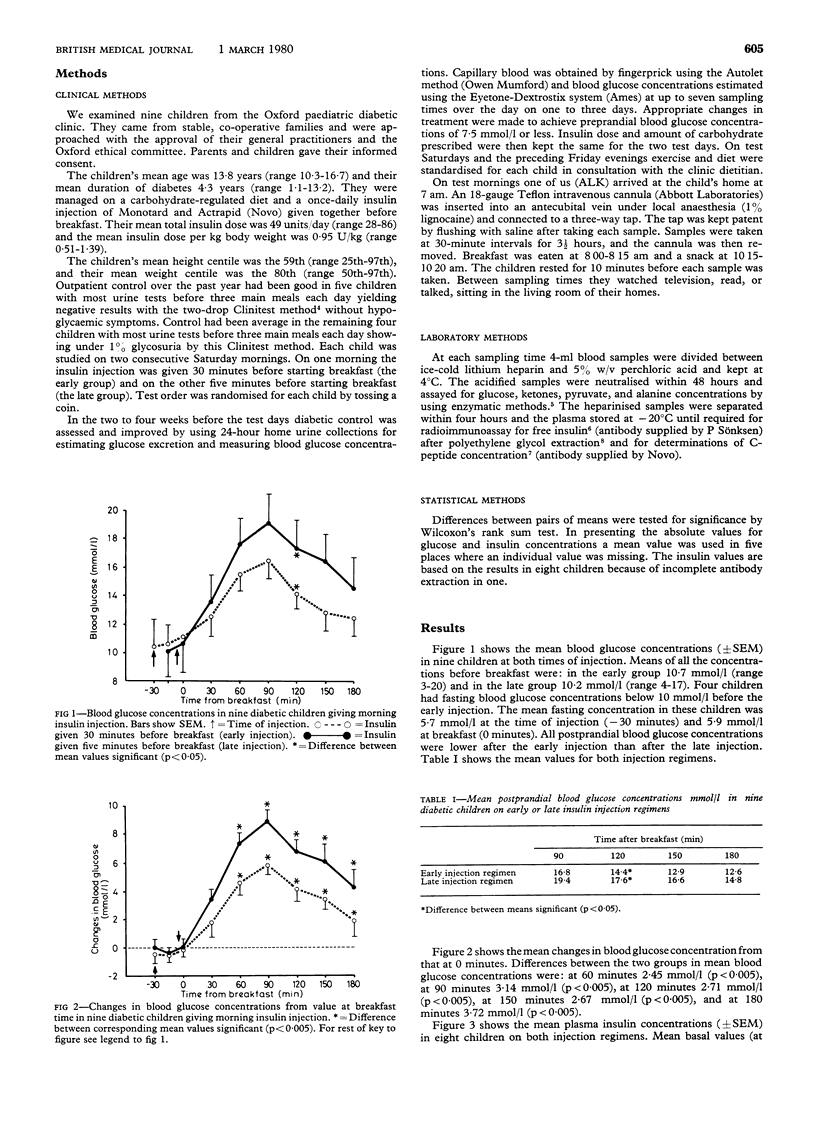
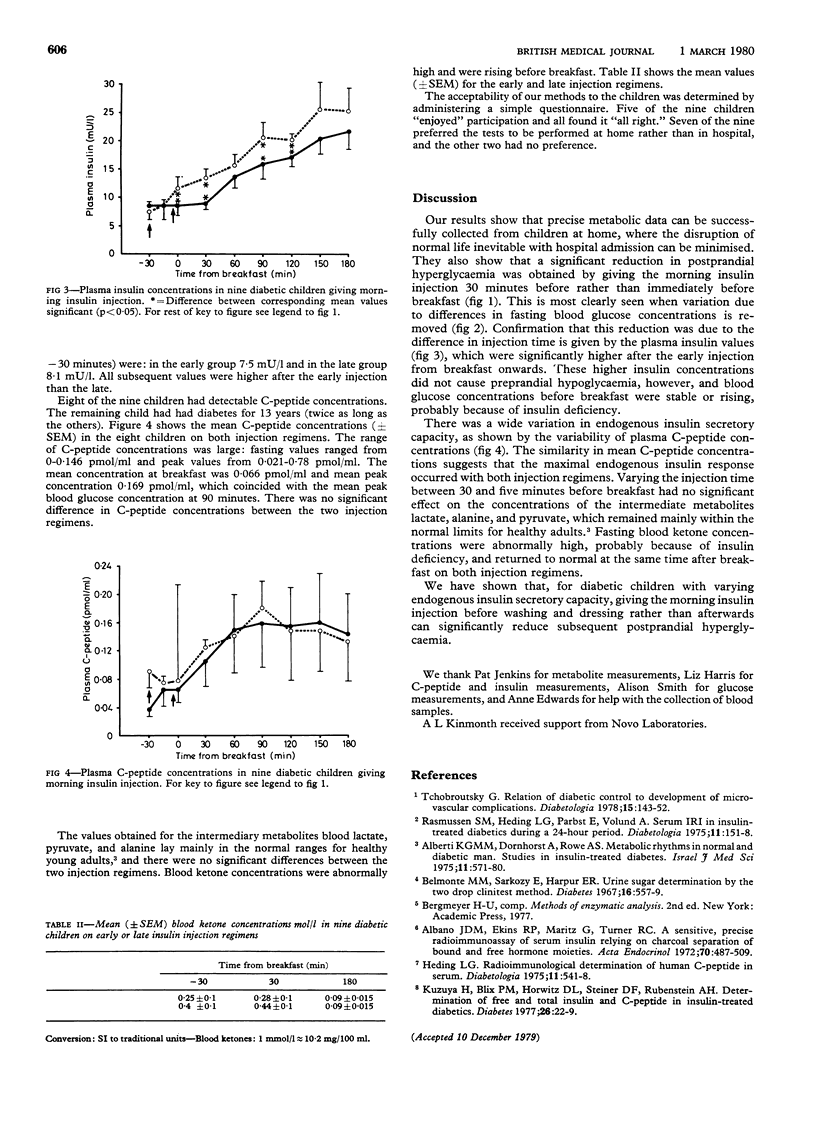
The mean blood glucose concentration at breakfast (0 minutes) was 11 mmol/l after the early injection and 10 mmol/l after the late injection. Subsequent concentrations were consistently lower with the early injection regimen than the late regimen. The greatest difference between values in the two groups was 3·7 mmol/l at 150 minutes. Mean plasma insulin concentrations were lower in the children on the early regimen than in those on the late regimen at 30 minutes before breakfast but higher at 0 minutes and thereafter. There were no significant differences in mean concentration of intermediary metabolites between the two injection regimens. These were mainly within the normal range for healthy young adults except for the ketone concentrations, which were raised with both injection regimens until 180 minutes after breakfast.
These results suggest that the timing of the morning injection of insulin is important in the control of postprandial hyperglycaemia in diabetic children.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Albano J. D., Ekins R. P., Maritz G., Turner R. C. A sensitive, precise radioimmunoassay of serum insulin relying on charcoal separation of bound and free hormone moieties. Acta Endocrinol (Copenh) 1972 Jul;70(3):487–509. doi: 10.1530/acta.0.0700487. [DOI] [PubMed] [Google Scholar]
- Alberti K. G., Dornhorst A., Rowe A. S. Metabolic rhythms in normal and diabetic man. Studies in insulin-treated diabetes. Isr J Med Sci. 1975 Jun;11(6):571–580. [PubMed] [Google Scholar]
- Heding L. G. Radioimmunological determination of human C-peptide in serum. Diabetologia. 1975 Dec;11(6):541–548. doi: 10.1007/BF01222104. [DOI] [PubMed] [Google Scholar]
- Kuzuya H., Blix P. M., Horwitz D. L., Steiner D. F., Rubenstein A. H. Determination of free and total insulin and C-peptide in insulin-treated diabetics. Diabetes. 1977 Jan;26(1):22–29. doi: 10.2337/diab.26.1.22. [DOI] [PubMed] [Google Scholar]
- Rasmussen S. M., Heding L. G., Parbst E., Volund A. Serum IRI in insulin-treated diabetics during a 24-hour period. Diabetologia. 1975 Apr;11(2):151–158. doi: 10.1007/BF00429840. [DOI] [PubMed] [Google Scholar]
- Tchobroutsky G. Relation of diabetic control to development of microvascular complications. Diabetologia. 1978 Sep;15(3):143–152. doi: 10.1007/BF00421230. [DOI] [PubMed] [Google Scholar]