

Abstract
We report on the case of a 15-year-old adolescent who presented with a transient paraplegia and hyposensibility of the upper extremities after sustaining a minor hyperflexion trauma to the cervical spine. Neuroimaging studies revealed atlantoaxial dislocation and ventral compression of the rostral spinal cord with increased cord signal at C1/C2 levels caused by an os odontoideum, as well as anterior and posterior arch defects of the atlas. The patient underwent closed reduction and posterior atlantoaxial fusion. We describe the association of an acquired instability secondary to an os odontoideum with an anteroposterior spondyloschisis of the atlas and its functional result after 12 months. The rare coincidence of both lesions indicates a multiple malformation of the upper cervical spine and supports the theory of an embryologic genesis of os odontoideum.
Keywords: Os odontoideum, Atlantoaxial instability, C1/C2 fusion, Midline cleft of atlas
Introduction
The craniovertebral junction is a common site for malformations [10]. Clefts of the anterior and posterior arch of the atlas are rare, but well-documented congenital anomalies [1, 2]. Several reports attributed the aetiology of os odontoideum to an either embryologic, traumatic or vascular basis [3–5, 8]. We describe the unusual case of a combined midline cleft of the anterior and posterior arch of the atlas associated with os odontoideum leading to atlantoaxial instability with acute myelopathia after a minor trauma. We presume an embryologic genesis of our findings.
Case report
A 15-year-old male patient injured his cervical spine in a hyperflexion trauma when performing a somersault on a trampoline. He presented with transient numbness and weakness of both arms. Initial X-rays and computed tomography demonstrated a displaced os odontoideum which reduced on extension and a rostral compression of the cervical spinal cord due to a subluxation of C1 over C2 with narrowing of the spinal canal to 50%. Additionally midline clefts of the anterior and posterior arch of the atlas became evident (Figs. 1, 2). MRI scans revealed increased cord signals at C1/C2 levels on T2-weighted images and a persistent subdental synchondrosis was visualized on T2-weighted turbo spin echo sequences (Fig. 3). The patient underwent closed reduction and posterior atlantoaxial fusion by sublaminar tension band wiring with autologous bone grafting and transarticular lag screw fixation. Postoperatively all symptoms improved significantly. Radiographs taken 1 year after the trauma showed a stable fusion of C1/C2 (Fig. 4). The patient presented with a range of motion at 30° of extension, 40° of flexion and 50–0–40° of rotation. He was free of symptoms and had returned to his pre-injury status regarding work and leisure activities.
Fig. 1.

X-rays of the cervical spine in neutral position (a), flexion (b) and extension (c). Ventral subluxation of C1 over C2 in flexion (b), which reduces on extension (c)
Fig. 2.
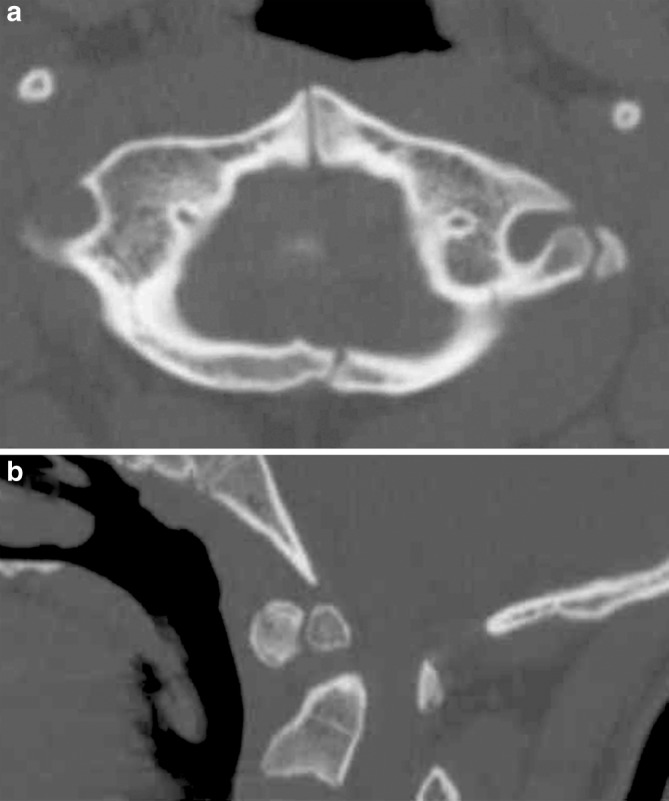
CT scans reveal midline clefts of the anterior and posterior arch of the atlas (a). Displaced os odontoideum and subluxation of C1 over C2 with narrowing of the spinal canal (b)
Fig. 3.
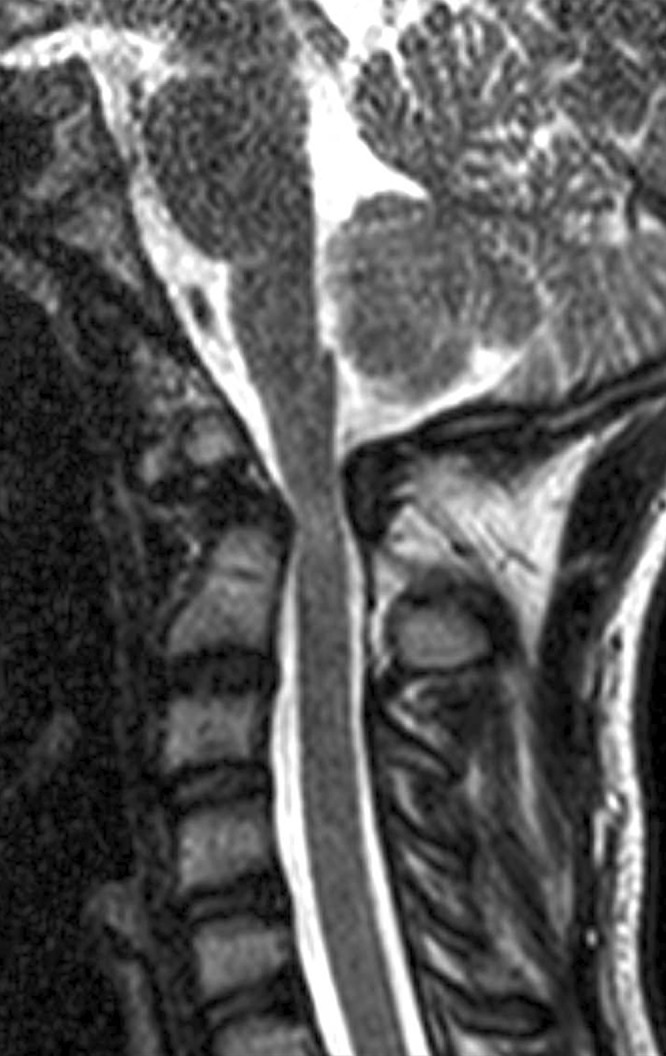
T2-weighted MRI images with increased cord signals at C1/C2 levels and a persistent subdental synchondrosis
Fig. 4.

Follow-up X-rays 12 months after trauma. Stable atlantoaxial fusion after sublaminar wiring and transarticular screw fixation in ap (a) and lateral (b) view
Discussion
The odontoid process and the atlas originate from the first cervical sclerotome. Body of the axis, lateral masses and posterior arch arise entirely from the second cervical sclerotome. The atlas is formed from three primary ossification centres, which develop during the seventh week of gestation. Two centres at the lateral masses extend posteromedially to form the posterior arch usually in the fourth year. Ossification of the anterior arch involves one or two ossification centres, which extend posterolaterally to fuse with lateral masses around the seventh year. The odontoid process separates from the atlas between the sixth and seventh week of intrauterine life and moves caudally to join the body of the axis (Fig. 5).
Fig. 5.

Scheme of the embryologic development of atlas and axis
Os odontoideum is an oval or round shaped ossicle of variable size with a smooth cortical border. Several reports attributed its aetiology to either an embryological, traumatic or vascular basis. Failure of fusion of ossification centres in the odontoid process has been considered to be the main aetiology [8]. Considerable evidence on cases of acquired os odontoideum indicates, that occult fractures with subsequent avascular necrosis might result in similar pathology [5]. O’Rahilly et al. [9] studied the cervical spine of 8-weeks-old human embryos and observed that axis consists morphologically of three parts. Two rostral parts form the odontoid process and a caudal part gives rise to the axis body, separated from the middle part by subdental synchondrosis. A segmentation anomaly of the two rostral parts, which never occurred in normal individuals, may result in bipartite dens [3]. Currarino [3] reported 11 cases with complete or partial segmentation defect in mid odontoid, suggesting an embryological anomaly characterized by a complete segmentation of two rostral parts of axis which may explain the congenital os odontoideum.
Malformations of the atlas are very rare and include both clefts and aplasias [1, 2]. Galindo and Francis [6] reported the incidence of anteroposterior spondyloschisis of the atlas in normal individuals as 0.3%.
Atasoy et al. [1] reported the first case of bipartite atlas with os odontoideum causing spinal stenosis. Garg et al. [7] presented a report of bipartite atlas with anterior arch aplasia associated to an os odontoideum. They found a small projection on the anterior surface of the dens and concluded that the ossification centre of anterior arch of atlas may fail to separate from future dens resulting in anterior arch aplasia with a small tubercle attached to the anterior surface of the dens. To our knowledge no other case of bipartite atlas with os odontoideum had been reported previously in the English literature.
In our case, there was a malformation of the anterior and posterior arch of the atlas and a persistent subdental synchondrosis, both likely to be a result of a congenital failure of fusion of ossification centres. The associated os odontoideum was clinically silent until a traumatic instability occurred which resulted in acute myelopathy.
Our findings support the theory of a congenital aetiology of os odontoideum. Both the combined anterior and posterior clefts of atlas and os odontoideum are either asymptomatic or, if cervical instability arises, may develop neurological symptoms.
Conclusion
We described a rare association of an anterior and posterior midline cleft of the atlas with an os odontoideum in an adolescent. An embryologic genesis is likely. Minor trauma is commonly the cause for the onset of symptoms, which may occur immediately after the injury, be transitory and experienced repeatedly or have a delayed progressive course. If the lesion is reducible, atlantoaxial fusion is recommended.
References
- 1.Atasoy C, Fitoz S, Karan B, Eden I, Akyar S. A rare cause of cervical spinal stenosis: posterior arch hypoplasia in a bipartite atlas. Neuroradiology. 2002;44:253–255. doi: 10.1007/s00234-001-0740-4. [DOI] [PubMed] [Google Scholar]
- 2.Childers JC, Wilson FC. Bipartite atlas. J Bone Joint Surg. 2002;53A:578–582. [PubMed] [Google Scholar]
- 3.Currarino G. Segmentation defect in the midodontoid process and its possible relationship to the congenital type of os odontoideum. Pediatr Radiol. 2002;32:34–40. doi: 10.1007/s00247-001-0579-1. [DOI] [PubMed] [Google Scholar]
- 4.Dai LY, Yuan W, Ni B, Jia L. Os odontoideum: aetiology, diagnosis and management. Surg Neurol. 2000;53:106–108. doi: 10.1016/S0090-3019(99)00184-6. [DOI] [PubMed] [Google Scholar]
- 5.Fielding JW, Hensinger RN, Hawkins RJ. Os odontoideum. J Bone Joint Surg. 1980;62A:376–383. [PubMed] [Google Scholar]
- 6.Galindo MJ, Francis WR. Atlantal fracture in a child through congenital anterior and posterior arch defects: a case report. Clin Orthop. 1983;140:220–222. [PubMed] [Google Scholar]
- 7.Garg A, Gaikwad S, Gupta V, Mishra N, Kale S, Singh J. Bipartite atlas with os odontoideum: case report. Spine. 2004;29(2):E35–E38. doi: 10.1097/01.BRS.0000106487.89648.88. [DOI] [PubMed] [Google Scholar]
- 8.Morgan MK, Onofrio BM, Bender CE. Familial os odontoideum: case report. J Neurosurg. 1989;70:636–639. doi: 10.3171/jns.1989.70.4.0636. [DOI] [PubMed] [Google Scholar]
- 9.O’Rahilly R, Muller F, Meyer DB. The human vertebral column at the end of the embryonic period: Part 2. The occipitocervical region. J Anat. 1983;136:181–195. [PMC free article] [PubMed] [Google Scholar]
- 10.VanGilder JC, Menezes AH, Dolan KD. The craniovertebral junction and its abnormalities. Mount Kisco New York: Futura; 1987. [Google Scholar]