

Abstract
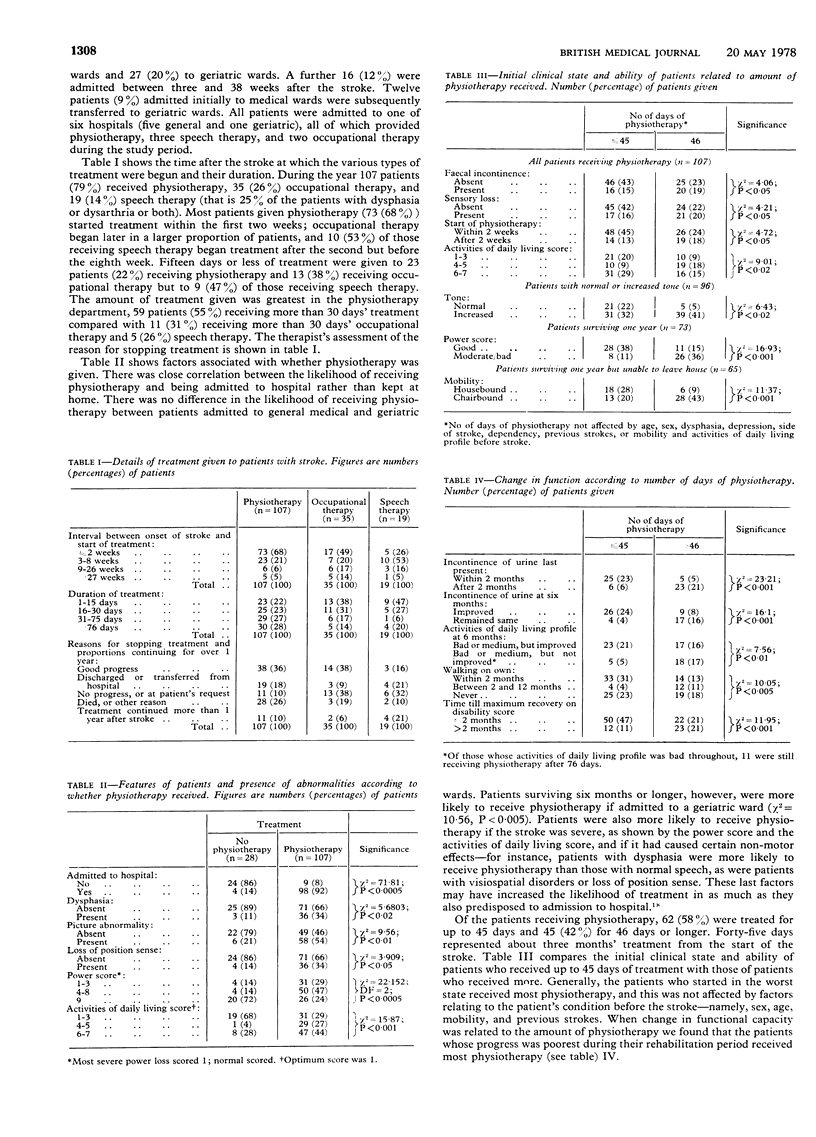
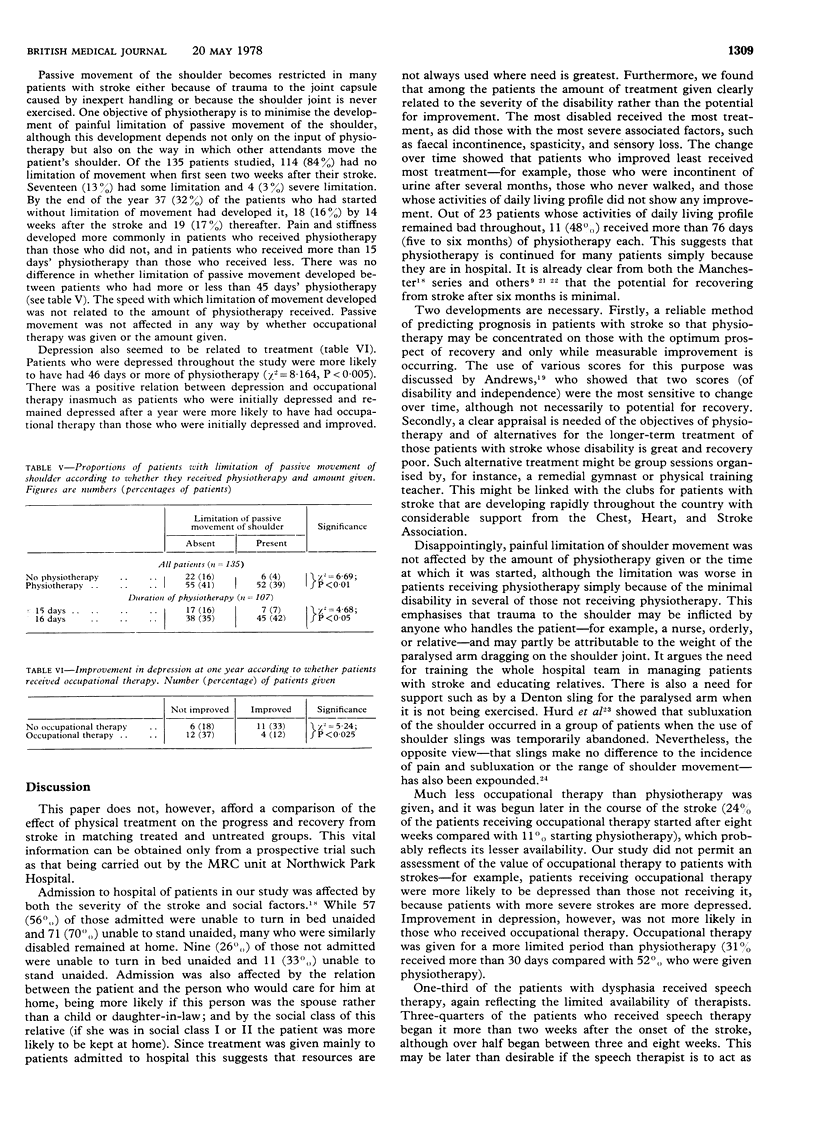
The use of physiotherapy, occupational therapy, and speech therapy for patients with stroke was investigated, and the three treatments were compared. Out of 135 patients with stroke surviving at two weeks, 107 received physiotherapy, but only 35 received occupational therapy and 19 speech therapy. Those who received most physiotherapy were the most severely disabled and had the worst prognosis, and, although almost no recovery occurred after six months, 30 patients continued with treatment beyond this time. Stiff and painful shoulders were present in 21 of the patients by two weeks and had developed in a further 37 by one year. Physiotherapy did not prevent this. The objectives of physiotherapy for patients with stroke need careful definition, with emphasis on treatment in the early months. Alternative treatment, possibly carried out by volunteers or more simply trained personnel, merits further consideration.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ADAMS G. F., McCOMB S. G. Assessment and prognosis in hemiplegia. Lancet. 1953 Aug 8;265(6780):266–269. doi: 10.1016/s0140-6736(53)91128-3. [DOI] [PubMed] [Google Scholar]
- BARD G., HIRSCHBERG G. G. RECOVERY OF VOLUNTARY MOTION IN UPPER EXTREMITY FOLLOWING HEMIPLEGIA. Arch Phys Med Rehabil. 1965 Aug;46:567–572. [PubMed] [Google Scholar]
- Bourestom N. C. Predictors of long-term recovery in cerebrovascular disease. Arch Phys Med Rehabil. 1967 Aug;48(8):415–419. [PubMed] [Google Scholar]
- HOBERMAN M., SPRINGER C. F. Rehabilitation of the permanently and totally disabled patient. Arch Phys Med Rehabil. 1958 Apr;39(4):235–240. [PubMed] [Google Scholar]
- Hurd M. M., Farrell K. H., Waylonis G. W. Shoulder sling for hemiplegia: friend or foe? Arch Phys Med Rehabil. 1974 Nov;55(11):519–522. [PubMed] [Google Scholar]
- LOWENTHAL M. Recent advances in the evaluation and management of the hemiplegic patient. N Y State J Med. 1960 Oct 15;60:3235–3238. [PubMed] [Google Scholar]
- LOWENTHAL M., TOBIS J. S., HOWARD I. R. An analysis of the rehabilitation needs and prognoses of 232 cases of cerebral vascular accident. Arch Phys Med Rehabil. 1959 May;40(5):183–186. [PubMed] [Google Scholar]
- Lehmann J. F., DeLateur B. J., Fowler R. S., Jr, Warren C. G., Arnhold R., Schertzer G., Hurka R., Whitmore J. J., Masock A. J., Chambers K. H. Stroke: Does rehabilitation affect outcome? Arch Phys Med Rehabil. 1975 Sep;56(9):375–382. [PubMed] [Google Scholar]
- MAHONEY F. I., BARTHEL D. W. Rehabilitation of the hemiplegic patient: a clinical evaluation. Arch Phys Med Rehabil. 1954 Jun;35(6):359–362. [PubMed] [Google Scholar]
- Stern P. H., McDowell F., Miller J. M., Robinson M. Factors influencing stroke rehabilitation. Stroke. 1971 May-Jun;2(3):213–218. doi: 10.1161/01.str.2.3.213. [DOI] [PubMed] [Google Scholar]
- Waylonis G. W., Keith M. W., Aseff J. N. Stroke rehabilitation in a Midwestern county. Arch Phys Med Rehabil. 1973 Apr;54(4):151–passim. [PubMed] [Google Scholar]
- Wilkes E. Community care. Physiotherapy. 1975 Dec;61(12):365–367. [PubMed] [Google Scholar]
- Wylie C. M. The value of early rehabilitation in stroke. Geriatrics. 1970 May;25(5):107–113. [PubMed] [Google Scholar]