

Abstract
Background
People with diabetes mellitus are more likely to have cardiovascular, renal and ophthalmic comorbidity than those without diabetes. Information on the economic impact of diabetes and its complications on the Canadian health care system is limited.
Methods
To estimate health care expenditures for diabetes and its major complications, we identified people with diabetes in 1996 in Saskatchewan, using the administrative databases of Saskatchewan Health. We grouped utilization and expenditure data for prescription drugs, physician services, hospitalizations, day surgery procedures and dialysis services according to cardiovascular, renal and ophthalmic services, according to billing codes and the American Hospital Formulary Services classification for prescription drugs.
Results
Of the 38 124 people identified (48.5% female and 9.7% registered Indians), 46.6% had cardiovascular-related records, 19.8% ophthalmic-related records and 6.6% renal-related records. Registered Indians had significantly fewer (p < 0.001) cardiovascular-related records than the rest of the diabetic population (35.1% v. 47.9%, respectively) but more renal- related records (11.7% v. 6.0%, respectively). The total 1996 Saskatchewan Health expenditure for the study group, within the observed categories, was estimated to be $134.3 million, of which $35.5 million (26.4%) was for cardiovascular-related services, $10 million (7.5%) for renal-related services and $3.3 million (2.5%) for ophthalmic-related services.
Interpretation
In 1996, 36.4% of health care expenditures for people with diabetes was attributable to major comorbidity. Actions to prevent or control such comorbidity will yield significant cost savings.
Between 5% and 6% of Canadians over the age of 12 years have diabetes mellitus.1 People with diabetes are at increased risk of macrovascular and microvascular complications2,3 and are more likely than people without diabetes to have other cardiovascular risk factors, such as hypertension and hyperlipidemia.4,5 These factors contribute to an increased risk of illness and death,2,6,7,8,9 which places a significant burden on our health care system.
In 1997, the direct expenditures for health care services attributable to diabetes were estimated to be $44.1 billion in the United States.10 Management of chronic complications associated with diabetes, such as cardiovascular, renal and ophthalmic disease, accounted for approximately 27% of these expenditures.10 Observations from managed care organizations in the United States suggest that annual management costs for people with diabetes are 1.5 to 2 times higher than those for people without diabetes.11,12 As diabetes-related complications develop and progress, management costs increase.13,14
Information on the economic impact of diabetes and its complications on the Canadian health care system is limited. The annual cost of diabetes in Canada has been estimated at US$9 billion from an extrapolation by the Canadian Diabetes Association.1 Recently, with a top-down costing method, the direct medical costs of hospital services, physician services and medications for diabetes in Canada were estimated at US$2.6 billion, or approximately 8% of the total medical expenditures in Canada for 1998.15 Although the model provided some insight, the estimates were limited by the top-down approach and the use of a model rather than direct observation.
Our study was designed to estimate the resource use and associated expenditures for diabetes and major comorbidity from empirical data for the population with diabetes in Saskatchewan in 1996. Resource use and associated costs for registered Indians were included in this analysis; however, expenditures for this group were reported separately because of the different epidemiologic features of diabetes in this subpopulation and the lack of data on prescription drug use of registered Indians in Saskatchewan Health databases. The study was approved by the Health Research Ethics Board of the University of Alberta and the Data Access Review Committee of Saskatchewan Health.
Methods
Setting
We obtained population descriptors and information on prescription drug use, hospitalizations, day surgery procedures, physician services and dialysis from the linkable health care databases of Saskatchewan Health.16 Nearly all residents of Saskatchewan are eligible for insured health care services, and certain service transactions are tracked by means of a unique health services number for each resident. The prescription drug database contains records of all outpatient dispensations of drugs covered by the Saskatchewan Prescription Drug Plan (SPDP). This database provides information on the drug and quantity dispensed, as well as the share of the cost that is covered by the SPDP and that covered by the patient. Registered Indians receive prescription drug coverage under a federal program; therefore, their medication use is not recorded in the provincial database. The hospital and physician databases contain records of all medically necessary hospitalizations and physician services that are covered by the provincial health care system. Each hospital separation record contains the dates of admission and discharge, the resource intensity weight (RIW) (an estimated level of acuity for the admission, assigned by the Canadian Institute for Health Information [CIHI]), the primary, secondary and tertiary diagnoses (coded according to the World Health Organization International Classification of Diseases, 9th revision [ICD-9]17), and the type of discharge (alive or dead). Each physician record includes the ICD-9 diagnosis code, type of physician, fee-for-service procedure codes and approved payment. The continuous and comprehensive health care information for Saskatchewan residents in the Saskatchewan Health databases has been useful for numerous epidemiologic studies.16
Subject identification
From health care records for 1991 through 1996, we selected for the cohort all persons that we could assume had diabetes because of 1 or more dispensation records for insulin or an oral antidiabetic agent, 2 or more physician service claims for diabetes (ICD-9 code 250) within a 2-year period, or 1 or more hospitalizations with a diabetes code as the primary, secondary or tertiary diagnosis. The physician and hospital components of this algorithm are highly specific for diabetes.18,19 The addition of prescription drug use to the algorithm likely improves its sensitivity. However, because prescription drug use is not recorded for registered Indians, the prevalence of diabetes in this group was underestimated; consequently, the resource use and expenditures for this group were also underestimated.
Identification of expenditures
We abstracted information on prescription drug use, hospitalizations and physician services for the cohort in 1996 from the corresponding databases. For day surgery procedures, we abstracted the date of service, ICD-9 diagnosis code and day procedure RIW from the hospital services files. Using the physician services database, we identified people receiving dialysis services from fee-for-service codes, then determined the type and duration of dialysis from the physician service claims for initiation of hemodialysis, maintenance hemodialysis and peritoneal dialysis.
Expenditures for prescription drugs and physician services in 1996 were taken directly from corresponding database records. We estimated hospitalization expenditures with the use of a weighted cost per RIW of $2165, derived from the Saskatchewan acute care funding pool for 1996–97. For the approximately 21% of hospital separation records in 1996 that lacked an RIW, we imputed one from Saskatchewan Health estimates for hospitals of similar size. We estimated expenditures for day surgery procedures by multiplying the weighted cost per RIW ($2165) by the mean day procedure RIW for cohort members in 1996 (0.29). To estimate dialysis expenditures, we deflated to 1996 dollars the annual costs for hemodialysis and peritoneal dialysis estimated in 2000 dollars by Lee and colleagues,20 using the Saskatchewan Consumer Price Index for Health Care Services. All expenditures are reported in 1996 Canadian dollars.
Complication categories
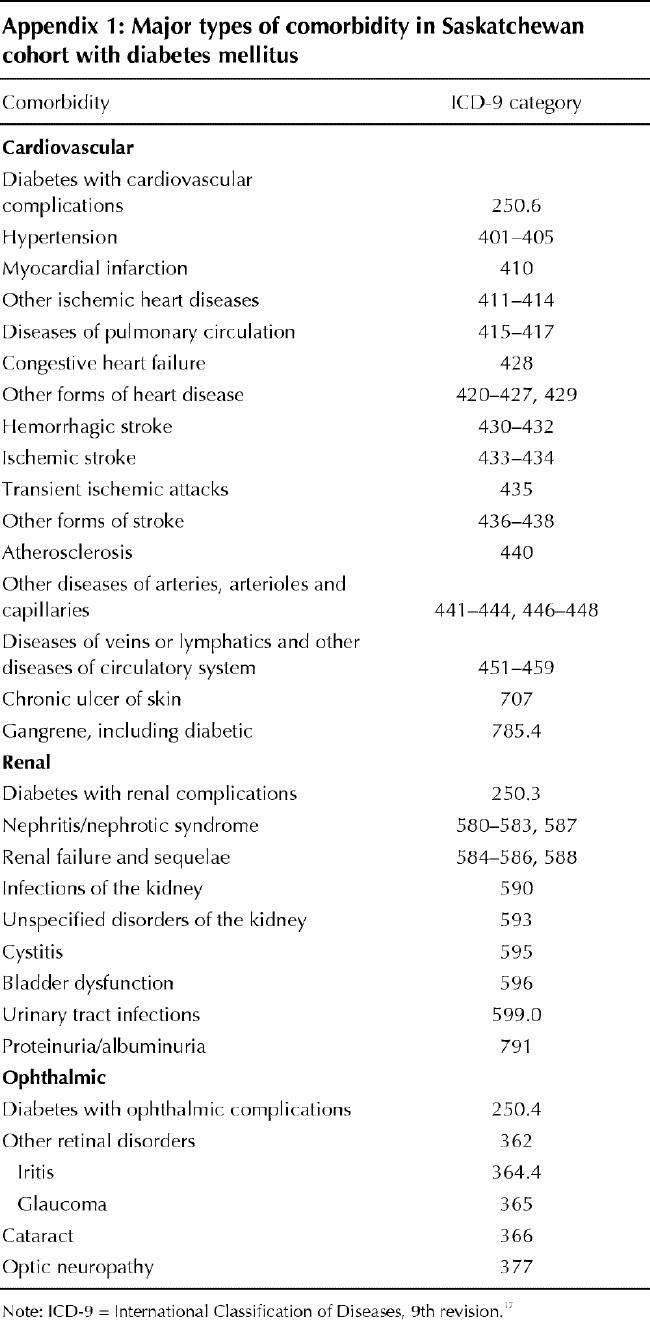
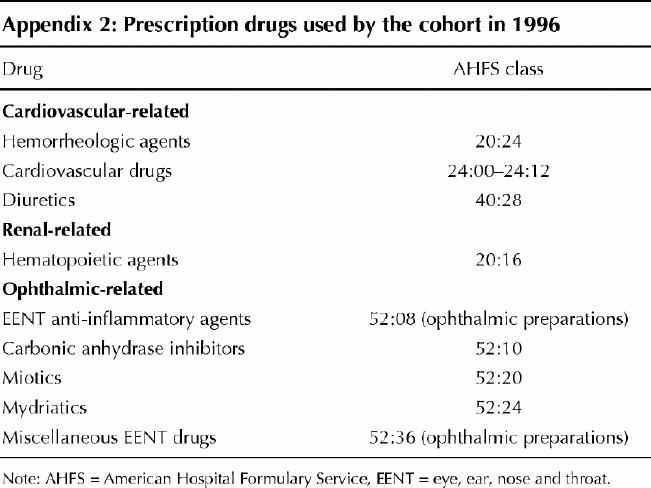
We grouped the ICD-9 diagnosis and procedure codes according to cardiovascular, renal, ophthalmic and other conditions (Appendix 1). According to CIHI coding rules, the primary diagnosis is the diagnosis most responsible for the length of stay and the resources consumed during the stay; therefore, we grouped hospitalizations by the primary diagnosis. We grouped the physician service claims by diagnosis and service codes. When there was a discrepancy between these codes (e.g., the diagnosis code referred to one comorbidity and the procedure code to a different comorbidity), we assigned a single comorbidity to the claim, using a hierarchical system. Types of comorbidity were ranked in descending order of importance as follows: cardiovascular, renal, ophthalmic and other. We grouped the physician claims for dialysis services and the estimated expenditures for outpatient dialysis services under renal comorbidity. Prescription drugs were classified according to the American Hospital Formulary Service and grouped in the same categories of comorbidity (Appendix 2).
Statistical methods
We used descriptive statistics for demographic information and expenditures and an ordinary least-squares regression model for evaluating the association among various subject characteristics, the presence of major diabetes-related comorbidity and the estimated expenditures for care.21,22 To compare registered Indians with the rest of the diabetic population, we used the sum of expenditures for physician services, hospitalizations, day surgery and dialysis services as the estimated expenditure for care in the regression model. Previous evaluations with this data set have found a positive skew for this estimate; that is, a small percentage of the cohort had very high expenditures.23 Therefore, the natural log transformation of the estimate (ln expenditure) was used as the dependent variable and regressed against age, sex, registered Indian status and presence of major comorbidity.
Results
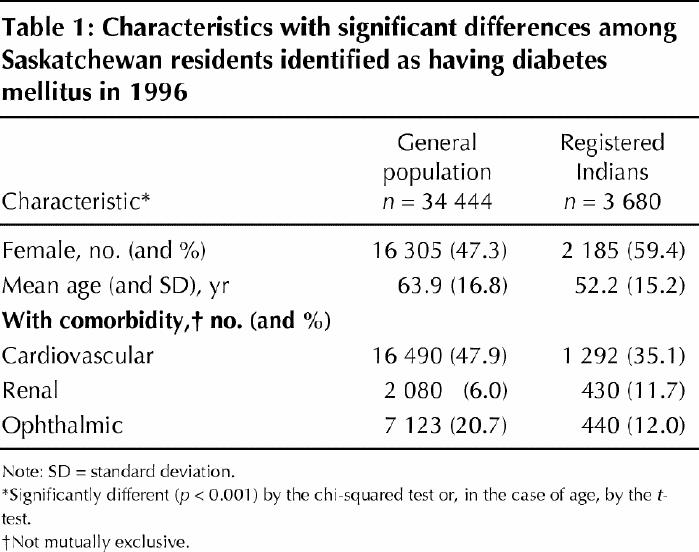
Detailed information on the 38 124 people in Saskatchewan identified as having diabetes in 1996 is provided elsewhere.23 The registered Indian group was younger than the general population with diabetes and had a higher proportion of women (Table 1).
Table 1
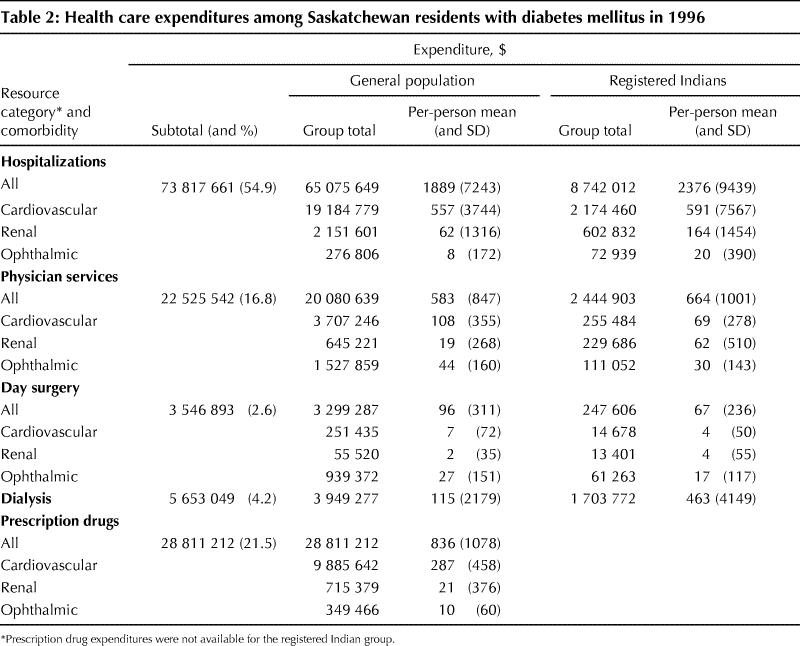
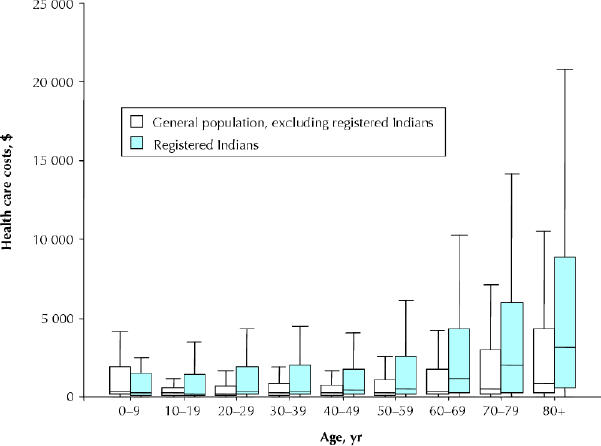
The total 1996 Saskatchewan Health expenditure for the cohort, within the observed categories, was estimated to be $134.3 million. Hospitalization accounted for the largest portion (54.9%), and prescription drugs, physician services, dialysis services and day surgical procedures for smaller portions in decreasing order (Table 2). The mean total health care expenditure per person was $3524. When prescription drug expenditures were excluded, the mean was $2768. Expenditure patterns were similar in the general population and the registered Indian group until the age of 60 (Fig. 1); thereafter, the median expenditure increased more rapidly for registered Indians.
Table 2
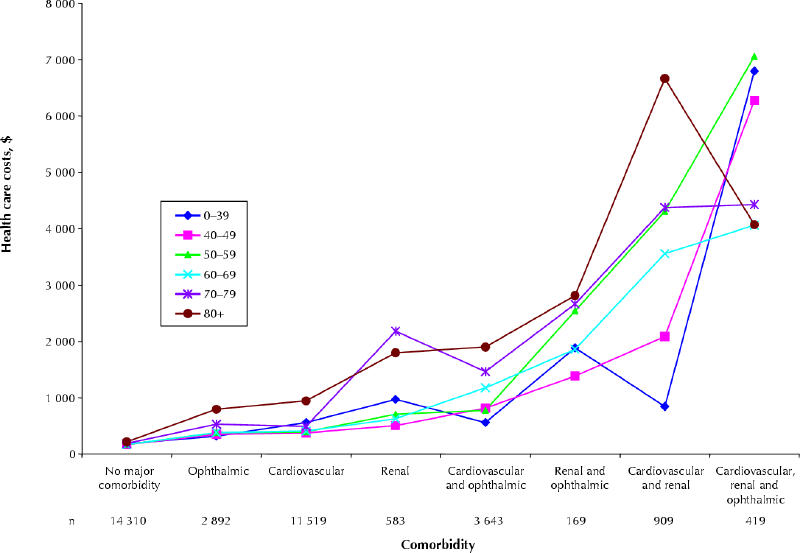
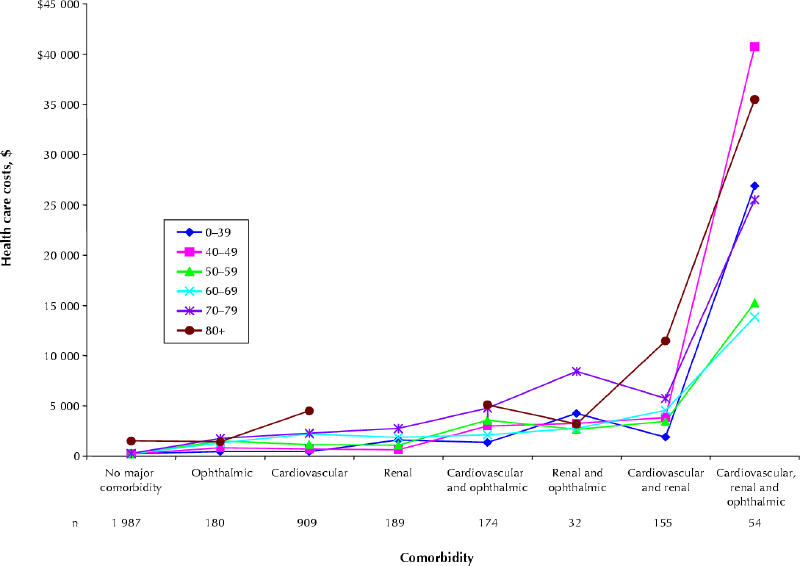
According to the diagnostic codes, cardiovascular comorbidity was present in 46.6% of the cohort, ophthalmic comorbidity in 19.8% and renal comorbidity in 6.6%. Renal comorbidity was more common in the registered Indian group, whereas ophthalmic and cardiovascular comorbidity was more common in the general population (Table 1). Many people had more than 1 type of comorbidity, and 1.2% (473) had all 3 major types. Of the total health care expenditure of $134.3 million, 36.4% was attributable to major comorbidity: $35.5 million (26.4%) to cardiovascular-related services, $10 million (7.5%) to renal-related services and $3.3 million (2.5%) to ophthalmic-related services. The median expenditures by comorbidity and age are shown for the general population and the registered Indian group in Figs. 2A and 2B, respectively. The overall median for those without major comorbidity was $186, for those with ophthalmic comorbidity alone $449, for those with cardiovascular comorbidity alone $508 and for those with renal comorbidity alone $1050. People with 2 or more types of comorbidity had even higher health care expenditures. It appears that as the number of types of comorbidity increases, health care expenditures increase. Furthermore, expenditures for those with cardiovascular and renal complications were much greater among registered Indians than in the general population with diabetes.
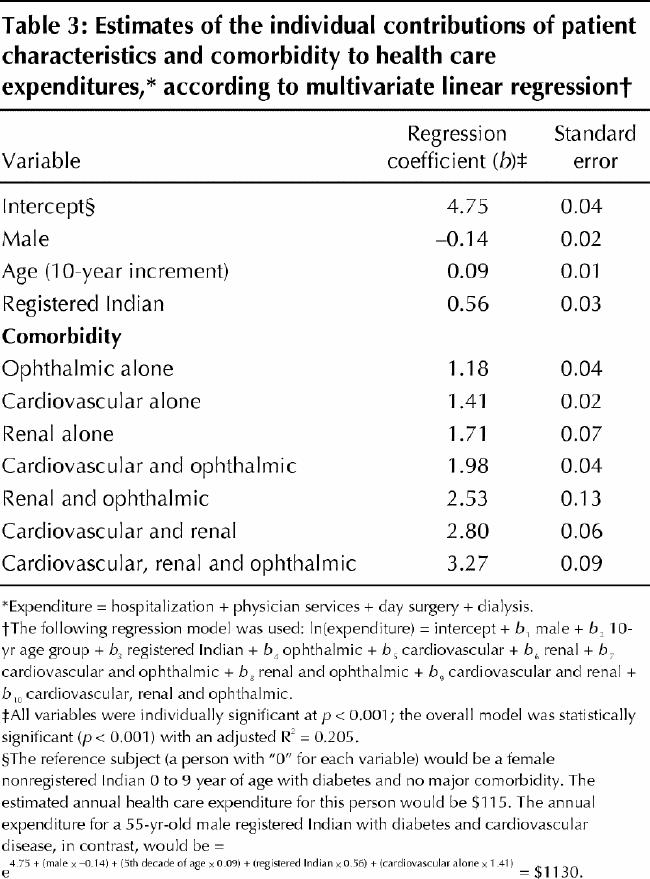
According to the multivariate regression (Table 3), health care expenditures were significantly greater when there was a major type of diabetes-related comorbidity. Age, sex and registered Indian status also had a significant impact on health care expenditure. In this model, the regression coefficients represented the contribution of the variables to the estimated total health care expenditure. For example, the estimated annual expenditure for a 55-year-old male registered Indian with diabetes and cardiovascular disease would be $1130. The overall model was statistically significant and explained 20.5% of the total variance in health care expenditures.
Table 3
Interpretation
The 38 124 people identified in this study as having diabetes represented 3.6% of the Saskatchewan population in 1996.24 We estimated that the health care expenditure for the cohort was $134.3 million, or approximately 15% of the total expenditure for hospitalizations, physician services and prescription drugs in Saskatchewan that year. The expenditures for people with concurrent ophthalmic, cardiovascular or renal disorders in the cohort were much higher than the expenditures for those with no major comorbidity. As the number of major complications increased, expenditures grew significantly.
We estimated that 36.4% of the cohort's diabetes- related expenditures were attributable to major comorbidity. This estimate is similar to that of Selby and associates,11 who reported that 33.9% of the excess costs of care for diabetes were attributable to cardiovascular disease, end-stage renal disease and ophthalmic disease. Others25,26 have reported that 41% to 50% of expenditures for people with diabetes could be attributable to long-term complications; however, the subjects of these studies primarily had type 2 diabetes. The inclusion of younger subjects with type 1 diabetes may have lowered the prevalence of complications in our cohort.
Several limitations of our study should be noted. First, we drew data from administrative health care databases and, as such, relied on the accuracy and completeness of the records. The Saskatchewan Health databases have, however, been used in numerous epidemiologic studies and are recognized as providing well-validated and comprehensive data.16 Second, the algorithm used to identify people with diabetes from the administrative records likely underestimated the true prevalence of diabetes in the province; therefore, the total health care expenditures were likely underestimated. In addition, registered Indians with diabetes were not identified from their prescription drug use. Furthermore, people with less than moderate diabetes during the study period may not have met the inclusion criteria; that is, their diabetes was never severe enough to require medication, 2 physician visits in a 2-year period or a hospitalization. Third, some physicians in Saskatchewan, particularly in the northern regions, are salaried; therefore, our use of physician service records underestimated the use of services by all people with diabetes in Saskatchewan. Finally, the databases that we used do not record services provided at the health district level, such as those associated with diabetes educators and dietitians in both inpatient and outpatient settings and podiatric services, nor do they record auxiliary costs of transplantation (e.g., those for transplant coordinators and living donors); therefore, the overall total costs were underestimates.
The magnitude of the expenditures indicates significant potential savings from prevention initiatives. Aggressive management of hyperglycemia, advocated by the Canadian Diabetes Association and the American Diabetes Association,27,28,29 reduces the risk of many long-term complications of diabetes.30,31,32,33,34 Interventions to reduce elevated blood pressure and cholesterol levels, which are common in people with diabetes,4,5 also delay the progression of cardiovascular and renal complications.35,36,37,38,39 Strategies targeted at preventing the onset of diabetes40,41 or delaying the progression of complications42 could produce substantial savings to the health care system.
Acknowledgments
We thank Dr. William Osei, Winanne Downey and Patricia Beck for their contributions to this study and for their comments on a draft of the article. The study was based in part on nonidentifiable data provided to the Institute of Health Economics in kind by Saskatchewan Health. The interpretation and conclusions contained herein are the authors' and do not necessarily represent those of the Government of Saskatchewan or Saskatchewan Health.
Appendix 1.
Appendix 2.
Footnotes
This article has been peer reviewed.
Contributors: Dr. Simpson conducted the statistical analysis. All authors contributed to the initial draft of the manuscript and the revisions and approved the final version.
This project was supported by funding from Aventis Pharma Inc., the Institute of Health Economics and the Alberta Heritage Foundation for Medical Research (AHFMR). Dr. Johnson holds a Canada Research Chair in Diabetes Health Outcomes and a Population Health Investigator Award from the AHFMR.
Competing interests: None declared.
Correspondence to: Dr. Jeffrey A. Johnson, Institute of Health Economics, #1200–10405 Jasper Ave., Edmonton AB T5J 3N4; fax 780 448-0018; jeff.johnson@ualberta.ca
References
- 1.Diabetes in Canada: national statistics and opportunities for improved surveillance, prevention, and control. Ottawa: Health Canada, 1999. Cat no H49-121/1999.
- 2.Morrish NJ, Wang S-L, Stevens LK, Fuller JH, Keen H. Mortality and causes of death in the WHO multinational study of vascular disease in diabetes. Diabetologia 2001;44(Suppl 2):S14-S21. [DOI] [PubMed]
- 3.Tan MH, MacLean DR. Epidemiology of diabetes mellitus in Canada. Clin Invest Med 1995;18:240-6. [PubMed]
- 4.Wingard DL, Barrett-Connor E, Criqui MH, Suarez L. Clustering of heart disease risk factors in diabetic compared to nondiabetic adults. Am J Epidemiol 1983;117:19-26. [DOI] [PubMed]
- 5.Stamler J, Vaccaro O, Neaton JD, Wentworth D. Diabetes, other risk factors and 12-year cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care 1993;16:434-44. [DOI] [PubMed]
- 6.Gatling W, Tufail S, Mullee MA, Westacott TA, Hill RD. Mortality rates in diabetic patients from a community-based population compared to local age/sex matched controls. Diabet Med 1997;14:316-20. [DOI] [PubMed]
- 7.Gu K, Cowie CC, Harris MI. Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971–1993. Diabetes Care 1998;21:1138-45. [DOI] [PubMed]
- 8.Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339:229-34. [DOI] [PubMed]
- 9.Jude EB, Oyibo SO, Chalmers N, Boulton AJM. Peripheral arterial disease in diabetic and nondiabetic patients. Diabetes Care 2001;24:1433-7. [DOI] [PubMed]
- 10.Economic consequences of diabetes mellitus in the U.S. in 1997. American Diabetes Association. Diabetes Care 1998;21:296-309. [DOI] [PubMed]
- 11.Selby JV, Ray GT, Zhang D, Colby CJ. Excess costs of medical care for patients with diabetes in a managed care population. Diabetes Care 1997;20: 1396-402. [DOI] [PubMed]
- 12.Ramsey SD, Newton K, Blough D, McCulloch DK, Sandhu N, Wagner EH. Patient-level estimates of the cost of complications in diabetes in a managed-care population. Pharmacoeconomics 1999;16:285-95. [DOI] [PubMed]
- 13.Brown JB, Pedula KL, Bakst AW. The progressive cost of complications in type 2 diabetes mellitus. Arch Intern Med 1999;159:1873-80. [DOI] [PubMed]
- 14.O'Brien JA, Shomphe LA, Kavanagh PL, Raggio G, Caro JJ. Direct medical costs of complications resulting from type 2 diabetes in the U.S. Diabetes Care 1998;21:1122-8. [DOI] [PubMed]
- 15.Dawson KG, Gomes D, Gerstein H, Blanchard JF, Kahler KH. The economic cost of diabetes in Canada, 1998. Diabetes Care 2002;25:1303-7. [DOI] [PubMed]
- 16.Downey W, Beck P, McNutt M, Stang M, Osei W, Nichol J. Health databases in Saskatchewan. In: Strom B, editor. Pharmacoepidemiology. Chinchester: Wiley; 2000. p. 325-45.
- 17.World Health Organization manual of the International Statistical Classification of Diseases, Injuries, and Causes of Death, 9th rev. Geneva: World Health Organization; 1977.
- 18.Blanchard JF, Ludwig S, Wajda A, Dean H, Anderson K, Kendall O, et al. Incidence and prevalence of diabetes in Manitoba, 1986–1991. Diabetes Care 1996;19:807-11. [DOI] [PubMed]
- 19.Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care 2002;25:512-6. [DOI] [PubMed]
- 20.Lee H, Manns B, Taub K, Ghali WA, Dean S, Johnson D, et al. Cost analysis of ongoing care of patients with end-stage renal disease: the impact of dialysis modality and dialysis access. Am J Kidney Dis 2002;40:611-22. [DOI] [PubMed]
- 21.Johnson JA, Connolly MA, Jacobs P, Montgomery M, Brown N, Zuberbuhler P. Costs of care for individuals with cystic fibrosis in Alberta: a regression approach to determining the impact of recombinant human DNase. Pharmacotherapy 1999;19:1159-66. [DOI] [PubMed]
- 22.Hu TW, Jerrell J. Cost-effectiveness of alternative approaches in treating severely mentally ill in California. Schizophr Bull 1991;17:461-8. [DOI] [PubMed]
- 23.Johnson JA, Simpson SH, Jacobs P, Downey W, Beck P, Osei W. Cost of health care for people with diabetes mellitus in Saskatchewan 1991 to 1996. Edmonton: Institute of Health Economics, 2002. Working paper 02-02.
- 24.Report of the Saskatchewan Advisory Committee on Diabetes. Diabetes 2000: recommendations for a strategy on diabetes prevention and control in Saskatchewan. Regina: Saskatchewan Health, 2000.
- 25.Huse DM, Oster G, Killen AR, Lacy MJ, Colditz GA. The economic cost of non-insulin-dependent diabetes mellitus. JAMA 1989;262:2708-13. [DOI] [PubMed]
- 26.Nichols GA, Brown JB. The impact of cardiovascular disease on medical care costs in subjects with and without type 2 diabetes. Diabetes Care 2002;25:482-6. [DOI] [PubMed]
- 27.Meltzer S, Leiter L, Daneman D, Gerstein HC, Lau D, Ludwig S, et al. 1998 clinical practice guidelines for the management of diabetes in Canada. Canadian Diabetes Association. CMAJ 1998;159(Suppl 8):S1-29. [PMC free article] [PubMed]
- 28.Implications of the diabetes control and complications trial. American Diabetes Association. Diabetes Care 2002;25(Suppl 1):S25-7. [DOI] [PubMed]
- 29.Implications of the United Kingdom prospective diabetes study. American Diabetes Association. Diabetes Care 2002;25(Suppl 1):S28-32. [DOI] [PubMed]
- 30.The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-86. [DOI] [PubMed]
- 31.Reichard P, Nilsson B-Y, Rosenqvist U. The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. N Engl J Med 1993;329:304-9. [DOI] [PubMed]
- 32.Shichiri M, Kishikawa H, Ohkubo Y, Wake N. Long-term results of the Kumamoto study on optimal diabetes control in type 2 diabetic patients. Diabetes Care 2000;23(Suppl 2):B21-9. [PubMed]
- 33.Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study Group. Lancet 1998;352:837-53. [PubMed]
- 34.Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study Group. Lancet 1998;352:854-65. [PubMed]
- 35.Parving HH, Andersen AR, Smidt UM, Svendsen PA. Early aggressive antihypertensive treatment reduces rate of decline in kidney function in diabetic nephropathy. BMJ 1982;285:685-8. [DOI] [PubMed]
- 36.Parving HH, Rossing P, Hommel E, Schmidt UM. Angiotensin-converting enzyme inhibition in diabetic nephropathy: ten years' experience. Am J Kidney Dis 1995;26:99-107. [DOI] [PubMed]
- 37.Marre M, Chatellier G, Leblanc H, Guyenne TT, Menard J, Passa P. Prevention of diabetic nephropathy with enalapril in normotensive diabetics with microalbuminuria. BMJ 1988;297:1092-5. [DOI] [PMC free article] [PubMed]
- 38.Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting enzyme inhibition on diabetic nephropathy. N Engl J Med 1993;329:1456-62. [DOI] [PubMed]
- 39.Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 39. UK Prospective Diabetes Study Group. BMJ 1998;317:713-20. [PMC free article] [PubMed]
- 40.Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among individuals with impaired glucose tolerance. N Engl J Med 2001;344:1343-50. [DOI] [PubMed]
- 41.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. Diabetes Prevention Program Research Group. N Engl J Med 2002;346:393-403. [DOI] [PMC free article] [PubMed]
- 42.Golan L, Birkmeyer JD, Welch HG. The cost-effectiveness of treating all patients with type 2 diabetes with angiotensin-converting enzyme inhibitors. Ann Intern Med 1999;131:660-7. [DOI] [PubMed]