

This article reviews the typical imaging characteristics of a vertebral pneumatocyst, an unusual, intraosseous gas-containing lesion of uncertain etiology. Pneumatocysts are usually found within the ilium or sacrum, adjacent to the sacroiliac joints. Fewer than 12 case reports of pneumatocysts of the spine were identified in the English-language literature; in eight of these cases, the lesions were present within the cervical spine (1–7). However, pneumatocysts are probably more common than has been reported. Vertebral body pneumatocysts are benign lesions that need to be differentiated from other gas-containing lesions of the spine, including those caused by osteomyelitis, osteonecrosis, and neoplasm as well as posttraumatic and postsurgical causes. The etiology and natural course of pneumatocysts are poorly understood, although the diagnosis can be reliably determined through a combination of computed tomography (CT) and magnetic resonance (MR) imaging characteristics alone, as shown in the five case studies below.
CASE STUDIES
A 58-year-old woman with a history of breast carcinoma diagnosed 2 years earlier presented to her primary care physician with worsening neck pain, bilateral shoulder pain, and bilateral upper-extremity paresthesias of gradual onset. Her CT images showed a pneumatocyst (Figure 1).
Figure 1.

(a) Sagittal T2- and (b) T1-weighted images of the cervical spine reveal a well-circumscribed focus of decreased signal intensity (arrows) within the C7 vertebral body. Given these findings, a blastic metastasis was initially suspected, given the patient's previous diagnosis of breast cancer. (c) Axial CT image shows a well-circumscribed, nonexpansile low-attenuation focus (arrow) within the central portion of the vertebral body consistent with gas density. The cortical margins of the vertebral body remain intact. This finding is seen in the setting of advanced spondylosis. (d) Sagittal reformatted CT image shows a large lucent focus containing gas density (arrow) within the central portion of the C7 vertebral body.
Pneumatocysts demonstrate generalized hypointensity on both T1- and T2-weighted image acquisition sequences, without associated enhancement on T1 postcontrast gadolinium sequences. This pattern of MR signal characteristics would be similar for a sclerotic lesion, such as a blastic metastasis, a bone island, or possibly intravertebral gas related to avascular necrosis. On CT imaging, pneumatocysts contain uniformly low attenuation, in the range of –580 to –950 Hounsfield units (HU). Given that the MR signal characteristics of pneumatocysts are not pathognomonic for a gas-containing lesion, the characteristic CT findings have proven to be the most useful in diagnosing a pneumatocyst.
Additional patients with vertebral pneumatocysts were as follows:
An 89-year-old woman with a history of dementia who presented to the emergency department with head and neck pain after a fall injury (Figure 2)
A 53-year-old woman involved in a motor vehicle accident who presented with severe neck pain (Figure 3)
A 46-year-old man who had recently been involved in a motor vehicle accident; prior MR examination showed signal abnormality within the C5 vertebral body (Figure 4)
A 43-year-old man with a fall injury after a seizure (Figure 5)
Figure 2.

(a) Sagittal and (b) coronal reformatted CT images show a wellmarginated gas-containing focus (arrows) within the C6 vertebral body in the setting of severe cervical spondylosis.
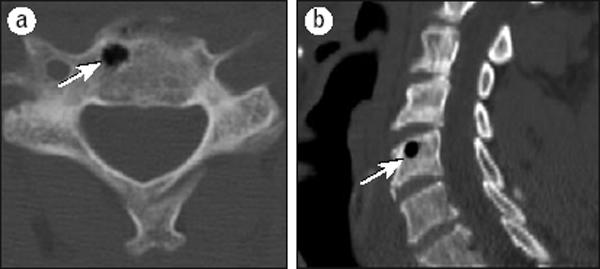
Figure 3.

(a) Sagittal reformatted CT image shows a round, subcentimeter gascontaining lesion (arrow) within the C4 vertebral body with an area of fluid density posterior to the gas-containing lesion. (b) Axial T2-weighted image reveals markedly diminished signal intensity within the right lateral aspect of the C4 vertebral body, with an area of increased signal more posteriorly, corresponding to both gas and dependently layering fluid (arrow). (c) Axial CT image shows a well-circumscribed, subcentimeter gas-containing lesion (arrow) within the C4 vertebral body, with dependent layering fluid.
Figure 4.
(a) Axial and (b) sagittal CT images show a small lucent lesion containing gas density (arrows) within the central portion of the C5 vertebral body.
Figure 5.

(a) Axial and (b) coronal CT images show two small wellmarginated gas-containing foci (arrows) within the ventral aspect of the C7 vertebral body.
CONCLUSION
Vertebral pneumatocysts are benign, gas-containing structures that, based on our anecdotal impression, appear to be underreported in the medical literature and generally poorly understood. When encountered on MR imaging, the pneumatocyst presents a potentially confusing appearance and one that can be indistinguishable from a more ominous lesion such as a blastic metastasis. In such cases, spinal CT will be diagnostic of this benign condition and preclude more exhaustive and unnecessary evaluation, particularly in the cancer patient population. Vertebral pneumatocysts identified in adults are most common in the cervical spine and are typically seen in the setting of spondylosis.
References
- 1.Grunshaw ND, Carey BM. Case report: gas within a cervical vertebral body. Clin Radiol. 1994;49(9):653–654. doi: 10.1016/s0009-9260(05)81887-2. [DOI] [PubMed] [Google Scholar]
- 2.Kamba M, Ohuchi Y, Ogawa T, Ohata R. Intraosseous pneumatocyst of the scapula. Br J Radiol. 2000;73(870):658–660. doi: 10.1259/bjr.73.870.10911791. [DOI] [PubMed] [Google Scholar]
- 3.Karasick D, Eason MA. Vertebral pneumatocyst mimicking susceptibility artifact on MR imaging. AJR Am J Roentgenol. 1998;170(1):221. doi: 10.2214/ajr.170.1.9423641. [DOI] [PubMed] [Google Scholar]
- 4.Laufer L, Schulman H, Hertzanu Y. Vertebral pneumatocyst: a case report. Spine. 1996;21(3):389–391. doi: 10.1097/00007632-199602010-00028. [DOI] [PubMed] [Google Scholar]
- 5.Miller TT, Hermann G, Abdelwahab IF. Intraosseous pneumatocyst of the ilium: CT findings. J Comput Assist Tomogr. 1992;16(6):1002–1003. doi: 10.1097/00004728-199211000-00037. [DOI] [PubMed] [Google Scholar]
- 6.Monu JU, Crotty JM, Pope TL., Jr Intraosseous pneumatocyst of the iliac bone. Clin Orthop Relat Res. 1996;(330):190–192. doi: 10.1097/00003086-199609000-00024. [DOI] [PubMed] [Google Scholar]
- 7.Yamamoto T, Yoshiya S, Kurosaka M, Nagira K, Takabatake M, Hamamoto H, Mineo K. Natural course of an intraosseous pneumatocyst of the cervical spine. AJR Am J Roentgenol. 2002;179(3):667–669. doi: 10.2214/ajr.179.3.1790667. [DOI] [PubMed] [Google Scholar]