

Abstract
The clinical presentation of the bronchogenic cyst is variable, from respiratory distress at birth to late appearance of symptoms. In order to determine clinical features and treatments, we retrospectively studied the medical records and pathology reports of all patients with bronchogenic cysts (n = 22) referred to our surgical department from February 1985 through January 2002. They included 18 male and 4 female patients with an age range of 1 to 38 years (average, 16.4 years). There were 14 mediastinal, 2 hilar, and 6 intrapulmonary bronchogenic cysts. Symptoms were present in 18 of the 22 patients. Cough was the most common symptom (45%). Ten patients (45%) presented with complications: severe hemoptysis, pneumothorax and pleuritis, esophageal compression, infected cyst, and postobstructive pneumonia.
In all patients, complete resection of the bronchogenic cyst was performed by thoracotomy. A postoperative sequela occurred in only 1 patient, who had a persistent air leak. There were no late sequelae, nor was there a recurrence of the cyst. The follow-up period ranged from 8 months to 12 years (mean, 5.2 years).
Because a confident preoperative diagnosis is not always possible and because complications are common, we recommend surgical resection of all suspected bronchogenic cysts in operable candidates. (Tex Heart Inst J 2003;30:105–8)
Key words: Bronchogenic cyst/surgery, bronchial diseases/surgery, cysts/surgery, mediastinal neoplasms/surgery
Congenital bronchogenic cysts are observed not only in infants and children, but also in adults. Although some bronchogenic cysts are asymptomatic, even these can eventually threaten life by producing compression, infection, hemorrhage, and rupture. The objectives of this retrospective study were to review the clinical presentations and treatment of bronchogenic cysts.
Patients
Over a 17-year period (February 1985 through January 2002), 22 patients with bronchogenic congenital cysts were treated at the Department of Thoracic Surgery, Akdeniz University. They comprised 18 male and 4 female patients, with an age range of 1 to 38 years (average, 16.4 years).
We reviewed the case records for symptoms, surgical therapy, and outcomes (Table I). The initial diagnostic evaluation had included plain radiography, computed tomography, and bronchoscopy. Follow-up had been performed by direct and indirect patient contact.
TABLE I. Clinical Presentation and Treatment of 22 Patients Who Presented with Bronchogenic Cyst from February 1985 through January 2002, Listed in Order of Chronology

We classified the location of the bronchogenic cysts in accordance with Maier's system. 1 Most of the cysts (14 out of 22) were found in the mediastinum: 6 of these were carinal, 5 paratracheal, and 3 paraesophageal. In addition, 6 cysts were intrapulmonary and 2 hilar. Four of the intrapulmonary lesions were located in upper lobes.
Results
Clinical Presentations
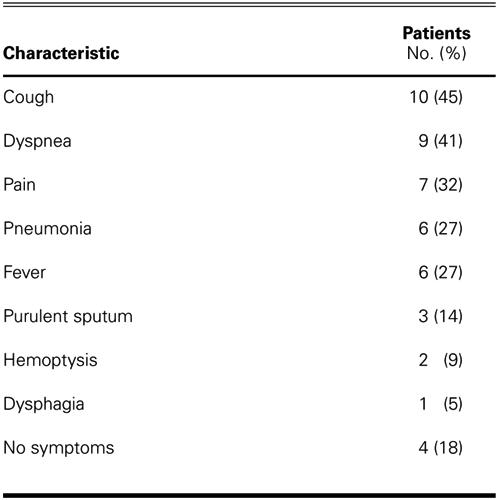
Symptoms were present in 18 patients (82%). Cough was the most common symptom, and it occurred in 10 patients (45%). Other symptoms are listed in Table I and summarized in Table II. Several patients had more than 1 symptom.
TABLE II. Summary of Symptoms and Signs in 22 Patients
Complications of bronchogenic cysts occurred in 10 patients (45%). In 1 patient (Patient 13), a ruptured, infected, parenchymal, bronchogenic cyst caused pleuritis and pneumothorax (Fig. 1). Three patients with intrapulmonary bronchogenic cyst presented with purulent sputum. A 21-year-old patient (Patient 12), who presented with severe hemoptysis, had a fistula between a bronchogenic cyst and the left upper bronchus. Esophageal compression resulting in dysphagia occurred in 1 patient. Compression of bronchus was seen in 4 patients. In 1 of these patients (Patient 6), a cyst, which originated from the right main bronchus, compressed the left main bronchus. Postobstructive pneumonia developed in 3 patients.
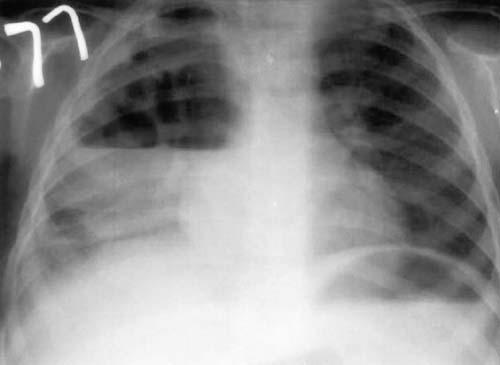
Fig. 1 Patient 13: Complications of bronchogenic cyst. Chest radiograph shows pneumothorax and pleuritis, which were caused by a ruptured and infected parenchymal bronchogenic cyst.
Standard chest radiographs revealed the cyst in 18 patients (82%). The 4 cysts not so revealed lay beneath the tracheal carina. Most of the cysts presented as homogeneous water-density shadows. There were 4 patients with hyperexpanded lungs, 3 with atelectasis, 2 with hydropneumothorax, and 2 with air-fluid levels that were apparent upon plain radiography. Barium swallows performed in 3 patients showed slight indentation of the esophageal image in 2 of the 3. Computed tomography (CT) was performed in 12 patients. The radiographic characteristics of the bronchogenic cyst were those of a round, well circumscribed, unilocular or multilocular mass, with density ranging from that of water to high density.
Bronchoscopy was performed in all 22 patients. Five patients had an extrinsic compression of the tracheobronchial tree. In 2 of these patients, purulent material was seen coming from the upper lobe. One patient with hemoptysis (Patient 12) had bronchoscopic evidence of a direct communication from a residual bronchogenic cyst to the left upper bronchus, and blood clots were seen coming from the cyst. This patient had undergone an incomplete excision of a hilar bronchogenic cyst in another institution. Six months later, he presented at our institution with a bronchopleural fistula and pleuritis.
Treatment
In all patients, complete resection of the bronchogenic cyst was performed via right (n=14) or left (n=8) thoracotomy. In the 6 patients with intrapulmonary cysts, pulmonary resection was required. Wedge excision (n=3) and lobectomy (n=3) were performed to enable complete removal of the bronchogenic cysts. Patient 12, who had a residual bronchogenic cyst to the left upper bronchus, underwent successful resection of the cyst and closure of the bronchial fistula. Patient 13, who had a ruptured and infected bronchogenic cyst, underwent decortication, right upper lobectomy, and drainage of the empyema.
A postoperative sequela occurred only in Patient 13, who had a persistent air leak. Two patients (Patients 4 and 10) were lost to follow-up. To the best of our knowledge, there were no late sequelae, nor did a cyst recur. The follow-up period ranged from 8 months to 12 years (mean, 5.2 years).
Discussion
Bronchogenic cysts are lesions of congenital origin derived from the primitive foregut 2 and are the most common primary cysts of the mediastinum. Most frequently unilocular, they contain clear fluid or, less commonly, hemorrhagic secretions or air. 3 They are lined by columnar ciliated epithelium, and their walls often contain cartilage and bronchial mucous glands. 4,5 It is unusual for them to have a patent connection with the airway, but when present, such a communication may promote infection of the cyst by allowing bacterial entry.
Most bronchogenic cysts originate in the mediastinum, while 15% to 20% occur in the lung parenchyma, 4–6 a statistic roughly in agreement with our series. According to the literature, most intrapulmonary cysts occur in the lower lobes. 4,6 But in our series, 4 of the 6 intrapulmonary cysts were in the upper lobe. They can occur in many atypical locations, ranging from the neck to the spinal dura mater, to below the diaphragm. 3,6,7
Although some bronchogenic cysts are asymptomatic and are incidental findings upon radiography, most cysts are symptomatic—and complications are more common in symptomatic patients. The most frequent symptoms are cough, fever, pain, and dyspnea. 4–8 Tracheobronchial compression and pulmonary infections can occur in children because of the relatively soft tracheobronchial tree. 6–8 In our series, 81% of patients were symptomatic.
Complications of bronchogenic cyst are frequent (45% in our series). Most of the complications result from compression of adjacent structures. Infection is a common complication, especially in cysts with bronchial communications. The cyst can rupture into the trachea, the pericardial cavity, or the pleural cavity, 6 as it did in one of our patients. Pneumothorax is not a rare complication 2,6 and is usually accompanied by pleuritis. Severe hemoptysis is rarely reported. 6,9
Chest radiographs and CT scans are the most valuable diagnostic studies. Bronchogenic cysts appear as spherical or oval masses with smooth outlines and are usually unilocular and noncalcified. 5,6 Computed tomography is valuable in demonstrating the size and shape of the cyst and in determining its position in relation to other structures. The fluid in these cysts has an average CT density of 0 Hounsfield units. 5,6 Bronchogenic cysts can in fact mimic hydatid cysts. However, the CT density reading may be higher, comparable to that of soft tissue, which can create other problems in diagnosis. 3 Also, the cysts may have an air/fluid level that is visible upon radiography. Occasionally, pneumonitis, pneumothorax, or empyema is apparent, as in our series.
The differential diagnosis of the parenchymal form includes lung abscess, hydatidosis, fungal disease, tuberculosis, infected bullas, vascular malformations, and neoplasms. 6 Because hydatid cysts are common in our region, hydatidosis is to us the most important differential diagnosis. Despite the value of various noninvasive diagnostic studies, definitive diagnosis is established only by surgical excision and tissue biopsy. We think that early surgical intervention is needed for precisely that reason.
Complete extirpation, with ligation of the point of attachment to the patent bronchus, is usually possible. The prognosis after complete excision is excellent in all patients. 2–6,8 In patients with pulmonary lesions, lobectomy may be necessary. Incomplete excision will lead to a high recurrence rate and to the potential for more serious sequelae, 6 as in our patient who had undergone incomplete excision elsewhere. Transtracheal and percutaneous cyst aspirations have been proposed as alternatives to operation, but these methods are not widely accepted because of possible cyst recurrence, which carries a substantial morbidity rate. 4,6 In light of the above-mentioned arguments, we conclude that a definitive diagnosis is not always possible preoperatively, and we recommend surgical resection of all suspected bronchogenic cysts in operable candidates.
Footnotes
Address for reprints: Alpay Sarper, MD, Akdeniz Universitesi Tip Fak, Gogus Cerrahisi Anabilim Dali, (07070) Antalya, Turkey
E-mail: asarper@med.akdeniz.edu.tr
References
- 1.Maier HC. Bronchogenic cysts of the mediastinum. Ann Surg 1948;127:476–502. [DOI] [PMC free article] [PubMed]
- 2.Aktogu S, Yuncu G, Halilcolar H, Ermete S, Buduneli T. Bronchogenic cysts: clinicopathological presentation and treatment. Eur Respir J 1996;9:2017–21. [DOI] [PubMed]
- 3.Rapado F, Bennett JD, Stringfellow JM. Bronchogenic cyst: an unusual cause of lump in the neck. J Laryngol Otol 1998:112;893–4. [DOI] [PubMed]
- 4.St. Georges R, Deslauriers J, Duranceau A, Vaillancourt R, Deschamps C, Beauchamp G, et al. Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg 1991;52:6–13. [DOI] [PubMed]
- 5.Di Lorenzo M, Collin PP, Vaillancourt R, Duranceau A. Bronchogenic cysts. J Pediatr Surg 1989;24:988–91. [DOI] [PubMed]
- 6.Suen HC, Mathisen DJ, Grillo HC, LeBlanc J, McLoud TC, Moncure AC, Hilgenberg AD. Surgical management and radiological characteristics of bronchogenic cysts. Ann Thorac Surg 1993;55:476–81. [DOI] [PubMed]
- 7.Ramenofsky ML, Leape LL, McCauley RG. Bronchogenic cyst. J Pediatr Surg 1979;14:219–24. [DOI] [PubMed]
- 8.Ribet ME, Copin MC, Gosselin BH. Bronchogenic cysts of the lung. Ann Thorac Surg 1996;61:1636–40. [DOI] [PubMed]
- 9.Lardinois D, Gugger M, Ris HB. Bronchogenic cyst of the left lower lobe associated with severe hemoptysis. Eur J Cardiothorac Surg 1999:16;382–3. [DOI] [PubMed]