

Abstract
Phosphodiesterase inhibitors such as milrinone can relieve symptoms and improve hemodynamics in patients with advanced congestive heart failure. We retrospectively evaluated the hemodynamic and clinical outcomes of long-term combination therapy with intravenous milrinone and oral β-blockers in 65 patients with severe congestive heart failure (New York Heart Association class IV function and ejection fraction <25%) refractory to oral medical therapy. Fifty-one patients successfully began β-blocker therapy while on intravenous milrinone. Oral medical therapy was maximized when possible. The mean duration of milrinone treatment in this combination-treatment group was 269 days (range, 14–1,026 days). Functional class improved from IV to II–III with milrinone therapy. Twenty-four such patients tolerated β-blocker up-titration and were successfully weaned from milrinone. Sixteen patients (31%) died while receiving combination therapy; one died of sudden cardiac death (on treatment day 116); the other 15 died of progressive heart failure or other complications. Hospital admissions during the previous 6 months and admissions within 6 months after milrinone initiation stayed the same. Meanwhile, the total number of hospital days decreased from 450 to 380 (a 15.6% reduction), and the mean length of stay decreased by 1.4 days (a 14.7% reduction).
We conclude that 1) milrinone plus β-blocker combination therapy is an effective treatment for heart failure even with β-blocker up-titration, 2) weaning from milrinone may be possible once medications are maximized, 3) patients' functional status improves on the combination regimen, and 4) treatment-related sudden death is relatively infrequent during the combination regimen. (Tex Heart Inst J 2003;30:109–13)
Key words: Adrenergic beta-antagonists; heart failure, congestive; milrinone
Advanced heart failure is an increasingly prevalent problem in cardiology. As the population ages and therapy for coronary artery disease improves, more people are developing advanced congestive heart failure (CHF). The annual mortality rate of patients who have New York Heart Association (NYHA) functional class IV CHF remains high regardless of therapy with digitalis, angiotensin-converting enzyme (ACE) inhibitors, diuretics, and β-blockers. 1 In a growing number of patients, symptoms of NYHA class IV CHF persist despite maximal oral medical management. The estimated mortality rate for such patients would exceed 40% were it not for therapies such as transplantation and support with left ventricular assist devices. In comparison, the recent COPERNICUS trial 2 revealed an annual mortality rate of 19.7% for its control patients (a somewhat healthier patient population [NYHA class III–IV]) who received oral medical therapy; other studies have found mortality rates of >30% in patients treated with various inotropic agents. 3–6
Inotropic drug therapy for patients who have advanced heart failure has been shown to increase cardiac output, reduce preload and afterload, and have life-saving potential. 7 During the past 10 years, the positive inotropic agent and phosphodiesterase III inhibitor milrinone has been used intravenously to treat patients with acute heart failure and as a bridge to transplantation. 3,8,9 More recently, intravenous (IV) milrinone has shown promise as long-term therapy for CHF on an outpatient basis. 3 Milrinone can dramatically improve the functional status of patients with severe heart failure and improve end-organ function. Nonetheless, long-term milrinone administration is controversial. This is due mainly to results of the PROMISE trial, 10 a study from the pre-β-blocker era that showed increased mortality rates for patients treated with large doses of oral milrinone. 10 The PROMISE trial, however, did not evaluate the use of milrinone intravenously, in lower doses, or with β-blockers. Currently, β-blockers are used to treat patients with NYHA class II–IV heart failure. However, hypotension and weakness may occur during the usual 6-week period of up-titration. This is problematic for NYHA class IV patients who are refractory to oral medical management, since their therapeutic options are few and their risk of death may increase without intermittent outpatient inotropic therapy. Therefore, in the present study, we examined whether IV milrinone might sufficiently stabilize and support cardiac function in patients with severe heart failure that is refractory to oral medical therapy during the addition and up-titration of β-blocker therapy.
Patients and Methods
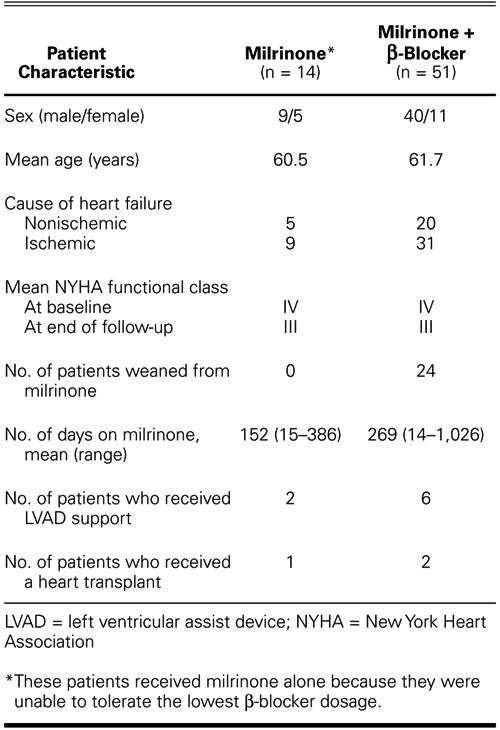
We retrospectively reviewed the cases of 65 patients with severe congestive heart failure (NYHA class IV symptoms) who were treated with continuous IV milrinone and β-blockers on an outpatient basis. The demographics and characteristics of this patient population are shown in Table I. All patients were stabilized in the hospital first with a continuous IV infusion of low-dose milrinone (0.375–0.45 μg/kg per min) and later with β-blockers. A peripherally inserted central catheter was used to administer the milrinone, except in 1 patient who required a subclavian catheter. All patients had been unresponsive to the maximum oral dosages of digitalis, diuretics, and ACE inhibitors and could not be weaned from milrinone while in the hospital. Of these 65 patients, 14 could not tolerate the lowest dose of β-blocker and were sent home without β-blocker therapy. In the 51 patients who tolerated low doses of β-blocker in the hospital, up-titration was implemented on an outpatient basis every 3–4 weeks (more slowly than the standard recommended rate of every 2 weeks). All patients were followed up in a specialized heart failure clinic.
TABLE I. Patient Characteristics by Treatment Regimen (n = 65)
In all cases, early weaning from milrinone during initial hospitalization was attempted but failed; failure was manifested clinically by an increase in symptoms of CHF. Later, weaning was considered for those patients who achieved NYHA class I–II function while on IV milrinone therapy and who tolerated β-blocker up-titration. Weaning consisted of discontinuing milrinone for 12 hours every other day for 1 week and then for 12 hours every day for 1 week. If the patient remained clinically stable, milrinone was discontinued after the 2-week period. If the patient did not remain clinically stable, weaning was implemented more slowly or for fewer hours per day.
Statistical methods are as follows: for all variables, differences between the 2 groups were considered statistically significant if the 2-tailed probability value was <0.05.
Results
According to data from invasive hemodynamic studies in the patient records, all patients treated with IV milrinone showed substantially increased cardiac output. Cardiac output and pulmonary capillary wedge pressure improved at least 20% with IV milrinone. The mean duration of IV milrinone therapy and follow-up was 269 days (range, 14–1,026 days). In 51 of the 65 patients, β-blocker therapy was successfully initiated during IV milrinone therapy. These patients improved from NYHA functional class IV to an average of II–III (Fig. 1). The duration of hospital stay for this group decreased from 450 days during the 6 months before treatment to 380 days during the first 6 months of treatment (a 15.6% reduction) (Fig. 2).

Fig. 1 Improvement in New York Heart Association mean functional class in patients who received milrinone plus β-blocker combination therapy.
*P <0.001 compared with before therapy

Fig. 2 There was a 15.6% decrease in hospital stay (number of days) in the 51 patients who received milrinone plus β-blocker therapy.
Intravenous milrinone therapy did not affect the QTc interval duration, as corrected for heart rate with Bazett's formula, in patients treated with β-blockers (441 ± 30 [SEM] ms before vs 446 ± 29 ms after milrinone initiation; P=0.82) but significantly prolonged it in patients not treated with β-blockers (436 ± 13 ms before vs 469 ± 28 ms after milrinone initiation; P=0.002). Therefore, β-blockade appeared to prevent milrinone-associated QTc interval prolongation in patients with congestive heart failure (Fig. 3).

Fig. 3 The QTc interval duration before therapy compared with milrinone plus β-blocker therapy (n=51) and with milrinone therapy alone (n=14).
*P=0.002
Survival longer than 3 years was 59% higher in the combination treatment group than in the milrinone-only treatment group (P<0.0001) (Fig. 4). Sixteen of 51 patients (31%) died while receiving the combination therapy. One experienced sudden cardiac death (on treatment day 116); the other 15 patients died of progressive heart failure or other medical complications. Four deaths occurred within the first 6 months of combination therapy, and 5 deaths occurred after 1 year.

Fig. 4 Kaplan-Meier survival curves for patients treated with milrinone plus β-blockers (n=51) versus milrinone alone (n=14) (P <0.0001).
Discussion
In a retrospective review, we examined some aspects of the safety and efficacy of long-term therapy with IV milrinone in 65 patients with CHF who were in NYHA class IV. We found that β-blocker therapy could be successfully initiated and up-titrated in some but not all patients and that the mortality rate in our small series was comparable to or better than that in historical controls treated with various inotropic agents, including milrinone. 3,5
The phosphodiesterase inhibitor milrinone is both an inotropic agent and a vasodilator that acts by inhibiting the breakdown of—and thus increasing the level of—intracellular cAMP. Milrinone also increases myocardial contractility without increasing regional myocardial oxygen consumption. 11,12 The hemodynamic effect of milrinone is to increase the cardiac index and to decrease pulmonary artery and pulmonary wedge pressures. 13 However, the effects of milrinone in patients with chronic CHF are impaired by an increased concentration of inhibitory G-protein αsubunits, which is believed to suppress basal cAMP formation. 14–16 The down-regulation of β-receptors and the increase in G-protein α subunits are mediated by the stimulation of adrenergic receptors, which is itself mediated by increased endogenous catechol-amines in chronic heart failure. 17,18 Therefore, adding a β-receptor blocking agent to a phosphodiesterase-III-inhibitor drug regimen may not only increase the β-adrenergic receptor density but also decrease the content of G-protein α subunits in myocytes, thereby increasing the potential effect of the phosphodiesterase III inhibitor. 18–20 In patients with CHF, the contractile response of myocardium to an infusion of milrinone can markedly improve after treatment with metoprolol during a 1-month period. 18 Therefore, the 2 drugs may work synergistically to improve myocardial function.
Intravenous milrinone therapy has been associated with QTc interval prolongation. 21 This effect may explain the increased mortality rates seen with the use of inotropic agents. In our study, the addition of β-blockade to a milrinone regimen was shown to stop QTc interval widening. We measured the mean QT interval from a standard 12-lead electrocardiogram before and after milrinone therapy in patients who were treated with β-blockers and in those who were not. Our findings indicate that IV milrinone with β-blocker therapy can substantially improve functional status in patients with advanced CHF. The 23% mortality rate observed in our series after nearly 1 year of follow-up compares favorably with that observed in other studies of similar patients. Mehra and colleagues 3 reported an annual mortality rate of 30% to 35%, and others 4–6 reported a rate of 36% or more for patients with NYHA class IV heart failure who were treated with various inotropic agents. Moreover, the incidence of sudden cardiac death in our series was low.
Conclusion
There is evidence of a synergistic effect of milrinone and β-blockers in heart failure patients, 18 and the β-blockade in this patient population seems to prevent milrinone-associated QTc interval prolongation. Therefore, combination milrinone and β-blocker treatment appears to offer hope to some patients with NYHA class IV heart failure who have no other treatment options.
In light of the present data, we conclude that milrinone and β-blockers can be used together safely and effectively. As is evident in the Kaplan-Meier curves, survival is significantly better in patients who are able to tolerate β-blockers in addition to milrinone than it is in those treated with milrinone alone. Therefore, the inability of patients on milrinone to tolerate β-blockers can be seen as a bad prognostic sign, and other treatment options (for example, the use of left ventricular assist devices or transplantation) should be explored for such patients. We also conclude that IV milrinone administration followed by β-blocker initiation and up-titration is an important new treatment option that may result in acceptable mortality rates, successful weaning from milrinone in some cases, and a substantially improved quality of life for patients with advanced congestive heart failure.
Footnotes
Address for reprints: Reynolds M. Delgado III, MD, 6624 Fannin, Suite 2420, Houston, TX 77030
E-mail: rdelgado@pol.net
References
- 1.Consensus recommendations for the management of chronic heart failure. On behalf of the membership of the advisory council to improve outcomes nationwide in heart failure. Am J Cardiol 1999;83(2A):1A–38A. [PubMed]
- 2.Ghali JK, Pina IL, Gottlieb SS, Deedwania PC, Wikstrand JC, MERIT-HF Study Group. Metoprolol CR/XL in female patients with heart failure: analysis of the experience in Metoprolol Extended-Release Randomized Intervention Trial in Heart Failure (MERIT-HF). Circulation 2002;105(13):1585–91. [DOI] [PubMed]
- 3.Mehra MR, Ventura HO, Kapoor C, Stapleton DD, Zimmerman D, Smart FW. Safety and clinical utility of long-term intravenous milrinone in advanced heart failure. Am J Cardiol 1997;80:61–4. [DOI] [PubMed]
- 4.Galinier M, Albenque JP, Afchar N, Fourcade J, Massabuau P, Doazan JP, et al. Prognostic value of late potentials in patients with congestive heart failure. Eur Heart J 1996;17:264–71. [DOI] [PubMed]
- 5.Stegmayr BG, Banga R, Lundberg L, Wikdahl AM, Plum-Wirell M. PD treatment for severe congestive heart failure. Perit Dial Int 1996;16(Suppl 1):S231–5. [PubMed]
- 6.Campana C, Gavazzi A, Berzuini C, Larizza C, Marioni R, D'Armini A, et al. Predictors of prognosis in patients awaiting heart transplantation. J Heart Lung Transplant 1993;12:756–65. [PubMed]
- 7.Young JB, Moen EK. Outpatient parenteral inotropic therapy for advanced heart failure. J Heart Lung Transplant 2000;19(8 Suppl):S49–57. [DOI] [PubMed]
- 8.Skoyles JR, Sherry KM, Price C. Intravenous milrinone in patients with severe congestive cardiac failure awaiting heart transplantation. J Cardiothorac Vasc Anesth 1992;6:222–5. [DOI] [PubMed]
- 9.Cesario D, Clark J, Maisel A. Beneficial effects of intermittent home administration of the inotrope/vasodilator milrinone in patients with end-stage congestive heart failure: a preliminary study. Am Heart J 1998;135:121–9. [DOI] [PubMed]
- 10.Packer M, Carver JR, Rodeheffer RJ, Ivanhoe RJ, DiBianco R, Zeldis SM, et al. Effect of oral milrinone on mortality in severe chronic heart failure. The PROMISE Study Research Group. N Engl J Med 1991;325:1468–75. [DOI] [PubMed]
- 11.Jaski BE, Fifer MA, Wright RF, Braunwald E, Colucci WS. Positive inotropic and vasodilator actions of milrinone in patients with severe congestive heart failure. Dose-response relationships and comparison to nitroprusside. J Clin Invest 1985;75:643–9. [DOI] [PMC free article] [PubMed]
- 12.Monrad ES, Baim DS, Smith HS, Lanoue A, Brauwald E, Grossman W. Effects of milrinone on coronary hemodynamics and myocardial energetics in patients with congestive heart failure. Circulation 1985;71:972–9. [DOI] [PubMed]
- 13.Benotti JR, Lesko LJ, McCue JE, Alpert JS. Pharmacokinetics and pharmacodynamics of milrinone in chronic congestive heart failure. Am J Cardiol 1985;56:685–9. [DOI] [PubMed]
- 14.Bohm M. Alteration of beta-adrenoceptor-G-protein-regulated adenyl cyclase in heart failure. Mol Cell Biochem 1995;147:147–60. [PubMed]
- 15.Bohm M, Gierschik P, Jakobs KH, Pieske B, Schnabel P, Ungerer M, Erdmann E. Increase of Gi alpha in human hearts with dilated but not ischemic cardiomyopathy. Circulation 1990;82:1249–65. [DOI] [PubMed]
- 16.Neumann J, Schmitz W, Scholz H, von Meyerinck L, Doring V, Kalmar P. Increase in myocardial Gi-proteins in heart failure. Lancet 1988;2:936–7. [DOI] [PubMed]
- 17.Reithmann C, Gierschik P, Sidiropoulos D, Werdan K, Jakobs KH. Mechanism of noradrenaline-induced heterologous desensitization of adenylate cyclase stimulation in rat heart muscle cells: Increase in the level of inhibitory G-protein alpha-subunits. Eur J Pharmacol 1989;172:211–21. [DOI] [PubMed]
- 18.Bohm M, Deutsch HJ, Hartmann D, Rosee KL, Stablein A. Improvement of postreceptor events by metoprolol treatment in patients with chronic heart failure. J Am Coll Cardiol 1997;30:992–6. [DOI] [PubMed]
- 19.Heilbrunn SM, Shah P, Bristow MR, Valantine HA, Ginsburg R, Fowler MB. Increased beta-receptor density and improved hemodynamic response to catecholamine stimulation during long-term metoprolol therapy in heart failure from dilated cardiomyopathy. Circulation 1989;79:483–90. [DOI] [PubMed]
- 20.Gilbert EM, Olsen SL, Renlund DG, Bristow MR. beta-adrenergic receptor regulation and left ventricular function in idiopathic dilated cardiomyopathy. Am J Cardiol 1993;71:23C–29C. [DOI] [PubMed]
- 21.Goldstein RA, Geraci SA, Gray EL, Rinkenberger RL, Dougherty AH, Naccarelli GV. Electrophysiologic effects of milrinone in patients with congestive heart failure. Am J Cardiol 1986;57:624–8. [DOI] [PubMed]