

Abstract
The extracranial segment of the vertebral artery is well protected, and the rate of occurrence of extracranial vertebral aneurysms is very low. We describe the case of a 40-year-old woman who presented with a large aneurysm of the left vertebral artery in the angiographic absence of a right vertebral artery. Her medical history included a motorcycle accident at the age of 20, at which time a neck sprain had been diagnosed. Computed tomography of the chest and neck revealed a 6- × 4-cm aneurysm with mural thrombus in the left thoracic outlet and in the first portion of the left vertebral artery before the entrance of the transverse foramen of the 6th cervical vertebra. Angiography of the arch vessels confirmed both the presence of an aneurysm of the left vertebral artery and the absence of a right vertebral artery. Due to the lack of contralateral vertebral flow, we planned to perform a graft interposition under deep hypothermic circulatory arrest, for cerebral protection. Unfortunately, the patient refused the operation and was lost to follow-up.
To our knowledge, there has been no previous report of an extracranial vertebral artery aneurysm in the absence of a contralateral vertebral artery. We believe that deep hypothermic circulatory arrest with graft interposition is the best treatment strategy, although we did not, in this case, have opportunity to treat the patient. (Tex Heart Inst J 2003;30:134–6)
Key words: Aneurysm/radiography; aneurysm, dissecting/radiography; congenital heart disease; tomography, x-ray computed; vertebral artery/radiography; wounds, nonpenetrating
Extracranial aneurysms of the vertebral artery are rare, and the most common cause is trauma. Unilateral surgical occlusion of this aneurysm in the presence of a normal contralateral vertebral artery is well tolerated. 1 We describe a case involving a patient who presented with a large aneurysm of the left vertebral artery in the angiographic absence of a right vertebral artery. In this report, we hypothesize on the possible cause and describe a potential operative strategy.
Case Report
In March 2002, a 40-year-old woman presented at our hospital with a pulsatile mass at the base of her neck, on the left side. She reported that the mass had been present, and growing slowly, for the past 3 years. Her medical history included a motorcycle accident at the age of 20, at which time a neck sprain had been diagnosed. The physical examination revealed a 2- × 3-cm, non-tender, pulsatile mass at the base of the neck. Radiography revealed no bony lesion of the cervical vertebrae. The computed tomographic (CT) scan of chest and neck revealed a 6- × 4-cm aneurysm with mural thrombus in the left thoracic outlet and in the 1st portion of the left vertebral artery before the entrance of the transverse foramen of the 6th cervical vertebra (Figs. 1 and 2). A 3-dimensional CT scan showed a fusiform aneurysm of the left vertebral artery arising from the left subclavian artery (Fig. 3). Angiography of the arch vessels confirmed both the presence of an aneurysm of the left vertebral artery (Fig. 4) and the absence of a right vertebral artery.

Fig. 1 Computed tomographic scan of the chest and neck (sagittal view) shows the vertebral aneurysm (A) in the thoracic outlet and in the 1st portion of the left vertebral artery before the entrance of the transverse foramen (arrow) of the 6th cervical vertebra.

Fig. 2 Computed tomographic scan of the chest and neck (coronal view) reveals a 4- × 6-cm aneurysm with mural thrombus. The arrow indicates the transverse foramen of the 6th cervical vertebra, and A indicates the aneurysm.

Fig. 3 Three-dimensional computed tomographic scan shows the vertebral aneurysm arising from the left subclavian artery.
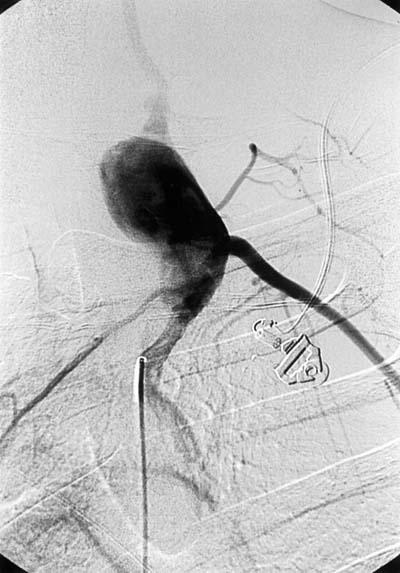
Fig. 4 Left subclavian arteriography shows the fusiform aneurysm of the left vertebral artery.
Upon observing the single arterial supply to the basilar system of the brain, we realized that simple ligation or surgery with direct clamping could cause vertebrobasilar ischemia. Therefore, we planned a graft interposition under deep hypothermic circulatory arrest, for cerebral protection. Unfortunately, the patient refused the operation and was lost to follow-up.
Discussion
The extracranial segment of the vertebral artery is well protected, and the rate of occurrence of extracranial vertebral aneurysms is very low. To our knowledge, there has been no previous report of an extracranial vertebral artery aneurysm in the absence of a contralateral vertebral artery. Extracranial vertebral aneurysms are caused chiefly by penetrating wounds to the neck, most commonly gunshot or stab wounds. 2 In addition, nonpenetrating diseases and conditions—such as atherosclerosis, syphilis, rheumatoid arthritis, and vertebral fracture—have been reported as causal factors. 3 In our patient, it is possible that a simple intimal injury of the vertebral artery during the motorcycle accident was the origin. Regional arterial dissection secondary to that intimal injury could have progressed to a fusiform vertebral aneurysm. 4
Angiography is generally considered the gold standard for determining the extent of a vertebral aneurysm and the patency of the contralateral vertebral artery. However, a specific diagnosis of aneurysm can be made on an angiographic basis alone in only 50% of patients. 5 Computed tomographic scanning and magnetic resonance imaging are important aides to diagnosis when angiography provides insufficient information. 2
Treatment options for vertebral aneurysm include resection of the aneurysm with ligation, direct repair of the vertebral artery, and therapeutic embolization. 2 Ligation of the vertebral artery has been the most commonly adopted strategy, and unilateral occlusion in the presence of a normal contralateral vertebral artery has been well tolerated. 1 The incidence of neurologic complications after ligation has been reported to be as high as 8%, 6 and it appears that the risk of neurologic deficits is higher in patients who lack blood flow in the contralateral vertebral artery. The incidence of congenital atresia or hypoplasia of the left vertebral artery is 3.1%, and of the right vertebral artery it is 1.8%; reconstruction of the aneurysmal segment should be considered in these patients, as it was in ours.
In repairing or resecting difficult aneurysms of vessels that supply the brain, there are methods of reducing neurologic risk. Profound hypothermia and circulatory arrest—the most common adjunct to surgical repair of large intracranial aneurysms that would otherwise be inoperable 7—provides a bloodless field and protection from cerebral ischemia. Another technique is the external carotid—posterior cerebral artery bypass before aneurysmectomy, 8 but that procedure requires another incision and an autogenous conduit to restore blood flow. In order to avoid a craniotomy to achieve bypass in the absence of a contralateral vertebral artery, we had planned to use deep hypothermic circulatory arrest during the restoration of arterial continuity. Although our patient refused surgery and was lost to follow-up, we strongly believe that this strategy would have been the best for her difficult situation.
In conclusion, a large, fusiform vertebral aneurysm in the absence of a contralateral vertebral artery is an extremely rare condition, and difficult to treat. Deep hypothermic circulatory arrest with a graft interposition is in our judgment the strategy that best combines safety and effectiveness.
Footnotes
Address for reprints: Jen-Ping Chang, MD, Division of Thoracic and Cardiovascular Surgery, Chang Gung Memorial Hospital at Kaohsiung, 123 Ta-Pei Rd., Niao Sung Hsiang, Kaohsiung Hsien, Taiwan, R.O.C.
E-mail: c9112772@adm.cgmh.org.tw
References
- 1.Amaral JF, Grigoriev VE, Dorfman GS, Carney WI Jr. Vertebral artery pseudoaneurysm. A rare complication of subclavian artery catheterization. Arch Surg 1990;125:546–7. [DOI] [PubMed]
- 2.Anand VK, Raila FA, McAuley JR, Reed JM. Large pseudoaneurysm of the extracranial vertebral artery. Otolaryngol Head Neck Surg 1993;109:1057–60. [DOI] [PubMed]
- 3.Sumimura J, Nakao K, Miyata M, Kamiike W, Yokota H, Kawashima Y. Vertebral aneurysm of the neck. J Cardiovasc Surg (Torino) 1988;29:63–5. [PubMed]
- 4.Yasui T, Komiyama M, Nishikawa M, Nakajima H, Kobayashi Y, Inoue T. Fusiform vertebral artery aneurysms as a cause of dissecting aneurysms. Report of two autopsy cases and a review of the literature. J Neurosurg 1999;91:139–44. [DOI] [PubMed]
- 5.Reid JD, Weigelt JA. Forty-three cases of vertebral artery trauma. J Trauma 1988;28:1007–12. [DOI] [PubMed]
- 6.Blickenstaff KL, Weaver FA, Yellin AE, Stain SC, Finck E. Trends in the management of traumatic vertebral artery injuries. Am J Surg 1989;158:101–6. [DOI] [PubMed]
- 7.Chyatte D, Elefteriades J, Kim B. Profound hypothermia and circulatory arrest for aneurysm surgery. Case report. J Neurosurg 1989;70:489–91. [DOI] [PubMed]
- 8.Wakui K, Kobayashi S, Takemae T, Kamijoh Y, Nagashima H, Muraoka S. Large thrombosed vertebral artery aneurysm managed with extracranial-intracranial bypass surgery and aneurysmectomy. Case report. J Neurosurg 1992;77:624–7. [DOI] [PubMed]