

Abstract
A 30-year-old man had multiple pellet injuries after being shot. An asymptomatic, acute, inferior-wall myocardial infarction was detected on an electrocardiogram at the time of a pre-anesthetic evaluation for eye surgery. A computed tomographic scan of the chest confirmed the presence of an intracardiac foreign body. Coronary angiography showed occlusion of the distal right coronary artery by a pellet. The patient was managed conservatively with aspirin and metoprolol.
In conclusion, a single coronary lesion, the absence of other cardiac complications, and a favorable outcome with conservative medical treatment after a gunshot injury contribute to the rarity of this case of myocardial infarction. (Tex Heart Inst J 2003;30:158–60)
Key words: Coronary vessels/injuries; foreign bodies/diagnosis; heart injuries/diagnosis; myocardial infarction, etiology; wounds, gunshot/complications; wounds, penetrating/diagnosis
Cardiac trauma can be caused by either penetrating or nonpenetrating injuries. Common cardiac results of such injuries include myocardial rupture, contusion, laceration, pericardial insult, coronary injury, valvular damage, arrhythmias, and conduction abnormalities. 1 The most frequently seen penetrating injuries are stab or gunshot wounds. We report a case of uncomplicated, acute, inferior-wall myocardial infarction after an injury by gunshot.
Case Report
In May 1998, a 30-year-old man was brought to the emergency room with multiple pellet injuries in the chest and face after being shot. At the time of admission, he did not mention any chest pain that would have suggested myocardial infarction. He was hemodynamically stable. The cardiovascular examination showed nothing unusual. During his pre-anesthetic examination for an eye injury, performed 48 hours after the accident, an electrocardiogram showed changes indicating an acute inferior-wall myocardial infarction. Chest radiography showed multiple pellets in the chest, including one in the cardiac silhouette (Fig. 1) Two-dimensional echocardiography showed inferior-wall hypokinesia. There was no pericardial effusion. A computed tomographic scan of the chest confirmed the presence of an intracardiac foreign body (Fig. 2). Elective coronary angiography showed complete occlusion of the distal right coronary artery (RCA) by a 2- × 2-mm pellet embedded in the heart. The pellet was moving in accordance with the RCA motion (Fig. 3). There was a thrombus in the RCA proximal to the occlusion. The distal RCA was filling through collateral vessels from the left coronary artery (Fig. 4). A left ventriculogram showed inferior-wall hypokinesia (Fig. 5). The patient was managed conservatively with aspirin, 150 mg per day, and metoprolol, 50 mg, twice a day. At the 6-month follow-up, he was asymptomatic and underwent an uneventful treadmill stress test. He remained asymptomatic when last seen in May 2002.

Fig. 1 A chest radiograph shows multiple pellets in the chest, including one in the cardiac silhouette.

Fig. 2 A computed tomographic scan of the chest shows an intracardiac foreign body.

Fig. 3 A right coronary angiogram in A) diastole and B) systole shows total occlusion of the right coronary artery with a thrombus at the site of occlusion.
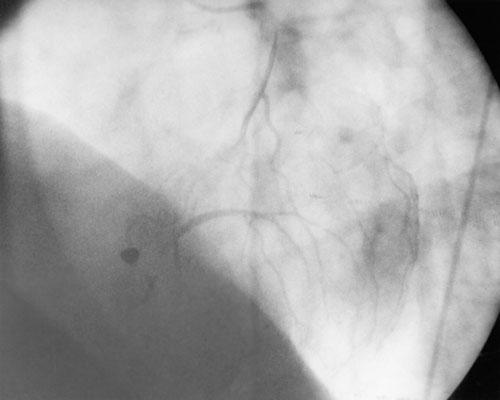
Fig. 4 A left coronary angiogram shows filling of the distal right coronary artery through collateral vessels.

Fig. 5 A left ventricular angiogram in A) diastole and B) systole shows inferior-wall hypokinesia with normal left ventricular contractility.
Discussion
The clinical presentation of a penetrating cardiac injury depends on several factors, such as the type of object, size of the wound, structures damaged, the presence of pericardial tamponade, and associated noncardiac injuries. Our patient had total occlusion of the distal RCA by a shotgun pellet, which caused an uncomplicated inferior-wall myocardial infarction. He was successfully managed with conservative medical treatment. Various complications, such as laceration of the coronary artery, hemopericardium, 2 coronary arteriovenous fistula, 3 cardiac perforation, 4 and pellet embolization, 5 have been reported after gunshot injury of a coronary artery. Despite the fact that a pellet had become embedded in the heart and was occluding the RCA, our patient had an uneventful recovery. Only 1 similar case has been reported in the world medical literature; that patient also had an uneventful recovery after RCA occlusion by a shotgun pellet. 6
Footnotes
Address for reprints: Dr. H.K. Bali, Additional Professor, Department of Cardiology, PGIMER, Chandigarh – 160012, India
E-mail: hkbali_pgi@rediffmail.com
References
- 1.Olsovsky MR, Wechsler AS, Topaz O. Cardiac trauma. Diagnosis, management, and current therapy. Angiology 1997;48:423–32. [DOI] [PubMed]
- 2.Doetsch N, Wolfhard U, Mathers MJ, Zerkowski HR. Survival after heart and coronary-artery penetration by an air-rifle projectile. Thorac Cardiovasc Surg 1989;37:332–4. [DOI] [PubMed]
- 3.Mukherjee DK, Banka VS, Keosathit N, Helfant RH. Penetrating injury of the chest and coronary arteriovenous fistula. Chest 1976;69:793–5. [DOI] [PubMed]
- 4.Biocina B, Sutlic Z, Husedzinovic I, Rudez I, Ugljen R, Letica D, et al. Penetrating cardiothoracic war wounds. Eur J Cardiothorac Surg 1997;11:399–405. [DOI] [PubMed]
- 5.Hopkins HR, Pecirep DP. Bullet embolization to a coronary artery. Ann Thorac Surg 1993;56:370–2. [DOI] [PubMed]
- 6.De Meester A, Six C, Henin P, Scavee C, Luwart R, Chaudron JM. Traumatic myocardial infarction caused by lead shot [in French]. Arch Mal Coeur Vaiss 1996;89:1673–6. [PubMed]