

Abstract
Background
The medical specialities chosen by doctors for their careers play an important part in the development of health-care services. This study aimed to investigate the influence of gender, personality traits, career motivation and life goal aspirations on the choice of medical speciality.
Methods
As part of a prospective cohort study of Swiss medical school graduates on career development, 522 fourth-year residents were asked in what speciality they wanted to qualify. They also assessed their career motivation and life goal aspirations. Data concerning personality traits such as sense of coherence, self-esteem, and gender role orientation were collected at the first assessment, four years earlier, in their final year of medical school. Data analyses were conducted by univariate and multivariate analyses of variance and covariance.
Results
In their fourth year of residency 439 (84.1%) participants had made their speciality choice. Of these, 45 (8.6%) subjects aspired to primary care, 126 (24.1%) to internal medicine, 68 (13.0%) to surgical specialities, 31 (5.9%) to gynaecology & obstetrics (G&O), 40 (7.7%) to anaesthesiology/intensive care, 44 (8.4%) to paediatrics, 25 (4.8%) to psychiatry and 60 (11.5%) to other specialities. Female residents tended to choose G&O, paediatrics, and anaesthesiology, males more often surgical specialities; the other specialities did not show gender-relevant differences of frequency distribution. Gender had the strongest significant influence on speciality choice, followed by career motivation, personality traits, and life goals. Multivariate analyses of covariance indicated that career motivation and life goals mediated the influence of personality on career choice. Personality traits were no longer significant after controlling for career motivation and life goals as covariates. The effect of gender remained significant after controlling for personality traits, career motivation and life goals.
Conclusion
Gender had the greatest impact on speciality and career choice, but there were also two other relevant influencing factors, namely career motivation and life goals. Senior physicians mentoring junior physicians should pay special attention to these aspects. Motivational guidance throughout medical training should not only focus on the professional career but also consider the personal life goals of those being mentored.
Background
The medical specialties chosen by doctors for their careers play an important role in the development of health-care services. There are some recent studies of how different medical specialities are perceived or how choices are made [1-3]. Several determinants have been identified: the feminisation of medicine, lifestyle, specialist status and the prospect of future income, as well as the structural conditions of the various residency programmes. Most studies addressed medical students, not residents. As far as we know there appear to be only a few studies on personality traits, career motivation and personal life goals as influencing factors on speciality choice [4].
Feminisation
Since the 1990s, more than half of the medical school graduates in Western countries have been women [5-8]. Although female physicians tend to specialise almost to the same degree, they enter other specialties than their male colleagues [9-12]. Especially in surgical specialities, female physicians are under-represented [13]. Gender differences in speciality choice can partly be explained as a function of socialisation [14-16], but also by structural operating barriers or closure mechanisms within specific fields [17-19].
Lifestyle
Several studies have reported that a so-called controllable lifestyle has become a determinant in physicians' speciality selection criteria [3,20-22]. The following characteristics of a controllable lifestyle have been defined: personal time free of practice requirements for leisure, family, and non-vocational pursuits and control of total weekly hours spent on professional responsibilities. For female physicians the prospect of combining their professional career with family responsibilities is a key issue in the process of speciality choice or changing the speciality to which they initially aspired to [16].
Status and income
Prestige within the medical profession, social status and income also play their role in the decision in favour of a medical speciality [23,24]. In some studies, students reported their student debt as one of the factors influencing their career choices [25,26]. Students with large debts tended to choose surgical specialities more often and were less likely to choose primary care.
Residency programmes
The application and selection procedures for residency programmes, the length, quality and structure of the programme, work schedules, mentorship, annual vacations are also factors which are considered when choosing a speciality [18,19,24,27,28].
Most studies investigated only one or two of the factors identified as influencing speciality choice. One has to consider, however, that Swiss studies addressing issues of speciality choice are lacking to date.
The aims of this study were to investigate (1) the development of the residents' speciality choices since graduating from medical school, and the differences compared to the speciality distribution of working doctors, and (2) what factors influence the young doctors' speciality choices. As shown in Figure 1, we hypothesised that gender and personality traits have an impact on speciality choice, and that career motivation as well as life goals have an influence, too. The present paper aimed to examine these hypotheses.
Figure 1.
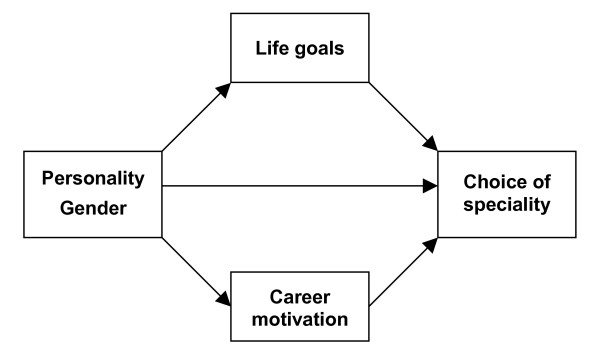
Conceptual framework of the study.
Methods
Study design, sample development, and study sample
The present study is part of an ongoing prospective survey of a cohort of graduates of the three medical schools in German speaking Switzerland, beginning in 2001 (T1). Of the 1004 registered final-year students, 715 (71%) participated in the first assessment (T1, in 2001) [15]. Subjects were re-evaluated after two years in 2003 (T2) [18,19]. The present paper refers to results of the third assessment (T3), conducted in the fourth year of residency (in 2005). Table 1 shows the sample development from T0 (questionnaires sent to all registered graduates at the medical schools of Basel, Bern, and Zurich) to T1, T2, and T3 for participants, non-participants and dropouts. There are no significant differences between the 193 dropouts (T1 – T3) and the 522 subjects participating at the third measurement with regard to socio-demographic data, personality traits, and career-related variables at T1.
Table 1.
Development of the study sample
| Sample addressed T0(2001) n (%) |
Non-participants n (%) |
Study sample T1(2001) n (%) |
Drop-outs T1 – T2 n (%) |
Study sample T2(2003) n (%) |
Drop-outs T1 – T3 n (%) |
Study sample T3(2005) n (%) |
|
| Gender | |||||||
| female | 487 (49) | 108 (37) | 379 (53) | 96 (50) | 283 (54) | 98 (51) | 281 (54) |
| male | 517 (51) | 181 (63) | 336 (47) | 97 (50) | 239 (46) | 95 (49) | 241 (46) |
| Age in years | |||||||
| mean | 27.4 | 27.6 | 29.3 | 31.5 | 31.3 | ||
| range | 23 – 44 | 23 – 44 | 26 – 44 | 29 – 48 | 27 – 46 | ||
| Total | 1004 | 289 | 715 | 193 | 522 | 193 | 522 |
| Study sample |
715 (100%) (71% of 1004) |
522 (73% of 715) (52% of 1004) |
522 (73% of 715) (52% of 1004) |
||||
Of these 522 residents there were 281 females (53.8%) and 241 males (46.2%). The mean age was 31.3 years (SD 2.4 y, range 27 – 46 y). Of the residents 428 (82.0%) had a stable partnership, of whom 125 were married (65 females and 60 males). Only 26 (9.3%) of the females, but 36 (14.9%) of the males had own children (p = 0.03). 94.7% worked full-time, 5.3% part-time. The mean working hours per week were 55.4 hrs (SD 8.2 hrs, range 30 – 80 hrs).
Speciality training and residencies in Switzerland
There are 43 registered speciality qualifications in Switzerland. Most of the specialities require at least a six-year residency, and a final speciality qualification exam. One major problem with most of the speciality training courses is the lack of structured and time-limited residency programmes. Young doctors usually only get contracts for a year, i.e. they have to arrange and organize their residency posts every one to two years.
Instruments
The main characteristics of the applied instruments are given in Table 2. All instruments are self-assessment scales. In the following, it is described what constructs are measured by the instruments:
Table 2.
Characteristics of the applied instruments
|
Dimensions and scales |
Number of items | Method of item scoring (Likert-scales) | Method of scale scoring | Reference value (mean) female | Reference value (mean) male | Reliability | Reliability in this study | Stability in this study T1 – T3 |
| Personality factors (T1) | ||||||||
| Sense of coherence (SOC) | 13 | 1 (low) – 7 (high) | Sum score divided by number of items | 4.96 | 5.18 | 0.85 | 0.84 | 0.56 |
| Rosenberg Self-esteem | 10 | 1 (low) – 4 (high) | Sum score/number of items | 2.23 | 2.31 | 0.88 | 0.85 | |
| 1PAQ Instrumentality | 8 | 1 (low) – 6 (high) | Sum score/number of items | 3.50 | 3.75 | 0.72 | 0.74 | |
| 1PAQ Expressiveness | 8 | 1 (low) – 6 (high) | Sum score/number of items | 4.63 | 4.38 | 0.75 | 0.74 | |
| Career-related factors (T3) | ||||||||
| 2CMQ Intrinsic career motivation | 8 | 1 (low) – 7 (high) | Sum score/number of items | 5.96 | 0.70 | 0.68 | 0.57 | |
| 2CMQ Extrinsic career motivation | 8 | 1 (low) – 7 (high) | Sum score/number of items | 4.17 | 0.76 | 0.69 | 0.58 | |
| 2CMQ Extra-professional concerns | 8 | 1 (low) – 7 (high) | Sum score/number of items | 4.30 | 0.72 | 0.74 | 0.60 | |
| Importance of life goals (T3) | ||||||||
| Intimacy | 4 | 1 (low) – 5 (high) | Sum score/number of items | 4.60 | 0.60 | 0.76 | ||
| Affiliation | 4 | 1 (low) – 5 (high) | Sum score/number of items | 3.47 | 0.82 | 0.85 | ||
| Altruism | 4 | 1 (low) – 5 (high) | Sum score/number of items | 3.55 | 0.76 | 0.82 | ||
| Power | 4 | 1 (low) – 5 (high) | Sum score/number of items | 2.73 | 0.85 | 0.83 | ||
| Achievement | 4 | 1 (low) – 5 (high) | Sum score/number of items | 4.00 | 0.68 | 0.75 | ||
| Variation | 4 | 1 (low) – 5 (high) | Sum score/number of items | 3.33 | 0.81 | 0.76 | ||
1 PAQ Personal Attributes Questionnaire
2 CMQ Career Motivation Questionnaire
• Questions concerning socio-demographic data and choice of medical speciality
• Sense of Coherence Scale, SOC-13 [29], is a measure of a person's resistance to stress and his/her ability to manage stress (measure of traits, stability in this study T1 – T3: 0.56).
• Rosenberg-Self-Esteem-Scale, RSE [30], assesses general self-esteem and includes items that express a general favourable or unfavourable attitude towards oneself (measure of traits).
• Personal Attributes Questionnaire, GE-PAQ, German Extended Personal Attributes Questionnaire [31], is a self-rating instrument for the assessment of gender-role orientation (measure of traits). The Instrumentality (PAQ-I) scale contains instrumental traits (e.g. 'independent', 'decisive') that are considered to be socially desirable to some degree in both sexes but stereotypically more characteristic of males. The Expressiveness (PAQ-E) scale contains so-called 'feminine' items that describe socially desirable expressive, communal traits (e.g. 'helpful') that are stereotypically more characteristic of females.
• Career Motivation Questionnaire, CMQ [32], consists of 3 scales (measure of traits): Intrinsic Career Motivation CMQ-I (i.e. enjoyment of and interest in professional activities) (stability in this study T1 – T3: 0.57), Extrinsic Career Motivation CMQ-E (i.e. striving for promotion, income, prestige) (stability 0.58) and Extraprofessional Concerns CMQ-EC (i.e. prioritising family, convenient working hours, job security) (stability 0.60).
• Life Goals Questionnaire, GOALS [33], assesses 24 general, long-term life goals pertaining to six major life domains (measure of traits): intimacy (close relationships based on mutual trust and affection), affiliation (spending time with other people, common activities), altruism (acting for the welfare of others), power (asserting oneself, seeking social status), achievement (improving on oneself, meeting standards), and variation (seeking new experiences and excitement). Each goal is rated in regard to the importance (How important is it for you to reach this goal in your lifetime?). Importance ratings indicate which goals are desirable and valuable for the person and indicate the strength of his/her commitment to a goal.
Statistical analyses
All analyses were carried out with SPSS for windows, release 12.0. Descriptive statistics were given in terms of counts and percentages, means and standard deviations respectively. Gender-different speciality choice was tested by Chi2-test. Study hypotheses were tested by univariate analyses of variance, followed by Scheffé-tests, and multivariate analyses of variance and covariance.
Results
Residents' speciality choices at T3: Of the 522 physicians participating at the third assessment, 83 (15.9%) had not yet decided in which speciality they wanted to qualify. The remaining 439 residents had decided to qualify in the following specialities: 45 (8.6%) in primary care, 126 (24.1%) in internal medicine (including all sub-specialities of internal medicine), 68 (13.0%) in surgical disciplines, 31 (5.9%) in gynaecology & obstetrics, 40 (7.7%) in anaesthesiology and intensive care, 44 (8.4%) in paediatrics, 25 (4.8%) in psychiatry, and 60 (11.5%) in other specialities (such as dermatology, ENT, neurology, ophthalmology, radiology). The participants had a list of all 43 officially acknowledged medical specialities in Switzerland, marked with a code number, which they could fill in answering the question concerning the speciality choice.
The development of residents' speciality choices is shown in Figure 2. At the end of medical school 60% of the female and 51% of the male graduates had made their speciality choice. In their second year of residency, 71% of the female and 64% of the male residents had decided, and in the fourth year of residency, 83% of the female and 84% of the male participants named their speciality aspired to. The distribution of the different specialities within the gender group did not change much between the three measurements. However, the distribution of the specialities aspired to by the study participants is different from the speciality distribution represented by the working doctors who hold a speciality qualification. Compared to all working female specialists, there are significantly fewer female residents aspiring to become primary care physicians and psychiatrists; also the group of other specialities is smaller. It might be that some of the still undecided residents will choose one of those specialities later on. Looking at the male participants, fewer residents want to become primary care physicians, internists or psychiatrists but significantly more want to go into surgical disciplines compared to working male doctors.
Figure 2.
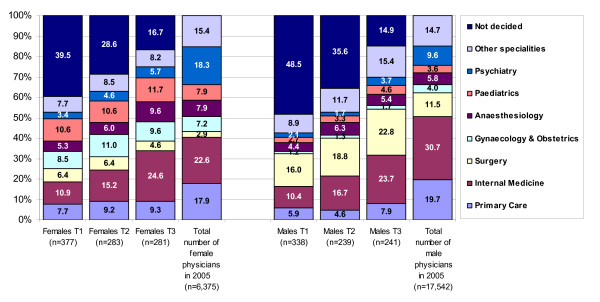
Study residents' speciality choices over time (T1 – T3) and speciality distribution of working doctors (2005).
The speciality choice depending on gender in the study sample at T3 is listed in Table 3. Male residents more often chose surgical specialities, whereas females decided on paediatrics, gynaecology & obstetrics (G&O), and anaesthesiology. In the group of other specialities there was no relevant gender-different distribution.
Table 3.
Frequency distribution of speciality aspired to shown by gender at T3 (n = 522)
| Speciality |
Females (n = 281) n (%) adjusted standardised residual |
Males (n = 241) n (%) adjusted standardised residual |
| Primary Care (n = 45) | 26 (9.3) 0.6 |
19 (7.9) -0.6 |
| Internal medicine (n = 126) | 69 (24.6) 0.2 |
57 (23.7) -0.2 |
| Surgical specialities (n = 68) | 13 (4.6) -6.2 |
55 (22.8) 6.2 |
| Gynaecology & Obstetrics (n = 31) | 27 (9.6) 3.8 |
4 (1.7) -3.8 |
| Anaesthesiology (n = 40) | 27 (9.6) 1.8 |
13 (5.4) -1.8 |
| Paediatrics (n = 44) | 33 (6.3) 2.9 |
11 (4.6) -2.9 |
| Psychiatry (n = 25) | 16 (5.7) 1.0 |
9 (3.7) -1.0 |
| Other specialities (n = 60) | 23 (8.2) -2.6 |
37 (15.4) 2.6 |
| Not decided (n = 83) | 47 (16.7) 0.6 |
36 (14.9) 0.6 |
Chi-square = 65.14, df = 8, p < 0.001
Residents' characteristics depending on speciality aspired to are shown in Table 4. Participants choosing surgical specialities or anaesthesiology comparably show the highest scores for sense of coherence, self-esteem and instrumentality; psychiatry residents give low scores on these three personality scales. With regard to the scores for expressiveness there are no significant differences between the groups. Physicians aspiring to surgical specialities have comparatively high values for intrinsic and extrinsic career motivation, but low values for extraprofessional concerns. Primary care physicians and psychiatrists rate extraprofessional concerns comparatively high. The life goal 'intimacy' is especially important for G&Os. Physicians in the surgical specialities as well as in G&O attach particular importance to 'power'. Future primary care physicians assess the life goal 'achievement' lowest. Subjects pursuing internal medicine show medium level values on all scales.
Table 4.
Means and standard deviations of personality traits, career motivation and importance of life goals according to speciality fields (n = 522)
| Scale |
PC n = 45 Mean (SD) |
IM n = 126 Mean (SD) |
SG n = 68 Mean (SD) |
GO n = 31 Mean (SD) |
AN n = 40 Mean (SD) |
PAED n = 44 Mean (SD) |
PSY n = 25 Mean (SD) |
OS n = 60 Mean (SD) |
ND n = 83 Mean (SD) |
p | Scheffé-test |
| Personality traits | |||||||||||
| SOC Sense of Coherence | 5.03 (0.73) | 4.99 (0.84) | 5.35 (0.82) | 5.03 (0.80) | 5.36 (0.77) | 4.91 (0.93) | 4.85 (1.03) | 5.21 (0.83) | 4.95 (0.77) | 0.011 | PSY, PAED, ND < SG, AN |
| RSE Rosenberg-Self-Esteem | 2.42 (0.38) | 2.27 (0.48) | 2.48 (0.42) | 2.30 (0.37) | 2.50 (0.55) | 2.31 (0.40) | 2.27 (0.62) | 2.44 (0.39) | 2.33 (0.51) | 0.037 | IM, PSY < SG, AN |
| PAQ1 Instrumentality | 4.03 (0.65) | 4.11 (0.63) | 4.63 (0.55) | 3.98 (0.73) | 4.42 (0.69) | 4.14 (0.67) | 3.89 (0.73) | 4.34 (0.59) | 4.00 (0.75) | <0.001 | PSY, GO, PC, ND < OS < AN < SG IM, PAED < SG, AN |
| PAQ1 Expressiveness | 4.93 (0.44) | 4.86 (0.51) | 4.76 (0.66) | 4.98 (0.56) | 4.85 (0.49) | 5.03 (0.53) | 4.97 (0.61) | 4.80 (0.64) | 4.91 (0.56) | 0.255 | - |
| Career motivation | |||||||||||
| CMQ2 Intrinsic motivation | 6.04 (0.51) | 6.09 (0.47) | 6.32 (0.42) | 6.09 (0.54) | 6.21 (0.40) | 6.18 (0.51) | 5.92 (0.59) | 6.16 (0.47) | 5.96 (0.61) | 0.001 | PSY < OS, PAED, AN < SG |
| CMQ2 Extrinsic motivation | 3.41 (0.76) | 3.60 (0.76) | 4.18 (0.88) | 3.75 (0.81) | 3.53 (0.75) | 3.47 (0.72) | 3.79 (0.70) | 4.12 (0.87) | 3.41 (0.95) | <0.001 | SG, OS > rest |
| CMQ2 Extraprofessional concerns | 4.75 (0.87) | 4.55 (0.94) | 3.54 (1.03) | 4.44 (0.95) | 4.15 (1.20) | 4.25 (0.83) | 4.85 (1.02) | 4.21 (0.89) | 4.40 (1.00) | <0.001 | SG < rest AN, OS, PAED < PC, PSY |
| Importance of life goals (GOALS) | |||||||||||
| Intimacy | 4.63 (0.34) | 4.59 (0.43) | 4.41 (0.59) | 4.76 (0.31) | 4.59 (0.46) | 4.66 (0.47) | 4.50 (0.55) | 4.67 (0.37) | 4.58 (0.49) | 0.016 | SG < GO |
| Affiliation | 3.50 (0.75) | 3.64 (0.69) | 3.46 (0.92) | 3.77 (0.79) | 3.64 (0.68) | 3.73 (0.76) | 3.53 (0.73) | 3.65 (0.69) | 3.62 (0.73) | 0.559 | - |
| Altruism | 3.73 (0.70) | 3.61 (0.58) | 3.73 (0.77) | 3.58 (0.56) | 3.71 (0.79) | 3.96 (0.71) | 3.41 (0.43) | 3.55 (0.73) | 3.66 (0.74) | 0.40 | - |
| Power | 2.53 (0.76) | 2.77 (0.77) | 3.07 (0.86) | 2.99 (0.63) | 2.63 (0.74) | 2.68 (0.70) | 2.97 (0.72) | 2.85 (0.76) | 2.70 (0.81) | 0.006 | PC < GO, SG |
| Achievement | 4.03 (0.56) | 4.22 (0.49) | 4.45 (0.46) | 4.25 (0.47) | 4.34 (0.48) | 4.33 (0.52) | 4.21 (0.46) | 4.32 (0.48) | 4.19 (0.56) | 0.002 | PC < OS, PAED, AN, SG |
| Variation | 3.80 (0.69) | 3.66 (0.70) | 3.82 (0.67) | 3.73 (0.75) | 3.86 (0.68) | 3.84 (0.66) | 3.43 (0.70) | 3.75 (0.75) | 3.75 (0.80) | 0.301 | - |
1PAQ Personal Attributes Questionnaire
2CMQ Career Motivation Questionnaire
PC = Primary Care, IM = Internal Medicine, SG = Surgery, GO = G&O, AN = Anaesthesiology, PAED = Paediatrics, PSY = Psychiatry, OS = Other specialities, ND = Not decided
The multivariate analyses of the influence of gender, personality traits, career motivation and importance of life goals is shown in Table 5. The effect of gender remained significant after controlling for personality traits, career motivation and life goals as covariates. The same does not apply to the influence of personality traits on the speciality choice after controlling for career motivation and life goals. In other words, there are no direct significant influences of personality traits on the speciality choice. This means that career motivation and life goals can be considered as mediator variables.
Table 5.
Influence of gender, personality traits, career motivation and importance of life goals on speciality choice at T3 (n = 522), multivariate analyses
| Wilk's Lambda | F (dfeffect, dferror) | p | Eta-quadrat | |
| Gender | F(8,513) = 9.14 | <0.001 | 0.13 | |
| Personality traits | 0.85 | F(32,1868) = 2.65 | <0.001 | 0.04 |
| Career motivation | 0.79 | F(24,1474) = 5.34 | <0.001 | 0.08 |
| Life goals | 0.81 | F(48,2503) = 2.31 | <0.001 | 0.04 |
| Gender (covariates: personality traits, career motivation, life goals) | F(8,493) = 5.45 | <0.001 | 0.08 | |
| Personality traits (covariates: career motivation, life goals) | 0.92 | F(32,1823) = 1.29 | 0.128 | 0.02 |
Discussion
The present study is part of an ongoing prospective survey of a cohort of Swiss medical school graduates. Subjects included in the study are fourth-year residents in different medical speciality fields. The aims of the study are to examine (1) the development of the residents' speciality choices since graduating from medical school and (2) what factors influenced their choices.
Development of the residents' speciality choices: at the end of medical school a considerable number of students have not yet developed precise ideas as to which speciality they want to work in. The main reason is lack of clinical experience. During the first and second years of post-graduate training they gain insight into various specialities, which makes it easier for them to make their decision. Some residents change the speciality they primarily aspired to, but not so many do. Nor is a marked shift away from one speciality towards another evident. Compared to the working doctors, significantly fewer young doctors aspire to become primary care physicians (PCPs) or psychiatrists. In the competition-based health care systems of Switzerland and the other German-speaking countries the professional prestige, social status, and income of other specialists is much higher than those of PCPs and psychiatrists. As long as the current health policy does not create better professional conditions, the shift away from PC and psychiatry will continue. If this trend prevails for some time, there will be a shortage of doctors providing basic somatic and mental health care, especially in rural areas.
Factors influencing speciality choice: As hypothesized, we found gender different speciality choices, female doctors being over-represented in specialities like gynaecology & obstetrics (G&O), paediatrics, and anaesthesiology and male doctors in surgical specialities. Similar results are reported in other studies [11-13,17,34]. Although G&O entails long hours and a heavy surgical workload, a growing number of women choose this speciality. Women are interested in surgical specialities, but often experience gender-relevant exclusion mechanisms in other surgical fields [17,35]. The marked gender shift in G&O is due to the growing attitude, starting in the late 1980s, that women should be treated by female physicians [36]. Paediatrics, the other speciality mainly chosen by women, is also a speciality in which gender schemas play a certain role [14]. This gender-distinct speciality choice was already found when the participants were in the last year of medical school [15]. The reasons for an increasing number of female doctors choosing anaesthesiology might be manifold: anaesthesiology is a professionally prestigious speciality like surgery but not as competitive, it covers a broad medical spectrum and offers good options for part-time work and good promotion prospects, all factors appreciated by females. Whether the decisive role of gender is based on internalised gender roles or whether there are open or masked deterrents cannot be distinguished by this study.
Personality, career motivation, life goals and speciality choice: According to our assumption, we found that gender, personality, career motivation and life goals have an impact on speciality choice. Petrides and McManus [1] described a mapping of medical careers based on the typology found by Holland in careers in general. Holland's theory [37] suggests that careers can be organised into six broad types, which can be represented around a hexagon, known by the acronym RIASEC, standing for 'Realistic', 'Investigative', 'Artistic', 'Social', 'Enterprising' and 'Conventional'. They also referred to the 'Things↔People' and 'Ideas↔Data' dimensions proposed by Prediger [38] which can be underpinned to Holland's typology. Both models use the attribution of the medical specialities based on the characteristics of their professional activities. We suppose that residents choose a medical speciality in which they can conduct their professional activities corresponding to their special personality traits, career motivation, and life goals aspired to. The residents in surgical specialities in our study were characterised by high values for instrumentality, intrinsic and extrinsic career motivation, 'power' and 'achievement' as life goals. These attributes and attitudes are mainly 'Things/technique-oriented' according to Prediger and can be assigned to Holland's realistic career type. Participants choosing anaesthesiology and intensive care assessed themselves almost as highly instrumental as doctors in surgery. They can also be mapped to the realistic type. Contrary to the study by Petrides & McManus [1], the G&O residents in our sample revealed characteristics of 'People Orientation', matching the social type, a fact which might be influenced by the high number of females in this group. They stated high expressiveness and life goals aiming at satisfying social relationships. Paediatricians in our study, mainly females, showed similar characteristics as the G&Os. Psychiatrists differed from all the other specialities by rating the extraprofessional concerns highest, while expressiveness and altruism were not values very high. They could not easily be assigned to one of the RIASEC types. The same applies for primary care physicians. They showed characteristics of 'People Orientation' (high extraprofessional concerns and altruism), and rated in the medium range in most of the other aspects. The internists were allocated to the investigative type by Petrides & McManus [1], a type in which patient-relationships and diagnostic investigations play their part. This might also apply to the internists in our study; they described themselves as empathetic (adequate expressiveness), but also instrumentally-oriented. The RIASEC mapping of medical specialities did not consider career motivation and life goals but focused only on personality traits. Our results indicate that career motivation and life goals are even more important for the speciality choice than personality traits.
In summary, the results of our study indicate that gender plays a decisive role in speciality choice, while the influence of personality declines after controlling for career motivation and life goals. The feminisation of medicine and especially of some specialities can be expected to lead to fundamental changes in the medical system. One can assume that the style of leadership in hospitals will change: As long as men are department heads, a "command and control style of managing others" will predominate, while women tend towards "interactive leadership" [39]. Other aspects concern employment: more part-time jobs have to be provided for women doctors with family obligations. However, the feminisation also carries the risk of the danger of vertical and horizontal gender segregation [40]: female physicians often spend more time with patients while male doctors look at what is more advantageous for their career, such as laboratory work, developing research projects and writing papers. These differences in working attitudes result in gender-different career opportunities: males taking over leadership positions and females looking after their patients' needs.
Conclusion
The speciality choice of the new generation of doctors is a matter of concern for the health care system in Switzerland. Ideally, as many doctors should practise in a speciality as are needed to cover the population's health care. As the statistics of the Swiss Medical Association and our study data show, a lack of primary care physicians as well as of psychiatrists will occur in the next decade. The question arises whether incentives, mainly financial, will encourage more young doctors to choose to become primary care physicians or psychiatrists, or whether access to the speciality qualification programmes and to the allocation of private practice licenses should be regulated by health policy.
There should be an acknowledgment of the distinctive features of female physicians' careers. Workplace conditions should allow women doctors, if they want, to combine pursuing a prestigious career in medicine with having a family. There is a need to promote and encourage their instrumental traits and extrinsic career motivation. Motivational guidance by senior physicians throughout medical training should not only focus on the professional career but should also consider the personal life goals of those being mentored.
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
All authors designed the study. BBF was responsible for data acquisition, RK conducted the statistical analyses. BBF, RK, TA and CB contributed to the interpretation of data, BBF drafted the manuscript versions, RK, TA and CB revised the drafts critically for important intellectual content. All authors gave final approval to the version to be published.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Acknowledgments
Acknowledgements
The study was supported by grants from the Swiss National Science Foundation (NF Nos. 3200-061906.00 and 3200 BO-102130).
Contributor Information
Barbara Buddeberg-Fischer, Email: barbara.buddeberg@usz.ch.
Richard Klaghofer, Email: richard.klaghofer@usz.ch.
Thomas Abel, Email: abel@ispm.unibe.ch.
Claus Buddeberg, Email: claus.buddeberg@usz.ch.
References
- Petrides KV, Mcmanus IC. Mapping medical careers: questionnaire assessment of career preference in medical school applicants and final-year students. BMC Medical Education. 2004;4:18 doi: 10.1186/1472-6920-4-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ciechanowski PS, Worley LL, Russo JE, Katon WJ. Using relationship styles based on attachment theory to improve understanding of specialty choice in medicine. BMC Medical Education. 2006;6:3 doi: 10.1186/1472-6920-6-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dorsey ER, Jarjoura D, Rutecki GW. The influence of controllable lifestyle and sex on the specialty choices of graduating U.S. medical students, 1996-2003. Academic Medicine. 2005;80:791–796. doi: 10.1097/00001888-200509000-00002. [DOI] [PubMed] [Google Scholar]
- Vaidya NA, Sierles FS, Raida MD, Fakhoury FJ, Przybeck TR, Cloninger CR. Relationship between specialty choice and medical student temperament and character assessed with Cloninger Inventory. Teaching and learning in medicine. 2004;16:150–156. doi: 10.1207/s15328015tlm1602_6. [DOI] [PubMed] [Google Scholar]
- Bundesamt für Statistik . Das Medizinstudium in der Schweiz im Profil. Neuchatel, Bundesamt für Statistik; 2005. [Google Scholar]
- Statistisches Bundesamt . Medizinstudierende in Deutschland. Wiesbaden, Statistisches Bundesamt; 2005. [Google Scholar]
- British Medical Association . Statistics of medical students in the U.K. London, BMA, Health Policy & Economic Research Unit; 2002. [Google Scholar]
- Association of American Medical Colleges Women in U.S. Academic Medicine Statistics 2002-2003. 2003.
- Bundesärztekammer Berufstätige Ärzte/Ärztinnen nach Fachrichtungen und Altersgruppen in Deutschland, Stand 31.12.2004. 2005.
- Generalsekretariat der Verbindung der Schweizer Ärztinnen und Ärzte FMH-Ärztestatistik 2005. Schweizerische Ärztezeitung. 2006;87:747–767. [Google Scholar]
- British Medical Association . BMA Cohort Study of 1995 Medical Graduates. London, British Medical Association, Health Policy & Economic Research Unit; 2005. [Google Scholar]
- Gjerberg E. Gender differences in doctors' preference - and gender differences in final specialisation. Social Science & Medicine. 2002;54:591–605. doi: 10.1016/S0277-9536(01)00054-5. [DOI] [PubMed] [Google Scholar]
- Gjerberg E. Medical women - towards full integration? An analysis of the specialty choices made by two cohorts of Norwegian doctors. Social Science & Medicine. 2001;52:331–343. doi: 10.1016/S0277-9536(00)00138-6. [DOI] [PubMed] [Google Scholar]
- Valian V. Why so slow? The advancement of women. Cambridge, Mass., London, MIT Press; 1999. [Google Scholar]
- Buddeberg-Fischer B, Klaghofer R, Abel T, Buddeberg C. The influence of gender and personality traits on the career planning of medical students. Swiss Medical Weekly. 2003;133:535–540. doi: 10.4414/smw.2003.10418. [DOI] [PubMed] [Google Scholar]
- Buddeberg-Fischer B, Illés C, Klaghofer R. Karrierewünsche und Karriereängste von Medizinstudierenden - Ergebnisse von Fokusgruppeninterviews mit Staatsexamenskandidatinnen und -kandidaten. Das Gesundheitswesen. 2002;64:353–362. doi: 10.1055/s-2002-32179. [DOI] [PubMed] [Google Scholar]
- Gargiulo DA, Hyman NH, Hebert JC. Women in surgery: do we really understand the deterrents. Archives of Surgery. 2006;141:405–407. doi: 10.1001/archsurg.141.4.405. [DOI] [PubMed] [Google Scholar]
- Buddeberg-Fischer B, Klaghofer R, Zivanovic I, Vetsch E, Buddeberg C. Institutional conditions and individual experiences in the career-entry period of Swiss medical residents - a qualitative study. Swiss Medical Weekly. 2006;136:26–32. doi: 10.4414/smw.2006.11199. [DOI] [PubMed] [Google Scholar]
- Buddeberg-Fischer B, Klaghofer R, Abel T, Buddeberg C. Junior physicians' workplace experiences in clinical fields in German-speaking Switzerland. Swiss Medical Weekly. 2005;135:19–26. doi: 10.4414/smw.2005.10830. [DOI] [PubMed] [Google Scholar]
- Dorsey ER, Jarjoura D, Rutecki GW. Influence of controllable lifestyle on recent trends in specialty choice by US medical students. Journal of the American Medical Association. 2003;290:1173–1178. doi: 10.1001/jama.290.9.1173. [DOI] [PubMed] [Google Scholar]
- Lambert EM, Holmboe ES. The relationship between specialty choice and gender of U.S. medical students, 1990-2003. Academic Medicine. 2005;80:797–802. doi: 10.1097/00001888-200509000-00003. [DOI] [PubMed] [Google Scholar]
- Newton DA, Grayson MS, Foster Thompson L. The variable influence of lifestyle and income on medical students' career choices: data from two U.S. medical schools, 1998-2004. Academic Medicine. 2005;80:809–796. doi: 10.1097/00001888-200509000-00005. [DOI] [PubMed] [Google Scholar]
- Azzizadeh A, McCollum CH, Miller CC, Holliday KM, Shilstone HC, Lucci A. Factors influencing career choice among medical students interested in surgery. Current Surgery. 2003;60:210–213. doi: 10.1016/S0149-7944(02)00679-7. [DOI] [PubMed] [Google Scholar]
- Thornton J, Esposto F. How important are economic factors in choice of medical specialties? Health economics. 2003;12:67–73. doi: 10.1002/hec.682. [DOI] [PubMed] [Google Scholar]
- Rosenblatt RA, Andrilla CH. The impact of U.S. medical students' debt on their choice of primary care careers: an analysis of data from the 2002 medical school graduation questionnaire. Academic Medicine. 2005;80:815–819. doi: 10.1097/00001888-200509000-00006. [DOI] [PubMed] [Google Scholar]
- Weeks WB, Wallace AE. The more things change: revisiting a comparison of educational costs and incomes of physicians and other professionals. Academic Medicine. 2002;77:312–319. doi: 10.1097/00001888-200204000-00010. [DOI] [PubMed] [Google Scholar]
- Girard DE, Choi D, Dickey JDD, Bloom JD. A comparison study of career satisfaction and emotional states between primary care and specialty residents. Medical Education. 2006;40:79–86. doi: 10.1111/j.1365-2929.2005.02350.x. [DOI] [PubMed] [Google Scholar]
- Caniano DA, Sonnino RE, Paolo AM. Keys to career satisfaction: insights from a survey of women pediatric surgeons. Journal of Pediatric Surgery. 2004;39:984–990. doi: 10.1016/j.jpedsurg.2004.02.039. [DOI] [PubMed] [Google Scholar]
- Antonovsky A. Unraveling the mystery of health. How people manage stress and stay well. San Francisco, Jossey-Bass; 1987. [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton N.J., University Press; 1965. [Google Scholar]
- Alfermann D. Androgynie. In: Reigber D, editor. Frauen-Welten. Düsseldorf, Econ; 1993. pp. 147–200. [Google Scholar]
- Abele AE. Karriereorientierungen angehender Akademikerinnen und Akademiker. Bielefeld, Kleine; 1994. [Google Scholar]
- Poehlmann K, Brunstein JC. GOALS: Ein Fragebogen zur Messung von Lebenszielen. Diagnostica. 1997;43:63–79. [Google Scholar]
- Wendel TM, Godellas CV, Prinz RA. Are there gender differences in choosing a surgical career? Surgery. 2003;134:591–596. doi: 10.1016/S0039-6060(03)00304-0. [DOI] [PubMed] [Google Scholar]
- McManus IC, Sproston KA. Women in hospital medicine in the United Kingdom: glass ceiling, preference, prejudice or cohort effect? J Epidemiol Community Health. 2000;54:10–16. doi: 10.1136/jech.54.1.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitzdorf U, Beck K. Frauenspezifische Probleme in der Medizin aus feministischer Sicht. In: Pöppel E, Bullinger M and Härtel U, editor. Medizinische Psychologie und Soziologie. Weinheim, Chapman & Hall; 1994. pp. 386–404. [Google Scholar]
- Holland JL. Making vocational choices: A theory of careers. New York, Prentice Hall; 1973. [Google Scholar]
- Prediger DJ. Dimensions underlying Holland's Hexagon: Missing link between interests and occupation? Journal of Vocational Behavior. 1982;21:259–287. doi: 10.1016/0001-8791(82)90036-7. [DOI] [Google Scholar]
- Rosener JB. Ways women lead. In: Kanter RM, editor. Reach for the top. Boston, Harvard Press; 1990. pp. 13–23. [Google Scholar]
- Wetterer A. Professionalisierung und Geschlechterhierarchie. Vom kollektiven Frauenausschluss zur Integration mit beschränkten Möglichkeiten. Vol. 3. Kassel, Wissenschaft ist Frauensache. Neue Folge; 1993. [Google Scholar]