

Abstract
Objective
Depression is one of the most frequent neuropsychiatric disturbances in stroke patients. The clinical aspects and correlations of depression in the first days after acute stroke are less known. This study aimed to 1) assess the frequency of depression, 2) describe the profile of depression of stroke patients and 3) analyze the relation between depression and demographic, predisposing and precipitating conditions, and clinical and imaging data, in acute stroke patients.
Methods
We used the Montgomery–Asberg Depression Rating Scale to assess depression in 178 consecutive acute (≤ 4 days) stroke (26 subarachnoid hemorrhage, 31 intracerebral hemorrhage, 121 cerebral infarct) patients (mean age 57 yr) and in a control group of 50 acute coronary patients (mean age 59 yr).
Results
Eighty-two patients (46%) presented acute depression; apathy/loss of interest was the most frequent clinical feature. In logistic regression, the best model to predict depression (backward model) identified previous mood disorder (odds ratio 2.2–12.9) as an independent predictor. There were no significant differences in the frequency or severity (p > 0.45) of depression between control subjects and acute stroke patients.
Conclusions
Depression was present in almost one-half of the acute stroke patients and was related to previous mood disorder but not not to stroke type or location. Apathy/loss of interest was the predominant clinical feature.
Medical subject headings: stroke, acute; depression; MADRS
Abstract
Objectif
La dépression constitue l'un des troubles neuropsychiatriques les plus courants chez les patients victimes d'un accident vasculaire cérébral. On connaît moins les aspects cliniques et les liens avec la dépression au cours des premiers jours qui suivent un accident vasculaire cérébral aigu. Cette étude visait à 1) évaluer la fréquence de la dépression, 2) décrire le profil de la dépression chez les patients qui ont subi un accident vasculaire cérébral et 3) analyser le lien entre la dépression et certains facteurs démographiques et conditions prédisposantes et déclenchantes, et les données cliniques et d'imagerie, chez les patients victimes d'un accident vasculaire cérébral aigu.
Méthodes
Nous avons utilisé l'échelle d'appréciation de la dépression de Montgomery–Asberg pour évaluer la dépression chez 178 patients consécutifs victimes d'un accident vasculaire cérébral aigu (£ 4 jours) (26 hémorragies sous-arachnoïdiennes, 31 hémorragies intracérébrales, 121 infarctus cérébraux) (âge moyen de 57 ans) et chez les sujets d'un groupe témoin de 50 patients victimes d'un syndrome coronarien aigu (âge moyen de 59 ans).
Résultats
Quatre-vingt-deux patients (46 %) avaient une dépression aiguë et l'apathie ou la perte d'intérêt constituait la caractéristique clinique la plus fréquente. Au cours d'une régression logistique, le meilleur modèle pour prédire la dépression (modèle rétrograde) a identifié des troubles antérieurs de l'humeur (coefficient de probabilité 2,2–12,9) comme prédicteur indépendant. Il n'y avait pas de différences significatives au niveau de la fréquence ou de la gravité (p > 0,45) de la dépression entre les sujets témoins et les patients victimes d'un accident vasculaire cérébral aigu.
Conclusions
La dépression était présente chez près de la moitié des patients victimes d'un accident vasculaire cérébral aigu et était reliée à un trouble antérieur de l'humeur, mais non au type de l'accident ni à son site. L'apathie ou la perte d'intérêt constituait la caractéristique clinique dominante.
Introduction
Depression is one of the most frequent neuropsychiatric disturbances in acute stroke, being present in 6%–52% of acute stroke patients.1–12 Further, poststroke depression is associated with impaired recovery in cognitive function and activities of daily living and increases mortality.13
There are contradictory results about the location of the stroke lesions that are associated with depression in acute stroke. In several studies, depression was found to be most frequent and severe among patients with left anterior (cortical or subcortical) lesions,7,10,11,14–17 while in several case descriptions of patients with depression, acute right hemisphere lesions18,19 were more obvious. A systematic review of patients with first-ever ischemic stroke did not associate depression with any particular acute hemispheric lesion site.1 Two metaanalyses did not support the hypothesis that the risk of depression after stroke is due to a specific location of stroke,20,21 while a systematic review by Bhogal and others8 sustained that depression was related to the left hemispheric stroke.
This study aimed to assess the frequency of depression and to describe the profile of depression of stroke patients in the first 4 days after stroke. We also aimed to analyze the relation between depression and a) demographics and predisposing and precipitating conditions, b) clinical and imaging data and c) functional outcome at discharge.
Methods
We investigated prospectively the presence, severity and correlates of depression in consecutive acute stroke patients. The inclusion criteria were as follows: 1) an admission diagnosis of cerebral infarct, intracerebral hemorrhage/intraventricular hemorrhage and subarachnoid hemorrhage and 2) depression assessment performed within 4 days after stroke onset.
We excluded from the study patients who scored less than 10 on the Glasgow Coma Scale (GCS) on “eye opening” (range 1–4) and “best motor response” (range 1–6) items.22 We also excluded patients with a severe communication disturbance, defined as scoring ≥ 2 on the Neurological Institute Health Stroke Scale (NIHSS)23 on items “best language” or “dysarthria.”
The control group comprised consecutive acute coronary patients hospitalized in the Coronary Intensive Care Unit of the Hospital de Santa Maria, Lisboa, with a diagnosis of acute myocardial infarction or unstable angina. A depression assessment was performed within 4 days after onset. In addition to the exclusion criteria for stroke patients, we excluded patients with concomitant stroke.
A trained psychologist conducted this study at the Stroke Unit in the neurology department of a university hospital. Stroke patients were examined whenever possible on their first day in the stroke unit. A psychiatrist further observed the same patient if a psychiatric disorder was presumed. Previous dementia or cognitive decline, mood disorder and acute neuropsychiatric disturbances were assessed during a semistructured interview.
Patients were diagnosed as having depression if they fulfilled the Diagnostic and statistical manual of mental disorders, fourth edition, text revision (DSM-IV-TR)24 criteria of Mood Disorder Due to Acute Stroke (depression), that is, if they reported and displayed depressive mood or anhedonia scoring in the items “Apparent Sadness” or “Reported Sadness” and “Inability to Feel” of the Montgomery–Asberg Depression Rating Scale (MARS)25 and had a MARS score ≥ 7 points.26–28 We used the MARS to assess intensity of depressive symptoms. We used the Gainotti's Post Stroke Depression Rating Scale (PSDRS)29,30 to describe the profile of depressive symptoms, because this scale relies less on symptoms that can be due to stroke itself, such as vegetative and sleep disturbances. For formal global cognitive assessment, we used the Mini-Mental State Examination (MMSE), validated in the Portuguese population,31 taking educational levels into consideration, as previously described.32
The following prestroke predisposing conditions for depression were considered: 1) dementia/cognitive decline, defined as a medical diagnosis of dementia or of mild cognitive impairment or a history of memory and another cognitive domain impairment with functional impairment in daily living activities, confirmed by a proxy; 2) alcohol abuse, defined as having at least 5 drinks daily; 3) previous stroke; and 4) previous mood disorder.24 Mood disorder was diagnosed if the patient had at least once in their lifetime been treated for a mood disorder and had been either prescribed specific medications for this condition, or used the medication for more than a month. The stroke symptoms fluent or nonfluent aphasia,1 neglect and hemiparesis were analyzed as possible predisposing variables for depression.
We defined the type and location of the stroke based on clinical data and on acute computed tomography (CT) magnetic resonance imaging (MRI). The type of stroke was defined as subarachnoid hemorrhage, intracerebral/intraventricular hemorrhage and infarct. If the CT/MRI failed to show an acute lesion, or showed only an old silent or old symptomatic lesion, location was derived from clinical data and was grouped as 1) brainstem/cerebellum, hemispherical or both and 2) left or right hemispherical or both. When the symptomatic lesion was visible on the CT/MRI, we grouped the stroke location as 1) brainstem/cerebellum, hemispherical or both and 2) left or right hemispherical or both. Hemispherical strokes were further subdivided as deep (thalamic and striatocapsular infarcts and lacunes), superficial anterior (frontal, fronto-temporal/parietal/insular) and superficial posterior (temporal, parietal, occipital or a combination of these).33 For statistical analyses, we considered a superficial lesion extending into the deep hemispherical structures.
We assessed functional outcome at discharge with the modified Rankin Scale34 (mRS). An unfavourable outcome was defined as a modified Rankin score of ≥ 3 (death or dependency). We assessed the presence and severity of depression in the control group as previously described for stroke patients.
Statistics
Data were analyzed in the Special Package for Social Sciences version 12. We used chi-square with continuity correction (χ2), odds ratios (ORs) and 95% confidence interval (95% CI) to test bivariate associations between the presence of depression and age (< 65 or ≥ 65 yr), sex and educational level (0–9 or ≥ 10 years of school, according to the minimal number of mandatory years of schooling in Portugal) and predisposing and precipitating conditions (previous stroke, dementia/cognitive decline, mood disorder and alcohol abuse). We used the same method to test for depression, clinical symptoms and signs (aphasia, neglect, hemiparesis), type (subarachnoid hemorrhage, intracerebral hemorrhage, infarct) and location (brainstem-cerebellum or hemispherical; hemispherical, left or right; hemispherical, deep or superficial; superficial, anterior or posterior) of stroke and mRS grade at discharge (0–2 or ≥ 3). We used the Mann–Whitney U test or the Kruskal–Wallis test to measure differences in MARS scores between 2 or more than 2 conditions of those categorical variables, respectively. For multivariate analysis, we used stepwise logistic regression, entering all the variables with a p < 0.15 on chi-square. Additionally, we calculated the receiver operating characteristic curves to assess the predictive value of the model. We also performed a bivariate and a multivariate analysis to analyze whether the above-mentioned variables were related to severe depression (MARS score ≥ 19). We considered a p-value ≤ 0.05 statistically significant.
Results
From a sample of 218 stroke patients, we assessed depression in 178 acute stroke patients. We found no significant differences between included and excluded patients concerning age (p = 0.32), sex (p = 1.0) and previous mood disorder (p = 0.52). Included patients had a higher mean educational level (p = 0.01) and a lower frequency of intracerebral hemorrhage (p = 0.001) than excluded patients.
Sixty percent of our sample were men and 40% were women, both with a mean age of 56.8 years (standard deviation [SD] 13, median 57, range 24–86 yr) and a median of 4 years of school (mean 6.6, SD 5, range 0–21 yr). During the acute phase, 23% (41) of the patients were assessed in the first day, 32% (57) in the second day, 23% (41) in the third day and 22% (39) in the fourth day (mean 2.4, SD 1.1; median 2). The characteristics of the stroke are displayed in Table 1.
Table 1
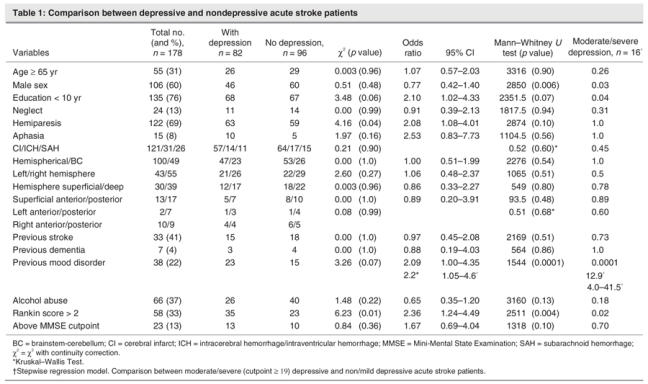
Thirteen percent of the patients presented a cognitive disturbance, as assessed with the MMSE (mean 25, SD 4.6, median 27, range 8–30). The median in the mRS score was 2 (range 0–6); one-third of the acute stroke patients had a poor outcome, with an mRS score > 2. (Table 1). Depression was diagnosed in 82 patients (46%) (mean score 13.7, SD 6.9, median 11.5, range 7–39). The whole sample had a mean MARS score of 8.3 (SD 7.3, median 7, range 0–35). Depression was associated with female sex, hemiparesis, previous mood disorder and an mRS score > 2. Age, sex, aphasia and previous mood disorder were included in the backward regression model. The final model (R2 = 0.05) included previous mood disorder as an independent predictive factor for depression (area under the ROC = 60%).
Regarding the PSDRS, the profile of the patients with depression was characterized by depressed mood, suicidal thoughts, vegetative disorders, apathy/loss of interest, anxiety, catastrophic reaction, increased emotionalism and anhedonia, which was different from the profile of the patients without depression (p < 0.01) (Fig. 1).
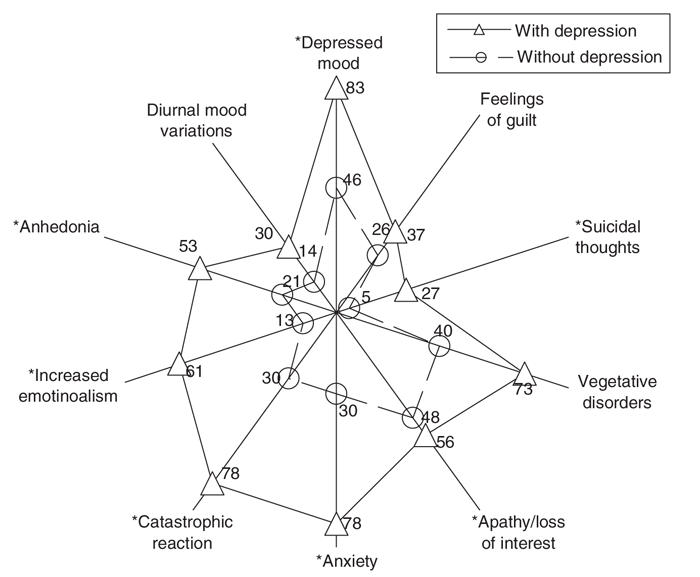
Fig. 1: Profile (in %) of acute stroke patients, with and without depression, in the 10 items of the Post Stroke Depression Rating Scale (PSDRS). Except for feelings of guilt and diurnal variation, stroke patients with depression scored ≥ 1 more frequently (*) when compared with stroke patients with no depression (p < 0.01).
Sixteen (9%) of the total stroke patients scored ≥ 19 on the MARS (moderate or severe depression). Patients with severe depression were more frequently female (n = 11; 69%), had a lower educational level (n = 16; 100%) and had a history of mood disorder (n = 10; 63%). When we entered the variables sex, educational level and previous mood disorder, the final backward regression model (R2 = 0.33) selected previous mood disorder as an independent predictive factor for moderate or severe depression (area under the ROC = 82%).
We assessed 50 control subjects with acute coronary disease, with a mean age of 59.1 years (SD 14.2, median 60, range 34–83 yr) and a median of 4 years of school (mean 8.1, SD 5.5, range 0–17 yr). Seventy-six percent of the patients were men and 24% were women. During the acute phase, 38% (19) of the coronary patients were assessed in the first day, 22% in the second, 24% in the third and 16% in the fourth. Control subjects were more frequently male and had a lower frequency of previous alcohol abuse, compared with stroke patients (Table 2).
Table 2
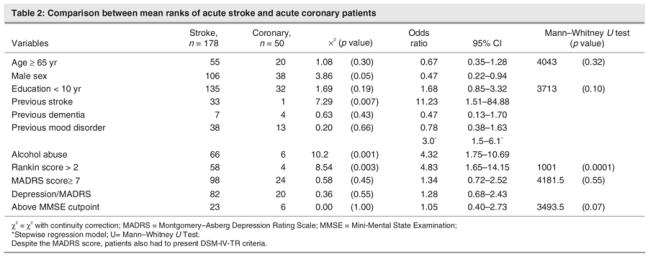
Twenty control subjects (40%) presented depression in the first 4 days of coronary disease. Compared with control subjects, the profile of depression in stroke patients was characterized by a higher frequency of apathy/loss of interest (p = 0.01) (Fig. 2). Case subjects did not have a higher frequency of depression than control subjects (OR 1.3; 95% CI 0.7–2.4). We entered the variables age, sex, educational level, previous mood disorder, stroke and coronary disease into a backward regression model. The final model (R2 = 0.10) selected previous mood disorder as an independent predictive factor for depression (area under the ROC = 61%).
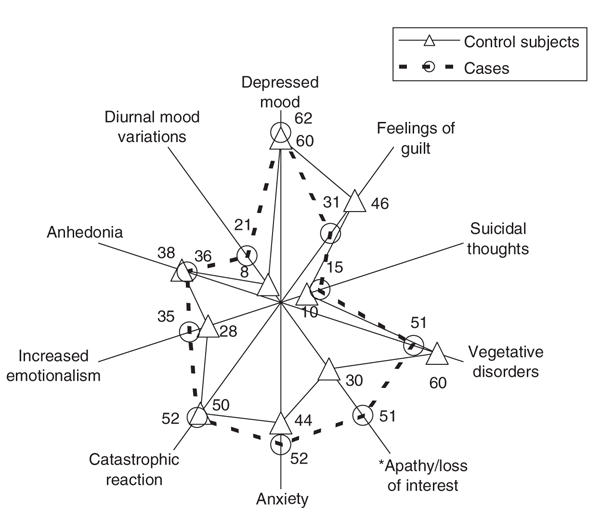
Fig. 2: Profile (in %) of the cases and control subjects in the 10 items of the Post Stroke Depression Rating Scale (PSDRS). Acute stroke patients scored more frequently in the item apathy/loss of interest (*) when compared with control subjects.
Discussion
Depression was frequent, being present in 46% of the acute stroke inpatients. Nine percent of the patients had moderate or severe depression. Female sex, the presence of a hemiparesis and previous mood disorder were associated with depression; the presence of a previous mood disorder was the only independent predictive factor for depression or severe depression. The profile of the patients with depression was characterized by depressed mood, suicidal thoughts, apathy/loss of interest, anxiety, catastrophic reaction, increased emotionalism and anhedonia.
The present study has some limitations, such as the exclusion of severe aphasic patients and the absence of an acute imaging exam that is more sensitive than a CT, such as diffusion MR or perfusion CT.
The use of the DSM-IV-TR depression criteria24 and of a validated scale as MARS, appropriate to the acute phase of stroke, allowed us to assess the prevalence and severity of acute stroke depression; the PSDRS allowed us to define the symptomatic profile of the patients with depression.
The frequency of acute poststroke depression or acute depressive symptoms, within the first days of acute stroke, were reported in about 27%–52% of the case subjects, depending on the sample size, methodology and scale used by the researchers.2,4,6,7,9,35 We found a higher frequency of depression, probably because we used the DSM-IV-TR criteria of Mood Disorder Due to Acute Stroke—the most appropriate criteria for the acute phase of a stroke—and because we used a different depression scale than that reported in other studies on depression in acute stroke.
Coronary patients had the same risk of developing depression as did stroke patients, contradicting research by Aben and colleagues,2 who found that stroke patients had a risk of of developing depression 1.7 times (95% CI 1.0–2.9) that of coronary patients. We assessed depression within the 4 days after stroke, whereas Aben and colleagues2 assessed depression within 1 month.
In our study, independent of the severity of depressive symptoms, previous mood disorder was the major independent predictive factor for depression. The presense of a previous mood disorder could highlight a neuropsychiatric vulnerability for ischemic stroke36 and, consequently, for acute stroke depression.
As in primary depression, female sex was associated with acute stroke depression. Berg and colleagues1 and Carota and colleagues35 reported the association with female sex, but their study did not reach a significant level. Notably, there was a higher proportion of depression in older women that is perceptible in acute stroke patients, as observed by Berg and colleagues,1 for poststroke patients with depression.
The absence of a relation between depression and aphasia is not in agreement with the study by Carota and colleagues,35 who reported a borderline level of significance between overt sadness and aphasia. Kellermann and colleagues6 also reported a higher depression scale score in patients with aphasia. However, in a systematic review, Bhogal and colleagues8 highlighted that aphasia increases the risk of developing poststroke depression but not acute stroke depression.
Left lesions have been reported as an independent factor for depression,8 particularly if they are small-sized lesions37 or if they are located in the basal ganglia (mainly in the head of the caudate)38 or frontal lobe.10 Berg and colleagues1 did not find an interaction between higher depression scores and lesion side, nor did Carson and colleagues20 in their systematic review. Berg and colleagues1 reported a higher nonsignificant frequency of depression after left lesion and brainstem strokes. More recently, Nys and colleagues9 found that, in first-ever stroke patients, a moderate or severe depression was associated with higher lesion volume but not with lesion location, previous white matter lesion or previous silent infarcts. Our research supported the systematic review by Bhogal and colleagues8: we did not find a relation between acute depression and side lesion in inpatients.
In our sample, in the first 4 days after stroke, patients cried and reported sadness more frequently than previously reported.35 Dissociation between crying behaviour, appearance of being sad and anhedonia were described in a previous publication.35 Crying is associated with a patient's subjective report of feelings of sadness and with the presence of aphasia. de Coster and colleagues39 reported that the clinical profile of depression in acute stroke is related to depressed mood, the most sensitive symptom to the diagnosis of depression.
When compared with acute coronary patients, we found that apathy/loss of interest was the only symptom that was more frequent in acute stroke patients. Often it is stated that anhedonia is part of the concept of apathy and is not as sensitive for the diagnosis of depression as is depressed mood.39 The finding that apathy/loss of interest is the only symptom that differentiated case subjects from control subjects might indicate that, although depressed mood may be a depressive reaction to a serious acute illness requiring hospitalization,9 apathy or anhedonia is probably related to the brain lesion.29,30,40–42
Conclusions
Depression was present in almost one-half of the acute stroke patients and was related to previous mood disorder but not to the type or location of the stroke. The profile of depressive acute stroke patients was characterized primarily by apathy/loss of interest.
Footnotes
Contributors: Drs. Caeiro, Ferro and Figueira designed the study. Dr. Caeiro acquired the data; Drs. Caeiro, Ferro and Santos analyzed it. Dr. Caeiro wrote the article, and Drs. Ferro, Santos and Figueira critically reviewed it. All authors gave final consent for publication.
Competing interests: None declared.
Correspondence to: Dr. Lara Caeiro, Hospital de Santa Maria CEEM, Serviço de Neurologia (piso 6), Av. Professor Egas Moniz, 1649-035 Lisboa, Portugal; fax +351 21 7957474; laracaeiro@fm.ul.pt
References
- 1.Berg A, Palomäki H, Pehtihalmes M, et al. Post-stroke depression in acute phase after stroke. Cerebrovasc Dis 2001;12:14-20. [DOI] [PubMed]
- 2.Aben I, Verhey F, Strik J, et al. A comparative study into the one-year cumulative incidence of depression after stroke and myocardial infarction. J Neurol Neurosurg Psychiatry 2003;74:581-5. [DOI] [PMC free article] [PubMed]
- 3.Carota A, Staub F, Bogousslavsky J. Emotions, behaviours and mood changes in stroke. Curr Opin Neurol 2002;15:57-69. [DOI] [PubMed]
- 4.Fedoroff JP, Starkstein SE, Parikh RM, et al. Are depressive symptoms non-specific in patients with acute stroke? Am J Psychiatry 1991;148:1172-6. [DOI] [PubMed]
- 5.Carota A, Staub F, Karapanayiotides T, et al. Behavioural changes and poststroke depression. J Neurology 2001;284 (Suppl 2):II/33.
- 6.Kellermann M, Fekete I, Gesztelyi R, et al. Screening for depressive symptoms in the acute phase of stroke. Gen Hosp Psychiatry 1999;21:116-21. [DOI] [PubMed]
- 7.Astrom M, Adolfsson R, Asplund K. Major depression in stroke patients. A 3-year longitudinal study. Stroke 1993;24:976-82. [DOI] [PubMed]
- 8.Bhogal SK, Teasell R, Foley N, et al. Lesion location and poststroke depression. Stroke 2004;35:794-802. [DOI] [PubMed]
- 9.Nys GMS, van Zandvoort MJE, van der Worp HB, et al. Early depressive symptoms after stroke: neuropsychological correlates and lesion characteristics. J Neurol Sci 2005;228:27-33. [DOI] [PubMed]
- 10.Robinson RG, Starr LB, Kubos KL, et al. A two-year longitudinal study of post-stroke mood disorders: findings during the initial evaluation. Stroke 1983;14:736-41. [DOI] [PubMed]
- 11.Shimoda K, Robinson RG. The relationship between poststroke depression and lesion location in long-term follow-up. Biol Psychiatry 1999; 45:187-92. [DOI] [PubMed]
- 12.Hackett ML, Yapa C, Parag V, et al. Frequency of depression after stroke: a systematic review of observational studies. Stroke 2005; 36: 1330-40. [DOI] [PubMed]
- 13.Robinson RG. Prevalence of depression disorders. In: Robinson RG, editor. The clinical neuropsychiatry of stroke. Cambridge: Cambridge University Press; 2006. p. 52-9.
- 14.Biran I, Chatterjee A. Depression with anosognosia following a left subcortical stroke. Clin Neurol Neurosurg 2003;105:99-101. [DOI] [PubMed]
- 15.Bogousslavsky J. William Feinberg lecture 2002. Emotions, mood and behaviour after stroke. Stroke 2003;34:1046-50. [DOI] [PubMed]
- 16.Robinson RG. Depression and lesion location in stroke. In: Bogousslavsky J, Cummings JL, editors. Behaviour and mood disorder in focal brain lesions. Cambridge: Cambridge University Press; 2000. p. 95-121.
- 17.Robinson RG, Kubos KL, Starr LB, et al. Mood disorders in stroke patients: importance of location of lesion. Brain 1984;107:81-93. [DOI] [PubMed]
- 18.Starkstein SE, Robinson RG, Honig MA, et al. Mood changes after right-hemisphere lesions. Br J Psychiatry 1989;155:79-85. [DOI] [PubMed]
- 19.Starkstein SE, Berthier ML, Fedoroff P, et al. Anosognosia and major depression in 2 patients with cerebrovascular lesions. Neurology 1990; 40:1380-2. [DOI] [PubMed]
- 20.Carson AJ, MacHale S, Allen K, et al. Depression after stroke and lesion location: a systematic review. Lancet 2000;356:122-6. [DOI] [PubMed]
- 21.Singh A, Herrmann N, Black SE. The importance of lesion location in poststroke depression: a critical review. Can J Psychiatry 1998;43: 921-7. [DOI] [PubMed]
- 22.Jennett B, Teasdale G. Aspects of coma after severe head injury. Lancet 1977;1:878-81. [DOI] [PubMed]
- 23.Brott T, Adams HP, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989;20:864-70. [DOI] [PubMed]
- 24.American Psychiatric Association (APA). Mood disorders. In: Diagnostic and statistical manual of mental disorders, 4th ed., text reviewed. Washington: the Association; 2002. p. 345-428.
- 25.Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry 1979;134:382-9. [DOI] [PubMed]
- 26.García-Portilla MPG, Férnandez MTB, Ojanguren BP, et al. Instrumentos de evaluación de los trastornos de ansiedad y depresivos en atención primaria. In: Garcia JB, García MB, García-Portilla MPG, et al, editors. Trastornos de ansiedad y trastornos depresivos en atención primaria. Barcelona: Masson; 2001. p. 57.
- 27.Singh A, Black SE, Herrmann N, et al. Functional and neuroanatomic correlations in post stroke depression. The Sunnybrook Stroke Study. Stroke 2000;31:637-44. [DOI] [PubMed]
- 28.Herrmann N, Black SE, Lawrence J, et al. The Sunnybrook Stroke Study: a prospective study of depressive symptoms and functional outcome. Stroke 1998;29:618-24. [DOI] [PubMed]
- 29.Gainotti G, Azzoni A, Lanzillotta M, et al. Some preliminary findings concerning a new scale for the assessment of depression and related symptoms of stroke patients. Ital J Neurol Sci 1995;16:439-51. [DOI] [PubMed]
- 30.Gainotti G, Azzoni A, Razzano C, et al. The post-stroke depression rating scale: a test specifically devised to investigate affective disorders of stroke patients. J Clin Exp Neuropsychol 1997;19:340-56. [DOI] [PubMed]
- 31.Guerreiro MS, Botelho MA, Leitão O, et al. Adaptação à população portuguesa da tradução do “Mini Mental State Examination” (MMSE). Revi Port Neurolog 1994:9-10.
- 32.Madureira S, Guerreiro M, Ferro JM. Dementia and cognitive impairment three months after stroke. Eur J Neurol 2001;8:621-7. [DOI] [PubMed]
- 33.Tatemichi TK, Foulkes MA, Mohr JP, et al. Dementia in stroke survivors in the Stroke Data Bank Cohort. Prevalence, incidence, risk factors and computed tomographic findings. Stroke 1990;21:858-66. [DOI] [PubMed]
- 34.Bamford JM, Sandercock PAG, Warlow CP, et al. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1989; 20:828. [DOI] [PubMed]
- 35.Carota A, Berney A, Aybek S, et al. A prospective study of predictors of poststroke depression. Neurology 2005;64:428-33. [DOI] [PubMed]
- 36.Simons LA. Risk factors for ischaemic stroke. Dubbo study of elderly. Stroke 1998;29:1341-6. [DOI] [PubMed]
- 37.Morris PL, Robinson RG, de Carvalho ML, et al. Lesion characteristics and depressed mood in the stroke data bank study. J Neuropsychiatry Clin Neurosci 1996;8:153-9. [DOI] [PubMed]
- 38.Starkstein SE, Robinson RG, Berthier ML, et al. Differential mood changes following basal ganglia vs thalamic lesions. Arch Neurol 1988;45:725-30. [DOI] [PubMed]
- 39.de Coster L, Leentjens AFG, Lodder J, et al. The sensitivity of somatic symptoms in post-stroke depression: a discriminant analytic approach. Int J Geriatr Psychiatry 2005;20:358-62. [DOI] [PubMed]
- 40.Marin RS, Biedrzycki RC, Firinciogullari S. Reliability and validity of the apathy evaluation scale. Psychiatry Res 1991;38:143-62. [DOI] [PubMed]
- 41.Fones CSL. Distinguishing apathy syndromes from vascular depression. Arch Gen Psychiatry 1998;55:844-5. [DOI] [PubMed]
- 42.Ghika-Schmid F, Bogousslavsky J. The acute behavioural syndrome of anterior thalamic infarction: a prospective study of 12 cases. Ann Neurol 2000;48:220-7. [PubMed]