

Abstract
Objective: Many knee rehabilitation studies have examined open and closed kinetic chain exercises. However, most studies focus on 2-legged, closed chain exercise. The purpose of our study was to characterize 1-legged, closed chain exercise in young, healthy subjects.
Subjects: Eighteen normal subjects (11 men, 7 women; age, 24.6 ± 1.6 years) performed unsupported, 1-legged squats and step-ups to approximately tibial height.
Measurements: Knee angle data and surface electromyographic activity from the thigh muscles were recorded.
Results: The maximum angle of knee flexion was 111 ± 23° for squats and 101 ± 16° for step-ups. The peak quadriceps activation was 201 ± 66% maximum voluntary isometric contraction, occurring at an angle of 96 ± 16° for squats. Peak quadriceps activation was 207 ± 50% maximum voluntary isometric contraction and occurred at 83 ± 12° for step-ups.
Conclusions: The high and sustained levels of quadriceps activation indicate that 1-legged squats and step-ups would be effective in muscle rehabilitation. As functional, closed chain activities, they may also be protective of anterior cruciate ligament grafts. Because these exercises involve no weights or training equipment, they may prove more cost effective than traditional modes of rehabilitation.
Keywords: one-legged squats, step-ups, functional exercise
Designing an optimal exercise regimen for knee rehabilitation continues to be a prevailing focus of sports medicine and physical therapy research. Much of the controversy surrounding knee rehabilitation concerns which type of exercise is most appropriate at various stages of rehabilitation. An example of this controversy is the ongoing debate over rehabilitation after anterior cruciate ligament (ACL) reconstruction.1–7 Given the frequency of ACL reconstruction and the lengthy rehabilitation that follows, the search for an optimal recovery regimen involving the most beneficial types of exercise is an important endeavor. While many modes of rehabilitation exercise have been used, much of the current debate centers on the risks and benefits of open versus closed kinetic chain exercise.
The concept of open and closed chain kinetic exercises comes from linkage analysis in mechanical engineering. In 1955, Steindler suggested that the human body could be represented by a chain of rigid segments connected by a series of joints.8 He observed that the pattern of muscle recruitment in the leg was different when the foot was fixed than when the foot was free. The term closed chain describes exercise in which the distal appendage is fixed, as in a squat or a pull-up. Open chain refers to movements in which the foot or hand is relatively free, such as during seated knee extension or throwing a baseball.
Both open and closed chain exercises have been studied extensively to determine their proper place in rehabilitation following ACL reconstructive surgery.2,4,7,9–12 The results of cadaveric research,9,13 biomechanical analyses,14,15 and tibial translocation studies12 suggest that closed chain exercises result in reduced anterior tibial shear force and decreased ACL strain, while open chain exercises produce greater anterior tibial shear forces and increased ACL strain, especially at 0° to 45° of extension. Still, open chain exercise continues to be an important rehabilitation tool. Open chain isokinetic exercise is widely used in evaluating strength recovery after ACL reconstruction, and previous studies demonstrated higher levels of target muscle activation during open chain exercises than during closed chain maneuvers.3–7 However these findings are somewhat deceptive because open chain leg extensions involve a single leg, while previously studied closed chain exercises are 2-legged activities.
The purpose of our study was to quantitatively characterize the activation of the quadriceps during 1-legged, closed chain exercises in young, recreationally athletic men and women. One-legged exercises were chosen for their potential for increased levels of muscle activation and their utility in practical rehabilitation settings. Additionally we wished to study maneuvers (1-legged squats and step-ups) that would not require the use of free weights or expensive weight-training machines.
MATERIALS AND METHODS
Subjects
Written consent in accordance with institutional review board policy was obtained from 11 men and 7 women (age = 24.6 ± 1.6 years, height = 174.2 ± 8.6 cm, weight = 67.9 ± 10.3 kg). The subjects had no history of prior knee injury or knee surgery. The institutional review board also approved the study.
Before testing, the skin surrounding the knee joint was shaved and cleaned with isopropyl alcohol to ensure adequate surface contact for electrodes. Two silver/silver chloride 3M Red Dot surface electrodes (St Paul, MN) were placed by a single investigator on the subject's dominant side (the arm with which the subject would prefer to throw a baseball) over the muscle bellies of the vastus lateralis, vastus medialis oblique, rectus femoris, and biceps femoris using anatomical landmarks described by Perotto.18 The interelectrode distance was approximately 4 cm. A single ground electrode was placed on the ulnar styloid of the ipsilateral forearm. Electrical impedance was determined and verified to be less than 2 kΩ.
An electrogoniometer (Noraxon USA Inc, Scottsdale, AZ) was attached to the lateral aspect of the subject's leg. A single investigator positioned the electrogoniometer along a line passing through the greater trochanter, the lateral femoral condyle, and the lateral malleolus. Double-sided tape was used to secure the electrogoniometer during positioning. Once in position, the goniometer was anchored more firmly to the skin using transverse strips of 3M Blenderm surgical tape. The subject was then instructed to stand upright, and the electrogoniometer was set to 0°.
For each trial, the analog data from the electromyographic (EMG) leads and the goniometer was sampled and processed with the Noraxon Telemyo System. Muscle activity signals were collected by the surface electrodes and passed to a battery-operated FM transmitter (Noraxon USA Inc) worn by the subject. The transmitter contained a single-ended amplifier that filtered at a bandwidth of 15 to 500 Hz and had a common-mode rejection ratio of 130 dB and a receiver that converted the signal from analog to digital data with an analog-to-digital card. From the transmitter, the signal was sent to the computer, where the raw EMG and goniometer data were sampled at a frequency of 1000 Hz and analyzed by the Myoresearch software package (Noraxon USA Inc).
Experimental Protocol
Each subject performed 1-legged squats, step-ups, and maximum isometric voluntary contractions (MVICs). The performance order of the squats and step-ups was randomly selected using a random number table. Maximum isometric voluntary contractions were performed last. The subjects were given the opportunity to practice each exercise until comfortable with their performance. Each subject then performed the squats and step-ups in 3 sets of 1 repetition each. A rest period of 1 minute was given between sets, between exercises, and between MVICs.
One-legged squats were performed by having the subjects stand on the instrumented leg with the arms outstretched and touching a vertical pillar. The subjects were instructed to use the pillar only to aid with balance. They were then asked to squat down as low as possible and rise again to the upright position using only the instrumented leg. If subjects lost their balance, could not rise in a smooth motion, or were judged to have used the pillar to pull themselves upright, the trial was discarded and the exercise was performed again after the 1-minute rest period.
Step-ups were performed by having the subjects place the foot of the instrumented leg on a step of approximately tibial plateau height (step height was adjusted for each subject). The subjects were instructed to step up to full extension of the instrumented leg and then return to the original position using only the instrumented leg. To ensure that the subjects did not push off the contralateral leg, they were required to stand on the heel of the uninstrumented leg, maintaining the toes dorsiflexed off the ground and the uninstrumented knee locked in full extension for the entire concentric portion of the step-up. To aid in their performance of this maneuver, subjects were instructed to bend their torsos forward over the instrumented knee. If a subject did not rise in a smooth motion or was judged to have pushed off the uninstrumented leg, the trial was discarded and the exercise was performed again after the 1-minute rest period. If a subject could not perform the exercise correctly after repeated attempts, the step was lowered 3 cm and the exercises were repeated. Three subjects (1 man, 2 women) were unable to perform step-ups at tibial plateau height. Each was able to perform the exercise with the step height lowered by 3 cm.
Maximum isometric voluntary contractions were measured with the subject sitting upright on a leg exercise chair with a padded leg extension-flexion bar contacting the distal leg. Care was taken to ensure that the hinge center on the machine arm was aligned with the knee joint center. The subject was secured in the seat with thigh, hip, and shoulder straps. Quadriceps MVICs were collected by asking the subjects to extend their legs as hard as possible for 5 seconds against the extension bar, which was locked at 90° of flexion. After a 1-minute rest period, the exercise was repeated at 60° of flexion and then at 30° of flexion after an additional 1-minute rest period. Hamstrings MVICs were collected at the same degrees of knee flexion with the same equipment, with the subjects flexing their legs as hard as possible for 5 seconds.
Data Analysis
We analyzed MVICs by integrating the rectified EMG signals and finding the greatest 1 second of activation for each of the muscles during each trial (30°, 60°, and 90°). This 1 second of greatest activation for each muscle from any trial was assigned 100% of EMG activity for that muscle. The maximum integrated EMG (IEMG) of the rectus femoris and the vastii were summed to obtain a value assigned as 100% of IEMG activity for the quadriceps (quadriceps MVIC). The maximum biceps femoris IEMG was assigned as 100% of the IEMG activity for hamstrings per second (hamstrings MVIC). We used these values to normalize the dynamic contractions recorded during the squats and step-ups. The squat and step-up data were analyzed over 10° arcs of knee flexion during the concentric and eccentric portions of exercise. The rectified EMG signals from the rectus and vastii muscles were integrated over these 10° arcs of motion and then summed to create a combined quadriceps IEMG for each arc. The quadriceps IEMG for each arc was then divided by the time-weighted quadriceps MVIC and multiplied by 100 to express the quadriceps activation for each 10° arc as a percentage of the quadriceps MVIC (MVIC%). The same methods were used to calculate the MVIC% for the hamstrings.
Data were summarized by routine descriptive statistics. Significant differences (P ≪ .05) were determined by repeated-measures analysis of variance with 1 grouping factor (sex) and 2 repeated factors (exercise and knee angle interval).
RESULTS
For the squat and step-up exercises, the maximum angle of knee flexion, angle of maximum quadriceps activation, and maximum quadriceps activation are summarized in Table 1. The male versus female differences in maximum quadriceps activation were not significant. However, the differences in maximum angle of knee flexion and angle of maximum quadriceps activation were significant (P ≪ .05). Men squatted to deeper angles of knee flexion and produced their maximum quadriceps contraction at greater knee-flexion angles than women.
Table 1. Electromyographic Analysis by Sex and Exercise*
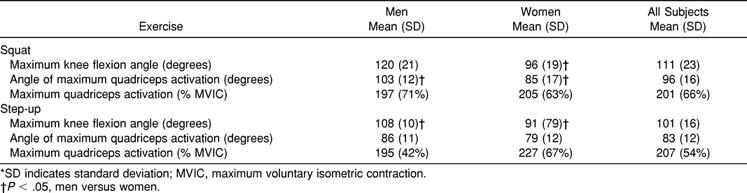
For the step-up exercise, the male versus female differences in angle of maximum quadriceps activation and maximum quadriceps activation were not significant. However, the maximum angle of knee flexion was significantly greater (P ≪ .05) for the male group.
Quadriceps activation did not differ between men and women over the arcs of motion ending at 90°, 60°, and 30°. Accordingly, the data were pooled and expressed for all subjects. Three subjects could not perform a 90° range of motion and were excluded. The quadriceps and hamstrings activation over each arc of motion with n > 14 is summarized for squats (Figure 1) and step-ups (Figure 2). The difference in quadriceps activation among 90°, 60°, and 30° was highly significant (P ≪ .0001) for the eccentric and the concentric portions of both the squats and the step-ups. No significant difference was seen between squats and step-ups in concentric activation at 90°, 60°, or 30°.
Figure 1.
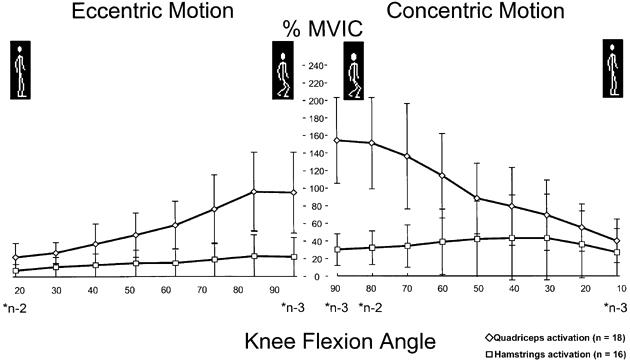
Relative quadriceps and hamstrings activation during 1-legged squats.
Figure 2.
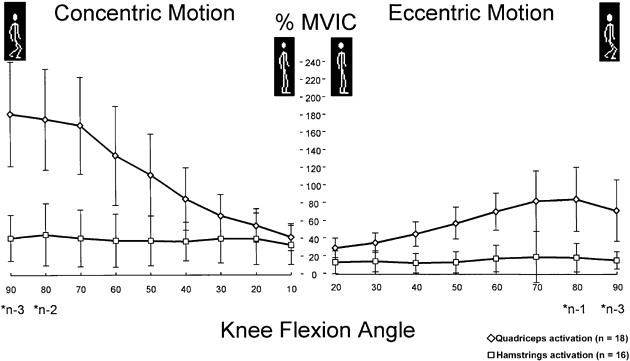
Relative quadriceps and hamstrings activation during 1-legged step-ups.
However, the eccentric quadriceps activation at 30° was greater for step-ups (36 ± 11% MVIC) than for squats (26 ± 12% MVIC, P = .067). In contrast, the eccentric activation at 90° was significantly greater for squats (95 ± 29% MVIC) than for step-ups (72 ± 36% MVIC, P = .045). Eccentric quadriceps activation was not significantly different (P = .185) between squats and step-ups at 60° of knee flexion.
The hamstrings electrodes of 2 subjects became detached during the exercises and were not discovered until after the test. Consequently, these data could not be reported; thus, 16 subjects had complete hamstrings data. The maximum hamstrings activation was 81 ± 74% MIVC, occurring at 86 ± 33° for squats, and 59 ± 37% MVIC, occurring at 65 ± 14° for step-ups. No significant differences in hamstrings data were noted between men and women.
DISCUSSION
The peak levels of quadriceps activation achieved by subjects in this study were 201 and 207% MVIC for squats and step-ups, respectively, approximately double the maximum activation measured during isometric exercise. Exercises that elicit maximal voluntary muscular contraction have been shown to be very effective in increasing muscular strength.16,19–21 The peak levels of quadriceps activation achieved in our study are more than double those reported by Isear et al22 and Gryzlo et al4 in unloaded 2-legged squats. Stuart et al10 and Wilk et al16 recorded quadriceps activation during loaded, 2-legged, closed chain exercises, and the quadriceps activation achieved by subjects in our study is roughly double that reported by both groups. Some important differences in method and subject selection exist between the trials. First, both Stuart et al10 and Wilk et al16 used free weights to increase resistance during exercise; no weights were used in our study. Second, Wilk et al's subjects were trained weight lifters and Stuart et al's trial included only male subjects. Our subject pool consisted of young, recreational male and female athletes. Also interesting to note is that the quadriceps activation for 1-legged squats and step-ups remained greater than 100% MVIC at 60° of flexion in our study. Both the peak and the sustained levels of activation suggest that 1-legged squats and step-ups are effective in achieving a maximal voluntary muscular contraction and would be effective in strength building for men and women. One possible advantage is that these 1-legged exercises involve neither free weights nor weight-training equipment. Hence, they may prove more cost effective than traditional modes of rehabilitation.
A second important feature of these 1-legged exercises is that they involve closed chain joint kinetics. Closed chain exercises have been associated with decreased ACL strain. While the safe or optimal level of strain for newly implanted ACL autografts remains unknown,1,5,6 most physicians and therapists have assumed that exercises that effectively strengthen the quadriceps muscles while producing less ACL strain are desirable.1,3,12,16 Results of cadaveric studies by More et al,9 Markolf et al,13 and Arms et al23 suggest that squatting produces significantly less ACL strain than seated leg extension, especially between 0 and 30° of knee flexion. Mathematical models of the biomechanical forces occurring in the knee joint have also been used to estimate ACL shear forces.14–17 Nisell14 and Wilk et al16 concluded that open chain exercises result in anterior shear and ACL stress, with peak values approaching 700 Newtons (or 1 body weight) at approximately 30° of knee flexion. However, closed chain exercises result in posterior tibiofemoral shear forces throughout the range of motion.14,16 These results are identical with those obtained by other investigators, who also demonstrated that increasing resistance during open chain exercise led to a nonlinear increase in anterior shear force,24,25 while increasing resistance during closed chain exercise did not significantly increase tibiofemoral shear force in a recent in vivo study.3 Finally, studies measuring anterior tibial displacement have been used to determine ACL stress during exercise. Yack et al12 and Drez et al26 found significantly less anterior tibial translation during closed chain exercise, especially in ACL-deficient knees. Clearly, exercises with closed chain biomechanics similar to the 1-legged exercises studied here produce less anterior shear force than open chain maneuvers. In addition, the closed chain, 1-legged exercises in our study involve increased torso flexion, which has been shown to further decrease the anterior component of the tibiofemoral shear force.16
Closed chain exercise also results in decreased anterior tibial shear force because the maximum quadriceps activation occurs at deep angles of knee flexion.11,12 Cadaveric analysis shows that the highly activated quadriceps can pull the tibial forward and stress the ACL between 0 and 45° of knee flexion.23,27 Studies of open chain exercises show maximum levels of quadriceps activation between 45° and 0 degrees of knee flexion.16,18 However, closed chain exercises maximally activate the quadriceps at angles of knee flexion greater than 45°.11,16,12 The 1-legged squats and step-ups in this study also demonstrated peak activation at knee flexion angles well away from the demonstrated “danger zone” for anterior tibial pull by the quadriceps (96 ± 16° in squats, 83 ± 12° in step-ups). Within the “danger zone,” at 30° of flexion, the 1-legged squats and step-ups had relatively low quadriceps activation levels of 69% MVIC and 67% MVIC, respectively.
Another potential stabilizing force at the tibiofemoral joint is hamstring cocontraction.8,22 Most published reports show a constant, low-level hamstring activity throughout the exercise cycle in 2-legged, closed-chain exercise.4,21,22 We found an average biceps femoris activation of roughly 20% to 40% MVIC throughout the exercise cycle, which is consistent with these previously reported results. Our hamstrings data displayed much higher intrasubject and intersubject variability than did our quadriceps data, making further interpretation and description difficult. Typical coefficients of variation ranged from 20% to 30% for quadriceps data and from 70% to 90% for the corresponding hamstrings parameters. Additionally, our hamstrings data reflected only EMG activity monitored from electrodes placed over the biceps femoris muscle, ignoring the contribution of the lateral semimembranosus and semitendinosus muscles. We also made no effort to control for hip angle, which may be an important factor in hamstrings activation.12 The primary purpose of our study was to characterize quadriceps activation; the hamstrings results are reported here for completeness.
The angle required to achieve maximal quadriceps contraction with a 1-legged squat or step-up may differ among groups of individuals. During the 1-legged squat exercise, the maximum angle of knee flexion and the angle of maximum quadriceps activation were significantly greater for men (120° and 103°, respectively) than for women (108° and 86°). Yet the level of maximum quadriceps activation was not significantly different between the 2 groups (197% MVIC in men, 206% MVIC in women). These data suggest that though the female subjects did not squat as low on average as their male counterparts, 1-legged squats would be equally effective for building quadriceps strength in men and women, because both groups were exercising at close to maximum-level quadriceps capacity.
The same trend did not exist for the step-up. Although the maximum angle of knee flexion was significantly greater for men (108°) than for women (91°), the angle of maximum quadriceps activation was not significantly different between the 2 groups (men, 86°; women, 79°; P = .187). However, when performing a 1-legged squat, the subject was instructed to squat down as low as possible while still being able to arise using only that leg. When attempting the 1-legged step-ups, subjects first attempted to step up onto a platform of knee height. If they could not perform the step-up correctly at this height, the platform was lowered until they could perform the exercise. Yet, if they were successful at knee height, no trial of increased platform height was attempted. Thus, the maximum angle and maximum angle of quadriceps activation during step-ups may exhibit a negative skew, obscuring the true difference between the 2 groups. Despite this variation in the methods, the maximum quadriceps activation was not significantly different between men (195% MVIC) and women (227% MVIC), nor was the maximum quadriceps activation significantly different between squats (201% MVIC) and step-ups (207% MVIC) for all subjects. One-legged squats and step-ups appear to be equally effective in maximally activating the quadriceps of both male and female participants.
Differences existed between the eccentric phases of 1-legged squats and step-ups. The differences in eccentric quadriceps activation at 30° and 90° likely reflect the differing patterns of eccentric “braking” that are required by the 2 maneuvers. While performing a squat, 90° of eccentric motion occurs immediately before a change of direction (ie, beginning the concentric, rising motion). Hence, a high level of eccentric activation is expected as the quadriceps slow the fall of the torso before the concentric exercise begins. However in a step-up, 90° of eccentric motion occurs just before heel strike. Logically then, less eccentric activity would be expected than in the former scenario because most of the energy of stopping is provided by the heel strike of the contralateral leg. The statistical difference at 30° is likely of less functional significance but appears to reflect an increased initial “braking” in step-ups to lessen the impact forces of the upcoming heel strike.
Closed chain exercises have also been thought to recruit muscles in functional, familiar patterns.22,28 Theoretically, this should result in less time being spent in the initial learning phase of strength building (reduction of the pretraining effect) and more rapid entry into the muscular building phase of strength training.16,29,30 Additionally, recruiting and activating muscles in such functional patterns may improve proprioception and coordination, leading to decreased rates of injury.31,32 These theoretic benefits have not been proven conclusively, since few long-term comparisons of closed and open chain rehabilitation have been reported.1,2 However, should initial studies prove correct in predicting these beneficial training effects, 1-legged exercises may also provide these benefits due to their functional, closed chain kinetics. In fact, the balance required to perform 1-legged exercises might further enhance the coordination and proprioceptive aspects of rehabilitation. More research with studies designed specifically to test these variables are needed to better understand the role of balance and proprioception in rehabilitation.
Finally, 1-legged exercises might be useful in assessing the functional recovery of a patient without isokinetic testing. With only 1 leg used to perform the exercise, functional comparisons can easily be made between the involved and uninvolved legs. The height to which a patient can step up or the angle to which he or she can squat with the involved versus the uninvolved leg may provide valuable information concerning the stage of functional recovery. Further research comparing these 1-legged exercises in normal subjects and patients with ACL reconstructions is ongoing at this time.
CONCLUSIONS
One-legged squats and step-ups in young, athletically active men and women yield levels of quadriceps activation sufficiently high enough for strength building. Further investigation is needed to assess these exercises in postsurgical patients and to further compare these exercises with other traditional modes of rehabilitation therapy.
Acknowledgments
ACKNOWLEDGMENTS
We thank Scott Colby, Jason Hurst, and Anthony Francisco for their technical expertise in designing and carrying out this project and Drs Michael Gross and Kevin Guskiewicz for their assistance in preparing the manuscript.
This project was supported in part by a grant from Nike Incorporated, Beaverton, OR. No author or related institution has received any financial benefit from research in this study. This project was performed in the Coach Krzyzewski Human Performance Laboratory, Department of Orthopaedic Surgery and Sports Medicine, Duke University, Durham, NC.
The opinions expressed are those of the authors and do not represent official policy of the Department of the Air Force or the Department of Defense.
REFERENCES
- Beynnon B D, Johnson R J. Anterior cruciate ligament injury rehabilitation in athletes: biomechanical considerations. Sports Med. 1996;22:54–64. doi: 10.2165/00007256-199622010-00005. [DOI] [PubMed] [Google Scholar]
- Bynum E B, Barrack R L, Alexander A H. Open versus closed chain kinetic exercises after anterior cruciate ligament reconstruction: a prospective randomized study. Am J Sports Med. 1995;23:401–406. doi: 10.1177/036354659502300405. [DOI] [PubMed] [Google Scholar]
- Frndak P H, Berasi C C. Rehabilitation concerns following anterior cruciate ligament reconstruction. Sports Med. 1991;2:338–346. doi: 10.2165/00007256-199112050-00006. [DOI] [PubMed] [Google Scholar]
- Gryzlo S M, Patek R M, Pink M, Perry J. Electromyographic analysis of knee rehabilitation exercises. J Orthop Sports Phys Ther. 1994;20:36–43. doi: 10.2519/jospt.1994.20.1.36. [DOI] [PubMed] [Google Scholar]
- Shelbourne K D, Patel D V. Rehabilitation after autogenous bone-patellar tendon-bone ACL reconstruction. Instr Course Lect. 1996;45:263–273. [PubMed] [Google Scholar]
- Shelbourne K D, Rowdon G A. Anterior cruciate ligament injury: the competitive athlete. Sports Med. 1994;17:132–140. doi: 10.2165/00007256-199417020-00005. [DOI] [PubMed] [Google Scholar]
- Stanish W D, Lai A. New concepts of rehabilitation following anterior cruciate reconstruction. Clin Sports Med. 1993;12:25–58. [PubMed] [Google Scholar]
- Palmitier R A, An K N, Scott S G, Chao E Y. Kinetic chain exercise in knee rehabilitation. Sports Med. 1991;11:402–413. doi: 10.2165/00007256-199111060-00005. [DOI] [PubMed] [Google Scholar]
- More R C, Karras B T, Neiman R, Fritschy D, Woo S L, Daniel D M. Hamstrings—an anterior cruciate ligament protagonist: an in vitro study. Am J Sports Med. 1993;21:231–237. doi: 10.1177/036354659302100212. [DOI] [PubMed] [Google Scholar]
- Stuart M J, Meglan D A, Lutz G E, Growney E S, An K N. Comparison of intersegmental tibiofemoral joint forces and muscle activity during various closed kinetic chain exercises. Am J Sports Med. 1996;24:792–799. doi: 10.1177/036354659602400615. [DOI] [PubMed] [Google Scholar]
- Wilk K E, Andrews J R. The effects of pad placement and angular velocity on tibial displacement during isokinetic exercise. J Orthop Sports Phys Ther. 1993;17:24–30. doi: 10.2519/jospt.1993.17.1.24. [DOI] [PubMed] [Google Scholar]
- Yack H J, Collins C E, Whieldon T J. Comparison of closed and open kinetic chain exercise in the anterior cruciate ligament-deficient knee. Am J Sports Med. 1993;21:49–54. doi: 10.1177/036354659302100109. [DOI] [PubMed] [Google Scholar]
- Markolf K L, Gorek J F, Kabo J M, Shapiro M S. Direct measurement of resultant forces in the anterior cruciate ligament: an in vitro study performed with a new experimental technique. J Bone Joint Surg Am. 1990;72:557–567. [PubMed] [Google Scholar]
- Nissell R. On the biomechanics of the knee: a study of joint and muscle load with applications in ergonomics, orthopaedics and rehabilitation. Acta Orthop Scand. 1985;216:1–42. [PubMed] [Google Scholar]
- Noonan T J, Garrett W E. Orlando, FL: The patellar tendon-tibial shaft angle and its relation to non-contact injury of the ACL. Paper presented at: American Academy of Orthopaedic Surgeons' Annual Meeting. February 16-21 1995. [Google Scholar]
- Wilk K E, Escamilla R F, Fleisig G S, Barrentine S W, Andrews J R, Boyd M L. A comparison of tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. Am J Sports Med. 1996;24:518–527. doi: 10.1177/036354659602400418. [DOI] [PubMed] [Google Scholar]
- Ohkoshi Y K, Yasuda K, Kaneda K, Wada T, Yamanaka M. Biomechanical analysis of rehabilitation in the standing position. Am J Sports Med. 1991;19:605–611. doi: 10.1177/036354659101900609. [DOI] [PubMed] [Google Scholar]
- Perotto A P. Anatomical Guide for the Electromyographer. 3rd ed Charles C. Thomas Publishers; Springfield, IL: 1994. [Google Scholar]
- Berger R A, Hardage B. Effect of maximum loads for each of ten repetitions on strength improvement. Res Q. 1967;38:715–718. [PubMed] [Google Scholar]
- Fleck S J, Schutt R C., Jr Types of strength training. Orthop Clin North Am. 1983;4:449–458. [PubMed] [Google Scholar]
- Withers R T. Effect of varied weight-training loads on the strength of university freshmen. In: Fleck S J, Kraemer W J, editors. Designing Resistance Training Programs. Human Kinetics; Champaign, IL: 1987. [PubMed] [Google Scholar]
- Isear J A, Jr, Erickson J C, Worrell T W. EMG analysis of lower extremity muscle recruitment patterns during an unloaded squat. Med Sci Sports Exerc. 1997;29:532–539. doi: 10.1097/00005768-199704000-00016. [DOI] [PubMed] [Google Scholar]
- Arms S W, Pope M H, Johnson R J, Fischer R A, Arvidsson I, Eriksson E. The biomechanics of anterior cruciate ligament rehabilitation and reconstruction. Am J Sports Med. 1984;12:8–18. doi: 10.1177/036354658401200102. [DOI] [PubMed] [Google Scholar]
- Hirokawa S, Solomonow M, Lu Y, Lou Z P, D'Ambrosia R. Anterior-posterior and rotational displacement of the tibia elicited by quadriceps contraction. Am J Sports Med. 1992;20:299–306. doi: 10.1177/036354659202000311. [DOI] [PubMed] [Google Scholar]
- Lutz G E, Palmitier R A, An K N, Chao E Y. Comparison of tibiofemoral joint forces during open-kinetic-chain and closed-kinetic-chain exercises. J Bone Joint Surg Am. 1993;75:732–739. doi: 10.2106/00004623-199305000-00014. [DOI] [PubMed] [Google Scholar]
- Drez D, Paine R, Neushwander D C. In vivo testing of closed versus open kinetic chain exercises in patients with documented tears of the anterior cruciate ligament. Orthop Trans. 1992;16:43. [Google Scholar]
- Renstrom P, Arms S W, Stanwyck T S, Johnson R J, Pope M H. Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med. 1986;14:83–87. doi: 10.1177/036354658601400114. [DOI] [PubMed] [Google Scholar]
- Shelbourne K D, Nitz P. Accelerated rehabilitation after anterior cruciate ligament rehabilitation. Am J Sports Med. 1990;18:292–299. doi: 10.1177/036354659001800313. [DOI] [PubMed] [Google Scholar]
- Fleck S J, Kraemer W J, editors. Designing Resistance Training Programs. Human Kinetics; Champaign, IL: 1987. [Google Scholar]
- Hakkinen K. Factors influencing trainability of muscular strength during short-term and prolonged training. Natl Strength Condition J. 1985;7:32–327. [Google Scholar]
- Hewett T E, Lindenfeld T N, Riccobene J V, Noyes F R. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27:699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- Hewett T E, Stroupe A L, Nance T A, Noyes F R. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]