

Abstract
Objective: To examine the effects of repetitive impact forces on lacrosse helmets and increase awareness of helmet safety standards about reconditioning and recertification practices.
Design and Setting: The independent variables for this study consisted of 4 lacrosse helmets of various design: 2 contemporary helmets (Sport Helmets Cascade and Cascade Air) and 2 traditional helmets (Sport Helmets Ultralite and Bacharach Ultralite). The dependent variable was attenuation of impact forces as measured by the Gadd Severity Index (GSI). Helmets were tested at an independent testing facility certified by the National Athletic Equipment Reconditioners Association.
Measurements: Helmets were raised to 152 cm and released onto an anvil padded with a 1.27-cm rubber modular elastomer programmer. Ten treatments to a front (FD) and right rear boss drop site (RD) were performed. A triaxial accelerometer within the head form measured impact force. Peak acceleration data were integrated into the GSI. We performed a 1-way analysis of variance and calculated descriptive statistics and the Tukey post hoc test.
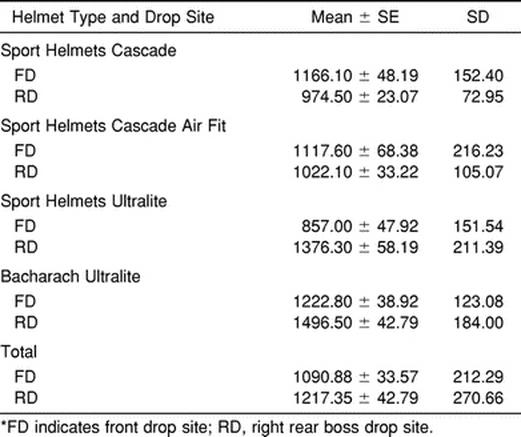
Results: A statistically significant difference was seen in FD GSI score (F3,36 = 9.680, P < .05) and in the RD GSI score (F3,36 = 28.140, P < .05) between helmet types. Mean GSI scores were 1166.1, 1117.6, 857, and 1222.8 for the FD and 974.5, 1022.1, 1376.3, and 1496.5 for the RD for Sport Helmets Cascade, Cascade Air, Ultralite, and Bacharach Ultralite, respectively. With repetitive drops, GSI scores increased, indicating a greater chance for cerebral injury. Percentage increases in GSI scores from drops 1 to 10 were 48.8, 54.3, 45.6, and 18.8 on the FD and 22.6, 35.9, 71.7, and 57.4 on the RD for the Sport Helmets Cascade, Cascade Air, Ultralite, and Bacharach Ultralite, respectively.
Conclusions: Our findings indicate differences between helmets at the 2 drop sites and decreasing capacity of the helmets to dissipate forces with repetitive impacts.
Keywords: Gadd Severity Index, National Operating Committee on Standards for Athletic Equipment, head injury
An estimated 300 000 sport-related traumatic brain injuries occur annually in the United States.1,2 Athletes who participate in contact sports, such as men's lacrosse, are at particular risk. Lacrosse is the oldest sport in North America and originated with Native American Indians.3–6 Comparable with football and ice hockey, men's lacrosse involves high-mass, high-velocity, body-to-body collisions and low-mass, high-velocity, object-to-body impacts3–5 that are inherent to the sport and can cause serious, life-threatening injuries.7–10 During the 1999 National Collegiate Athletic Association men's lacrosse season, head injuries accounted for 13% of game-related incidents, with most of those diagnosed as concussions.11 The precise threshold at which acute traumatic brain injury occurs is unknown. Children who have experienced a previous head injury face an increased risk of traumatic brain injury.2,12,13 Repeated mild brain injury may cause cumulative damage and lead to chronic neurologic sequelae.14,15
To prevent injury, male lacrosse players are required to wear helmets. In recent years, manufacturers have redesigned helmets in an effort to improve their products. The new designs are lighter, shaped differently than traditional lacrosse helmet designs, and popular (they are worn by most players at secondary and collegiate-level institutions). However, some athletic trainers have postulated that these new helmets may increase the risk of cerebral concussions in men's lacrosse players.5
Helmet manufacturers and reconditioners test helmets and use quantitative criteria to ensure that consumers have a reasonable level of protection. Tolerance curves, such as the Head Injury Criterion and the Gadd Severity Index (GSI), have been developed. These tolerance curves define a criterion for distinguishing between impacts likely to produce brain injury from impacts that are less serious.2,16–18 However, in lacrosse, no revisions have been implemented in the GSI standards since 1990.19 Therefore, the purpose of our study was to examine various lacrosse helmets, comparing each design based on its ability to attenuate forces when subjected to repetitive impacts. We hope that our results will promote increased awareness regarding the importance of improving helmet safety standards while adhering to proper reconditioning and recertification practices.
METHODS
Helmets
We used 4 new National Operating Committee on Standards for Athletic Equipment (NOCSAE)–approved helmets in our study. Two were contemporary-model lacrosse helmets: the Sport Helmets Cascade (SC) and Cascade Air Fit (SA) (Sport Helmets, Liverpool, NY). Two were traditional-model lacrosse helmets: the Bacharach Ultralite (BU) (Bacharach Rasin Sporting Goods, Towson, MD) and Sport Helmets Ultralite (SU) (Sport Helmets, Liverpool, NY) (Figure 1, Figure 2, Figure 3, Figure 4). All helmets were of medium size and designed to fit a human head measuring 58.8 to 59.9 cm in circumference. All helmets possessed sun visors. Helmets were stressed in a guided free fall using a NOCSAE-recommended head form, triaxial accelerometer, and drop testing carriage assembly (Southern Impact Research Center, Knoxville, TN).
Figure 1.

Sport Helmets Cascade contemporary design model. Photo courtesy of Sport Helmets.
Figure 2.

Sport Helmets Cascade Air Fit contemporary design model.
Figure 3.

Sport Helmets Ultralite traditional design model.
Figure 4.

Bacharach Ultralite traditional design model.
Instrumentation
The NOCSAE head form, which was developed by Dr Voigt Hodgson at Wayne State University, has a high degree of biofidelity, accurately simulating the human head response to impact accelerations.20,21 The medium-sized head form measures 575 mm in circumference and weighs 4.8 kg, including the neck. It incorporates a 3-dimensional piezoelectric accelerometer (354MO3, PCB Piezotronics, Inc, Depew, NY), mounted at the center of gravity, and glycerin is sealed in the cranium. A polychlorinated biphenyl triaxial accelerometer (354MO3) is designed to measure the peak acceleration of gravity in 3 orthogonal directions: the x-axis (anterior-posterior), the y-axis (superior-inferior), and the z-axis (left to right).2,21–28 The peak acceleration of gravity occurs at the head form's moment of impact.
Evaluative Criteria
The GSI is a commonly used biomechanical criterion that provides researchers with a standard to evaluate sport helmet safety.28 The GSI is defined as a measure of the severity of impact with respect to the immediate acceleration experienced by the head form at impact16,17,20–23,25,26:
 |
where T = pulse duration in seconds, A = acceleration in g, 2.5 = weighting factor, and t = time interval in seconds.
The GSI predicts a helmet's ability to decrease forces at impact and effectively protect the brain.28 The NOCSAE sets standard GSI threshold limits for the increased probability of sustaining a cerebral injury. These GSI values may not exceed 1200 for football helmets and 1500 for lacrosse helmets.2,19–26,29
Calibration Protocol
Before data collection, the triaxial accelerometer located at the head form's center of gravity was calibrated according to the NOCSAE protocol by dropping a medium-sized NOCSAE head form. The head form, without helmet, was released from 3 specified heights onto an anvil padded with a calibration modular elastomer programmer (MEP) (Southern Impact Research Center, Knoxville, TN). The calibration MEP pad rests on top of the anvil and is a 7.6 × 15.2-cm-diameter cushion molded from polyurethane thermoplastic elastomer.
Calibration began with a drop to the front of the head form from a height of 144.7 cm, followed by a drop to the side from 132 cm, and finally a drop to the crown from 111.7 cm. Resulting GSI values for each of the 3 drops were within acceptable limits (1200 GSI ± 2%). Air and helmet temperature were ambient and maintained at 22°C ± 2°C, as recommended by NOCSAE.19,29–31
Test Protocol
After calibration, helmets were placed on a medium-sized NOCSAE head form. Their intended model face masks were intact, and 4-point buckle systems were fastened according to manufacturers' specifications. Helmet positioning was checked before each impact test. The helmet's ear holes were aligned concentric with the head form's index ear holes, and the helmet's front rim was positioned properly by using a nose gauge.19
Helmets were raised using the carriage assembly to a height of 152 cm, as specified by NOCSAE standards (Figure 5). Next, the helmets were released in a gravity-induced free fall. Two wires guided the helmets into a rigid anvil padded with a 1.3 × 15.2-cm-diameter, 45-durometer hardness testing MEP pad (Southern Impact Research Center, Knoxville, TN) that is designed to simulate the playing surface (Figure 6).19,23–27,32–34 First, all helmets hit the front drop site (FD) 10 times, mimicking a head-on collision. This was followed by 10 impacts to a right rear boss drop site (RD), mimicking a blind-sided impact. The front impact location was adjusted to ensure the helmets hit the MEP without contacting the visor.19,20,29,32–34 Approximately 60 seconds separated successive impacts to a specified helmet at both the FD or RD treatments.19 Approximately 80 ± 5 minutes separated all helmets' FD and RD treatments. Each helmet was tested 20 times, for a total of 80 impact tests.
Figure 5.

Drop testing carriage assembly with head form and contemporary helmet in testing position for a front drop test.
Figure 6.

Front drop impact location onto anvil and testing modular elastomer programmer pad with a contemporary helmet design.
Data Analysis
Impact attenuation was determined for each helmet by measuring the head form's resulting peak instantaneous acceleration on contacting the MEP pad. Results for the 3 orthogonal axes were recorded by the head form's internally mounted triaxial accelerometer (Figures 5 and 6).19–22,29,32–34
Statistical Analysis
To analyze impulse criteria, we used a NOCSAE-recommended Severity Index Computer (KME Series 200 Data Analyzer, KME Co, Troy, MI). The computer recorded impulse signals from the triaxial accelerometer using a 4-pole, 1650-Hz filter, then used an integration equation to synthesize data into the GSI.19,32–34,35 Two 1-way analyses of variance, taking into account variations due to helmet design, were performed to determine whether the treatment of repetitive impacts had a significant effect on the dependent variables (FD GSI, RD GSI). Post hoc Tukey tests were conducted to assess the differences between the helmets. We preset α at P < .05 for statistical significance.
RESULTS
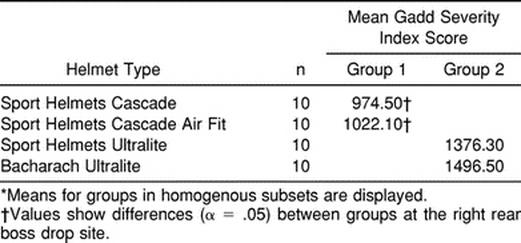
The FD GSI values (F3,36 = 9.680, P < .05) and the RD GSI values (F3,36 = 28.140, P < .05) were significantly different among helmet types (Table 1). The mean GSI statistics for FD and RD on each of the 4 helmet types are shown in Table 2. Three helmets scored above 1100.0 on the GSI. The BU helmet recorded the largest mean FD GSI score of 1222.8, which exceeds the NOCSAE recommendation for football helmets. The SU helmet design recorded the lowest mean GSI score of 857.0 for the FD trials. Contemporary helmets recorded the lowest mean GSI values of 974.5 for SC and 1022.0 for SA helmets in RD trials. Traditional helmets recorded the highest mean GSI values of 1376.3 by SU and 1496.5 by BU helmets in the RD trials.
Table 1. Helmet Impact Responses Exceeding Certain Gadd Severity Index Values*

Table 2. Gadd Severity Index Values for Front Drop and Right Rear Boss Drop Sites*
After repetitive impacts, helmets generally exhibited concomitant increases in GSI scores (Table 3, Figures 7 and 8). Helmet GSI scores plotted by impact trial for each treatment site are provided in Figures 9 and 10. Significant differences were revealed in GSI scores between traditional and contemporary designs for both FD and RD treatments (Tukey post hoc, P < .05) (Tables 4 and 5).
Table 3. Increases in Gadd Severity Index Scores (GSI), Trials 1 Through 10*
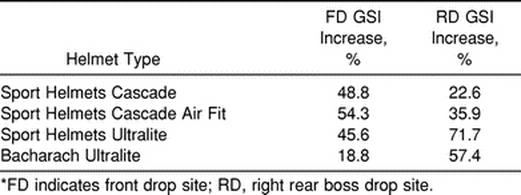
Figure 7.

Standard deviations of front drop site mean Gadd Severity Index (GSI) values. SC indicates Sport Helmets Cascade; SA, Cascade Air Fit; SU, Sport Helmets Ultralite; and BU, Bacharach Ultralite.
Figure 8.

Standard deviations of right rear boss drop site mean Gadd Severity Index (GSI) values. SC indicates Sport Helmets Cascade; SA, Cascade Air Fit; SU, Sport Helmets Ultralite; and BU, Bacharach Ultralite.
Figure 9.

Front drop site Gadd Severity Index values by trial for each helmet design. SC indicates Sport Helmets Cascade; SA, Sport Helmets Cascade Air Fit; SU, Sport Helmets Ultralite; BU, Bacharach Ultralite.
Figure 10.

Right rear boss drop site Gadd Severity Index values by trial for each helmet design. SC indicates Sport Helmets Cascade; SA, Sport Helmets Cascade Air Fit; SU, Sport Helmets Ultralite; BU, Bacharach Ultralite.
Table 4. Tukey Post Hoc Test Results for Front Drop Site*
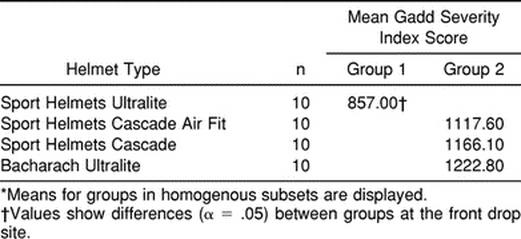
Table 5. Tukey Post Hoc Test for Right Rear Boss Drop Site*
DISCUSSION
Men's lacrosse has the potential for serious and catastrophic acute injuries to the head and neck.3,5,8,10 The 1999 National Collegiate Athletic Association Injury Surveillance Report on men's lacrosse concluded that player contact caused more than half of the reported game injuries. Thirteen percent of total game injuries involved the head; most were concussions.11
Our study is the first to quantify the impact response of 4 different lacrosse helmets by using a guided free-fall drop test. The NOCSAE, which was formed in response to the increasing number of football fatalities during the late 1960s and early 1970s, has examined and devised standards for lacrosse helmets.29 We chose the FD to mimic a head-on collision and the RD to simulate forces from a blind-sided impact. We attempted to provide a true representation of the potential contact forces placed on a lacrosse helmet during actual competition.
Our data demonstrate apparent differences among helmet designs based on each helmet's decreasing ability to dissipate impact energy throughout repeated contact. The SU traditional design was more efficient at attenuating impact forces at the FD location than all other helmet designs. At the RD, the SU and BU helmets exhibited the highest mean GSI values in the study, demonstrating significant differences between the traditional and contemporary helmet designs at the RD.
These findings suggest 2 important points of interest. First, the SC and SA contemporary helmet designs may attenuate RD impact forces more effectively than the traditional SU and BU helmets. Second, the SU traditional helmet design is more effective at attenuating FD impact forces when compared with the other helmet designs in our study. These observations support the effect of helmet design on energy attenuation.
Repeated impacts at subconcussive intensities could have injurious, cumulative effects, both histopathologically and cognitively.35,36 We know of no such studies of men's lacrosse players. However, neuropsychological studies of soccer players have revealed reduced cognitive functioning after repeated heading of the ball.37 Neuropsychological studies involving the cumulative effects of repeated head impacts in football have shown significant but perhaps reversible neuropsychological impairment after a single minor head injury, but potential long-term consequences remain to be explained.38–40
Naunheim et al2 made an effort to quantify the frequency and level of head acceleration experienced by high school athletes. Their purpose was to provide a basis for the correlation of longitudinal neurologic evaluations with the number and severity of subconcussive-level exposures. A triaxial accelerometer, which was mounted inside the helmets of secondary school ice hockey and football players, recorded an average of 24.7 and 40.5 impacts, respectively, per player-hour. The average peak acceleration was 29.2 ± 1.1g for football-related impacts and 35.0 ± 1.7g for ice hockey. We found average peak acceleration measures for contemporary helmets of 47.34 ± 3.0g by the SC and 47.93 ± 3.0g by the SA. We also noted average peak measures for traditional helmets of 45.62 ± 3.0g by the SU and 49.12 ± 2.9g by the BU. Threshold criterion values of 200g or 1500 on the GSI for a serious traumatic impact have been shown.2,22 All observed peak acceleration values in our study fall below the 200g predicted for a traumatic brain injury. However, reasonable questions exist regarding the cumulative effects of frequent subconcussive impacts and their potential to cause neurologic dysfunction over time.2 The precise low-level GSI magnitude and frequency of impacts resulting in cumulative neurologic effects are unknown.
We analyzed percentage increases in GSI values from trials 1 through 10 in both the FD and RD treatments to determine which helmet design influences the capacity to attenuate repetitive impact energy. Similar experiments have been performed on football helmets using GSI criterion to compare factors of internal padding and outer shell design. Bishop et al22 tested 81 football helmets with various internal padding designs on a right rear boss impact site. Suspension helmets were inferior to padded-suspension and padded helmets. Vetter and Vanderby41 examined the influence of materials and structure on football helmet performance. They found that the helmet shell minimally influences energy absorption, regardless of material and thickness.
The superior portion padding in our lacrosse helmets manufactured by Sport Helmets USA is composed of extended polypropylene. According to the manufacturer, this material is capable of withstanding repetitive impacts without devaluing its quality of protection. Our data expose a decreased ability in all lacrosse helmets tested to attenuate impact force. Helmets exhibiting the largest increase in GSI values from drops 1 through 10 were the SA by 54.3% and the SU by 71.7% at the FD and RD, respectively. Hodgson20 examined the effects of helmet age and wear on attenuation. He tested 849 used football helmets and found that 84% produced GSI values between 1450 and 2900. Increasing GSI scores after repetitive impacts suggest the need for research on the effects of helmet age and use on a lacrosse helmet's capacity to dissipate impact force. The noted increases in GSI scores during our study indicate several important points. First, a discrepancy exists between GSI standards for lacrosse and football. The standard GSI limit for a safe football helmet is considered by the NOCSAE to be 1200.23–27,29 The NOCSAE standard for a safe lacrosse helmet is a GSI score of less than 1500. No revisions have been implemented in the lacrosse standard since 1990.19 Second, the RD has been shown to have lower GSI values in tests because of eccentric loading of the head form.22,28 Finally, Bishop et al22 reported that the use of a GSI standard of 1200 as opposed to a standard of 1500 seemed prudent because GSI data were developed for frontal impacts in adults. Therefore, GSI results may not be an accurate predictor of injury at other locations on the head. Additionally, this information raises concerns that a nonadult population may possess a lower GSI threshold to injury.
Several areas regarding helmet performance need further research. These include the effects of helmet fit, environmental conditions, shell composition, helmet shape, face mask design, and types of padding on helmet impact response. We examined helmets during 20 successive drops and observed a significant decrease in each helmet's capacity to dissipate impact force. A male lacrosse athlete may experience 20 collisions in a single practice. Repeated exposures to subconcussive levels of impact could be injurious. However, there are currently no quantitative data regarding the precise acceleration magnitude and impact frequency at which an athlete should be concerned about cumulative neurologic deficits.2 Thus, we can pose serious questions as to the capacity of a helmet to adequately protect an athlete throughout an entire season or career of impacts. The NOCSAE standards mandate football helmet reconditioning at the football season's conclusion by approved reconditioners. The NOCSAE also requires impact testing of a certain percentage of these helmets.19–29 Currently, the NOCSAE and the manufacturers of lacrosse helmets only recommend recertification on an annual basis or discarding the helmet after 3 years of use.29 We know of no epidemiologic data reporting percentages of lacrosse athletes adhering to the NOCSAE guidelines. Given the apparent decrease in protection of all helmets used in our study, it is possible that athletes who wear the same helmet for their entire lacrosse career without reconditioning and recertification are not ensured a proper standard of protection. Therefore, further longitudinal studies are needed regarding the prophylactic benefits of helmets on the incidence of acute and cumulative brain injuries in men's lacrosse players.
CONCLUSIONS
We examined 4 differently designed lacrosse helmets and compared them based on their capacity to attenuate impact energy transmitted to the head. We found significant differences between helmet designs at the FD and RD. All helmets used in the study exhibited sharp increases in GSI values with repetitive impacts. Contemporary helmet designs performed better in RD tests than traditional helmets. We believe that future research is needed to assist in the development of new helmet testing standards with increased validity and reliability. These studies should include impact force and frequency measurements during game situations, the effects of repetitive impacts on a larger sample, and longitudinal studies involving helmet wear and reconditioning practices on concussion rates in men's lacrosse athletes.
Acknowledgments
ACKNOWLEDGMENTS
We express our appreciation to Trenton E. Gould, MS, ATC, CSCS, for his contributions in performing the statistical analyses and critical revision; Michael G. Miller, EdD, ATC, CSCS, Western Michigan University, and David C. Berry, PhD, ATC, Salem State College, for their contributions to acquisition of data, analysis and interpretation of the data, and critical revision; Rodney Zide, Zides Sporting Goods (Marietta, OH), for allowing us the use of the helmet testing equipment; Sport Helmets USA, Liverpool, NY, for donating helmets and providing photos; and Bacharach Lacrosse Company for donating helmets. We also thank Scott Gardner, MS, ATC, for his time and contribution in providing photographs.
REFERENCES
- Sosin D M, Sniezek J E, Thurman D J. Incidence of mild and moderate brain injury in the United States, 1991. Brain Inj. 1996;10:47–54. doi: 10.1080/026990596124719. [DOI] [PubMed] [Google Scholar]
- Naunheim R S, Standeven J, Richter C, Lewis L M. Comparison of impact data in hockey, football, and soccer. J Trauma. 2000;48:938–941. doi: 10.1097/00005373-200005000-00020. [DOI] [PubMed] [Google Scholar]
- Matthews L S, Michael R H. Lacrosse. In: Fu F H, Stone D A, editors. Sports Injuries: Mechanisms, Prevention and Treatment. Williams & Wilkins; Baltimore, MD: 1994. pp. 469–479. [Google Scholar]
- Kulund D N, Schildwachter T L, McCue F C, III, Gieck J H. Lacrosse injuries. Physician Sportsmed. 1979;7(5):83–90. doi: 10.1080/00913847.1979.11710862. [DOI] [PubMed] [Google Scholar]
- Casazza B A, Rossner K. Baseball/lacrosse injuries. Phys Med Rehabil Clin N Am. 1999;10:141–157. [PubMed] [Google Scholar]
- Vennum T. American Indian Lacrosse: Little Brothers of War. Smithsonian Institution Press; Washington, DC: 1994. pp. 69–72. [Google Scholar]
- Rimel R W, Nelson W E, Persing J A, Jane J A. Epidural hematoma in lacrosse: a case report. Physician Sportsmed. 1983;11(3):140–144. doi: 10.1080/00913847.1983.11708487. [DOI] [PubMed] [Google Scholar]
- Nelson W E, DePalma B, Gieck J H, McCue F C, III, Kulund D N. Intercollegiate lacrosse injuries. Physician Sportsmed. 1981;9(10):86–92. doi: 10.1080/00913847.1981.11711187. [DOI] [PubMed] [Google Scholar]
- Ginsburg B. You think hockey is rough? Take a look at box lacrosse. Physician Sportsmed. 1975;3(9):100–101. doi: 10.1080/00913847.1975.11948265. [DOI] [PubMed] [Google Scholar]
- Mueller F O, Blyth C S. A survey of 1981 college lacrosse injuries. Physician Sportsmed. 1982;10(9):87–93. doi: 10.1080/00913847.1982.11947322. [DOI] [PubMed] [Google Scholar]
- National Collegiate Athletic Association The NCAA News & Features: Injury Surveillance System. Available at: http://www.ncaa.org/news/1990927/active/3620n07.html. Accessed December 27, 2000.
- Salcido R, Costich J F. Recurrent traumatic brain injury. Brain Inj. 1992;6:293–298. doi: 10.3109/02699059209029671. [DOI] [PubMed] [Google Scholar]
- Annegers J F, Grabow J D, Kurland L T, Laws E R., Jr. The incidence, causes, and secular trends of head trauma in Olmstead County, Minnesota, 1935–1974. Neurology. 1980;30:912–919. doi: 10.1212/wnl.30.9.912. [DOI] [PubMed] [Google Scholar]
- Jordan B D, Zimmerman R D. Computed tomography and magnetic resonance imaging comparisons in boxers. JAMA. 1990;263:1670–1674. [PubMed] [Google Scholar]
- Gronwall D, Wrightson P. Cumulative effect of concussion. Lancet. 1975;2:995–997. doi: 10.1016/s0140-6736(75)90288-3. [DOI] [PubMed] [Google Scholar]
- Gadd C W. Proceedings of the Tenth Stapp Car Crash Conference 1966; New York, NY. Vol. 29. Society of Automotive Engineers Inc; New York, NY: 1966. Use of weighted-impulse criterion for estimating injury hazard; pp. 249–254. [Google Scholar]
- Gadd C W. Report to SAE Performance Criteria Subcommittee. Vehicle Research Department, General Motors Research Laboratories, General Motors Technical Center; Warren, MI: 1972. [Google Scholar]
- Versace J. Proceedings of the 15th Stapp Car Crash Conference November 1971; New York, NY. Society of Automotive Engineers Inc; New York, NY: 1971. A review of the Severity Index. [Google Scholar]
- Standard Method of Impact Test and Performance Requirements for Lacrosse Helmets and Faceguards. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1990. [Google Scholar]
- Hodgson V R. Impact standards for protective equipment. In: Torg J, editor. Athletic Injuries to the Head, Neck, and Face. 2nd ed. Mosby; Baltimore, MD: 1991. pp. 28–41. [Google Scholar]
- Calvano N J, Berger R E. Effects of selected test variables on the evaluation of football helmet performance. Med Sci Sports. 1979;11:293–301. [PubMed] [Google Scholar]
- Bishop P J, Norman R W, Kozey J W. An evaluation of football helmets under impact conditions. Am J Sports Med. 1984;12:233–236. doi: 10.1177/036354658401200313. [DOI] [PubMed] [Google Scholar]
- In: Football Helmet Standards for Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Standard drop test method and equipment used in evaluating the performance characteristics of protective head gear; pp. 1–19. [Google Scholar]
- In: Football Helmet Standards for Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Standard performance specification for recertified football helmets; pp. 1–2. [Google Scholar]
- In: Football Helmet Standards for Newly Manufactured and Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1998. Standard drop test method and equipment used in evaluating the performance characteristics of protective headgear; pp. 1–18. [Google Scholar]
- In: Football Helmet Standards for Newly Manufactured and Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Standard performance specification for newly manufactured football helmets; pp. 3–6. [Google Scholar]
- In: Football Helmet Standards for Newly Manufactured and Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Standard performance specification for recertified football helmets; pp. 1–2. [Google Scholar]
- Crisco J J, Hendee S P, Greenwald R M. The influence of baseball modulus and mass on head and chest impacts: a theoretical study. Med Sci Sports Exerc. 1997;29:26–36. doi: 10.1097/00005768-199701000-00005. [DOI] [PubMed] [Google Scholar]
- NOCSAE Manual. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1997. [Google Scholar]
- In: Football Helmet Standards for Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Equipment calibration procedures; pp. 1–6. [Google Scholar]
- In: Football Helmet Standards for Newly Manufactured and Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Equipment calibration procedures; pp. 1–9. [Google Scholar]
- In: Football Helmet Standards for Newly Manufactured And Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Laboratory procedural guide for certifying newly manufactured football helmets; pp. 2–4. [Google Scholar]
- In: Football Helmet Standards for Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Laboratory procedural guide for recertifying football helmets; pp. 1–3. [Google Scholar]
- In: Football Helmet Standards for Recertified Helmets. NOCSAE. National Operating Committee on Standards for Athletic Equipment; Overland Park, KS: 1996. Trouble shooting guide for test equipment and impact testing; pp. 1–5. [Google Scholar]
- Gennarelli T A, Thibault L E, Ommaya A K. Pathophysiologic responses to rotational and translational accelerations of the head. In: Backaitis S H, editor. Biomechanics of Impact Injury and Injury Tolerances of the Head-Neck Complex. Society of Automotive Engineers Inc; Warrendale, PA: 1993. pp. 411–423. [Google Scholar]
- Bigler E, Snyder J. Neuropsychological outcome and quantitative neuroimaging in mild injury. Arch Clin Neuropsychol. 1995;10:159–174. [PubMed] [Google Scholar]
- Tysvaer A T, Lochen E A. Soccer injuries to the brain: a neuropsychologic study of former soccer players. Am J Sports Med. 1991;19:56–60. doi: 10.1177/036354659101900109. [DOI] [PubMed] [Google Scholar]
- Wilberger J E. Minor head injuries in American football: prevention of long term sequelae. Sports Med. 1993;15:338–343. doi: 10.2165/00007256-199315050-00005. [DOI] [PubMed] [Google Scholar]
- Willberger J E, Haag B, Maroon J C. New Orleans, LA: Cumulative effects of football related minor head injury. Paper presented at: American Association of Neurological Surgeons Meeting. April 21-25 1991. [Google Scholar]
- Alves W M, Rimel R W, Jane J. Dallas, TX: Recovery from football induced minor head injury. Paper presented at: American Association of Neurological Surgeons Meeting. October 7-9 1987. [Google Scholar]
- Vetter L, Vanderby R. Influence of materials and structure on performance of a football helmet. Polymer Eng Sci. 1987;27:1113–1120. [Google Scholar]