

Abstract
Objective: To determine enforcement patterns and athlete compliance with the National Collegiate Athletic Association (NCAA) rule requiring the wearing of mouthguards in men's collegiate ice hockey games during a single competitive season.
Design and Setting: We developed a questionnaire and sent it to certified athletic trainers (ATCs) directly responsible for men's varsity collegiate ice hockey at 127 NCAA-affiliated institutions. Then χ2 analyses were conducted to determine whether significant differences existed in the pattern of responses by division of play (Division I, II, or III or independent).
Subjects: A total of 104 ATCs responded. We obtained data from 94 questionnaires with complete answers to primary questions addressing program enforcement of the rule and mouthguard use.
Measurements: Our questionnaire asked about types of mouthguards used, attitudes of the sports medicine and coaching staffs regarding the role of mouthguards in prevention of injury, enforcement of mouthguard use, and actual numbers of athletes wearing mouthguards in competition. Respondents also provided an estimate of the number of penalties assessed against their team for mouthguard violations during the previous season.
Results: Most ATCs (93%) reported that they believed mouthguards play a role in injury prevention. Respondents indicated someone on the coaching or sports medicine staff enforced the rule at 74% of the institutions, with a trend toward greater enforcement at the Division II and III levels. Overall, ATCs reported 63% of athletes consistently wore mouthguards in competition, with significantly higher compliance at the Division II and III levels. A total of 19 penalties were reportedly assessed for violation of the mouthguard rule the previous season.
Conclusions: Our data suggest that the use of mouthguards in competition is not consistently enforced by ATCs, coaches, or game officials and that mouthguards are not routinely worn by athletes. These results raise legitimate concerns for all physicians, athletic trainers, coaches, and governing bodies involved with men's collegiate ice hockey.
Keywords: concussion, mild brain injury, injury prevention, protective equipment
Ice hockey is one of the fastest and most violent team sports in the world. In light of this, the number of injuries that result from collisions with the playing surface, boards, opponents, and teammates is not surprising. Athletes participating today are on average 2 in (5.08 cm) taller and 14 lb (6.35 kg) heavier than they were 25 years ago.1 Direct analysis of the prevalence of head injuries in ice hockey is difficult because of nonuniform patterns of injury reporting and disparate injury definitions. In addition, there are differences in the age, skill levels of athletes, and types of equipment being used when an injury occurs.2,3 The National Collegiate Athletic Association (NCAA) has developed the Injury Surveillance System4 in an effort to provide current and reliable data on collegiate injury trends. These data remain ambiguous, because there is no definitive mode of determining whether required safety standards are being upheld.
Mouthguards were first used in athletics by boxers during the 1930s.5–7 They were designed to protect the mouth, teeth, and mandible and to cushion the effects of concussive blows to the jaw. A properly fitted mouthguard considerably reduces the amount of force being transmitted to the mandible after an impact.8,9 The Committee on Sports Equipment and Facilities of the American Society of Testing and Materials developed the current NCAA mouthguard regulation in 1980. The regulation requires mouthguards to be constructed of a resilient material that covers all of the teeth of one jaw, usually the upper.7 The 2 types of mouthguards most prevalent in athletics are the boil and bite (also known as mouth formed) and the custom-made mouthguard, which is constructed from a mold of the athlete's teeth.
The wearing of mouth protection in competition has been mandated by the NCAA for men's ice hockey since 1975 (National Collegiate Athletic Association, unpublished data, November 5, 1997). The rule today reads, “All players, including goalkeepers, are required to wear an internal mouthguard that covers all the remaining teeth of one jaw. The mouthguard shall not be altered from original manufacturer specifications, except with the prescription of a medical authority.”10 Compliance with mouthguard regulations at the youth and secondary school levels is excellent, but at the collegiate level it is more sporadic.11 Unfortunately, it has taken the recent increase in the incidence of mild and severe brain injuries in ice hockey at all levels to focus attention on preventive measures that may help to reduce this alarming trend.11 A former director of officiating for the Western Collegiate Hockey Association identified the concern among all involved in collegiate ice hockey over the growing number of head injuries. He observed an increase in safety standards for headgear during his tenure and collaboration among sports medicine professionals nationwide to enforce current mouthguard regulations (G. Shepherd, unpublished data, October 6, 1997). However, research is needed to determine the extent to which mouthguards are involved in the prevention of concussion.
Before any direct cause-effect relationship can be established between the severity of concussion in men's collegiate ice hockey and the use of mouthguards, we must determine how mouthguards are currently being used by collegiate athletes, particularly in competition. Therefore, our purpose was to determine patterns of enforcement and the extent to which NCAA Division I, II, and III and independent male varsity collegiate ice hockey players used mouthguards in games during a single competitive season.
METHODS
Subjects
Subjects involved in this study were certified athletic trainers (ATCs) directly responsible for the care of 1 of the 127 NCAA Division I, II, or III or independent men's varsity collegiate ice hockey programs. We selected this target population based on their daily involvement with the care of the athletes in question, increasing the likelihood that they would be able to respond accurately to the questionnaire. Institutional review board approval was obtained before the start of the data collection for this project.
Instrumentation and Measurement
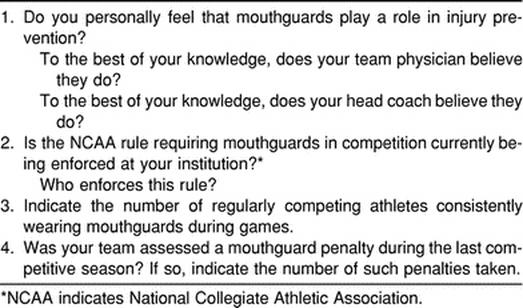
We developed a questionnaire specifically for this data collection process. It consisted of 7 basic questions requiring yes or no answers about mouthguard types, enforcement of use in both practice and games, and attitudes of both the sports medicine and coaching staffs regarding the efficacy of mouthguards in the prevention of head injury (Table 1). The ATCs were asked to estimate the number of athletes wearing mouthguards in games and the number of penalties incurred for noncompliance with the mouthguard rule during the previous season. As stated in the cover letter accompanying the questionnaire, completion and return of the questionnaire were accepted as informed agreement to participate in this study.
Table 1. Survey Questions Regarding Attitudes Toward Mouthguards, Enforcement Patterns, and Athlete Use During Collegiate Hockey Competition
A panel of 3 collegiate ATCs examined the questionnaire to ensure clarity of questions and determine logical or face validity. The questionnaire was pilot tested in December 1997 with ATCs at 8 local high schools sponsoring boys' ice hockey. This group was chosen because local collegiate hockey programs were part of the targeted study population. Minor revisions were made to the document, and it was finalized in December 1997.
Data Collection
Questionnaires were mailed in January 1998. Of 127 mailed, 104 were returned, for a response rate of 82%. Data for this study were obtained from 94 questionnaires containing complete answers to the questions of interest. This represented 74% of eligible programs.
Data Analysis
Responses to the first question regarding the role of mouthguards in injury prevention were tallied as a group. Responses to the other 3 questions were categorized by division of play (Division I, II, or III or independent). We conducted χ2 analyses to determine whether significant differences existed in the pattern of responses to questions by division of play. A significance level of .05 was chosen, and the Statistical Package for the Social Sciences (version 6.0, SPSS Inc, Chicago, IL) was used for analysis of the data. The findings are summarized in the Figure.
Fig. 1.

Summary of research findings on enforcement, compliance, and number of penalties assessed.
RESULTS
Key questions were identified as those best suited to answer our primary research objectives addressing mouthguard enforcement and use in NCAA men's varsity collegiate ice hockey. Each key question is listed, followed by the analysis of responses.
“Do you personally feel that mouthguards play an effective role in injury prevention?” Ninety-three percent responded affirmatively.
“To the best of your knowledge, does your team physician believe they do?” An almost equal percentage of team physicians, 92%, were reported to agree as well.
“To the best of your knowledge, does your head coach believe that they do?” More than three quarters (79%) of the responding ATCs agreed.
“Is the NCAA rule requiring mouthguards currently being enforced at your institution during games?” The ATCs were asked to respond to this question by indicating whether the coach or the sports medicine staff enforced wearing of mouthguards during competition. Responses were organized into a 4 × 2 table by division of play and enforcement (yes or no). The low number of independent and Division II institutions in the sample necessitated combining independent and Division I responses and Division II and Division III responses, creating a 2 × 2 table for analysis. Examination of the numbers in each category indicated that overall enforcement differed by grouped divisions, but the difference was not statistically significant (χ21 = 3.28, P = .07). Someone on the athletic training or coaching staff at 74% of responding institutions enforced the use of mouthguards during competition. Eighty-two percent of those at Division II and III schools reported enforcement, whereas 65% enforcement was reported for Division I and independent institutions (Table 2).
Table 2. Enforcement of Mouthguard Use During Competition*
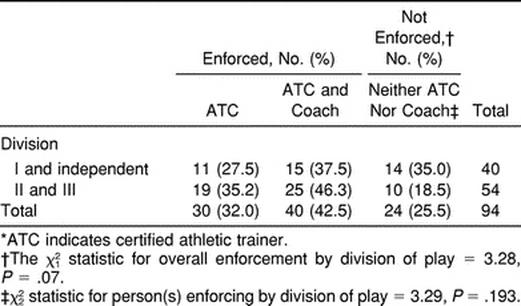
Responses were further categorized by whether the ATC alone, the coach alone, both the coach and ATC, or neither enforced the wearing of mouthguards during games. Only 3 ATCs reported that the coach alone enforced this rule. Consequently, these responses were combined with the ATC-alone classification for subsequent analysis. Low numbers in the independent and Division II classifications again necessitated combining of data as previously described. No significant difference in the pattern of enforcement by grouped divisions was noted (χ22 = 3.29, P = .193). Thirty-two percent of the ATCs reported that they alone or, in 3 cases, the coach alone enforced the rule. Approximately 26% responded that neither they nor the coach enforced the rule. The remainder, about 43%, reported that both the coach and ATC encouraged wearing of mouthguards by their athletes during games.
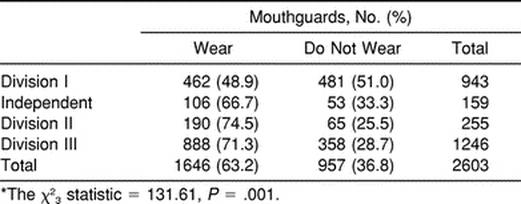
“Indicate the number of regularly competing athletes consistently wearing mouthguards during games.” Sufficient numbers of athletes were involved in each division to run the omnibus χ2 analysis with all 4 divisions of play. A significant difference was seen in the pattern of response by level of competition (χ23 = 131.61, P = .001) (Table 3). Follow-up χ2 tests were conducted to partition cells in sequence, comparing patterns of responses in individual cells with those in the combined other cells. The purpose of this 3-test sequence was to determine where actual differences existed among levels of play.12 Final results indicated a significant difference in the number of athletes wearing mouthguards during competition between the combined Division I and independent and Division II and Division III classifications (χ21 = 112.37, P = .001). Athletes in Divisions II and III were more likely to wear a mouthguard in competition than were their Division I and independent counterparts. Participating ATCs estimated that 72% of athletes in Divisions II and III wore mouthguards in games compared with 52% of Division I and independent athletes. Overall, 63% of athletes used mouthguards consistently in competition.
Table 3. Certified Athletic Trainers' Estimates of the Number of Athletes Wearing Mouthguards During Competition by Division of Play*
“Was your team assessed a mouthguard penalty during the last competitive season? If yes, indicate the number of such penalties taken.” The final question related to actual game official enforcement of the NCAA rule governing the use of mouthguards during the last competitive season. Responding ATCs reported that 19 penalties were assessed: 3 in Division I, 0 in independent, 2 in Division II, and 14 in Division III.
DISCUSSION
Because of recent restructuring, the divisional configuration of men's NCAA collegiate ice hockey has been altered since these data were collected. Division II has been dissolved, with teams redistributed primarily into Division III, whereas most independent programs have since merged into Division I. Therefore, our final statistical analysis groups, although driven by the pattern of responses and constraints of the analyses, are consistent with these current divisional alignments.
Our overall response rate was 82%, and data for this article were provided by 94 surveys with complete answers to the 4 key questions. Survey research presents the opportunity for nonresponse bias. Fewer surveys may have been returned from programs with less stringent enforcement or athlete compliance or both, which would make the actual percentages of athletes wearing mouthguards lower than reported herein.
One theory underlying the development of this study was that athletes in Division I men's ice hockey programs would be more prone to use mouthguards during competition due to the increased likelihood that these athletes would continue playing the sport professionally. This might make them more aware of the effects of a serious injury during collegiate play on their future careers. At least 152 Division I athletes are currently in the National Hockey League, whereas only 2 non–Division I collegiate athletes were identified as competing professionally by the same resource.13 However, this hypothesis was not supported by the data. At the combined Division I and independent levels, only 52% of the athletes were reported to wear mouthguards during competition, significantly different from 72% of Division II and III athletes reported to wear mouthguards in competition during the same season.
Athletes are often resistant to mouthguard use, complaining that mouthguards make it hard to speak clearly and that they cause breathing difficulty. Coaches may cite this as a reason for their lack of encouragement to wear them in practices and competition. Castaldi11 reported that almost all noncustom mouthguards fit poorly and tend to hinder normal respiration. Francis and Brasher14 investigated the physiologic effects of mouthguard use on respiratory ventilation and gas exchange during exercise. Their results supported Castaldi's comments by demonstrating that 3 types of noncustom mouthguards created a significant reduction in forced expiratory air volume and peak expiratory flow rates at heavy workloads. However, the authors also reported a significant decrease in oxygen consumption during high-intensity effort for all mouthguard types. They concluded that use of a mouthguard during high-intensity exercise may produce an effective pattern of respiration that may improve tissue oxygenation and lower metabolic cost. Clearly, more research needs to be conducted in this area, but these findings suggest that mouthguard use may not hinder high-intensity performance in objective laboratory tests. This information has not been well disseminated among coaches and athletes in sports requiring mouthguard use.
In addition, we presumed that Division I and independent coaches and ATCs would be more likely to encourage the wearing of mouthguards during competition. This presumption was also based on the potentially greater opportunity for their athletes to pursue a professional ice hockey career. Another issue is the fact that most Division I and independent men's ice hockey programs have a full-time ATC, in addition to the added support of another assistant coach. Our data indicated that, although there was no significant difference in the pattern of enforcement by division of play, a higher overall level of enforcement was reported at the combined Division II and III levels (82%) than at the combined Division I and independent levels (65%). In addition, both the ATC and coach were more likely to encourage mouthguard use at the Division II and III levels. This heightened level of enforcement corresponded with significantly higher athlete compliance at Division II and III levels than at Division I and independent levels.
One of the more alarming findings of this study is that one quarter of responding ATCs reported that neither they nor the coaching staff enforced mouthguard use during competition. This identified inaction clearly does not reflect the stated beliefs of most ATCs responding to this survey, who indicated that they, the team physician, and the coach feel mouthguards play a role in injury prevention. The health and safety of their athletes are compromised by the lack of enforcement of the use of mandated protective equipment. This is in direct opposition to the basic domains of athletic training. This breach of enforcement is also contrary to the NCAA regulation requiring mouthguard use, and it should be of concern to all individuals associated with collegiate ice hockey programs.
Compelling but controversial evidence has suggested that mouthguards may be instrumental in reducing the severity of concussion, in addition to their well-known capacity to reduce the incidence of orofacial injury.8,9,15–17 Properly fitted mouthguards alter condylar position at the temporomandibular joint, which appears to reduce force transmission from the mandible to the occiput.8,17 In theory, this would reduce the severity and potentially even the likelihood of concussion. A well-fitted mouthguard should be thick enough to adjust bite such that the mandibular condyles are not contacting the joint fossae. This realignment is critical to the aforementioned shock absorbance.9 Currently, researchers are examining this variable in the typical mouthguards being worn in high school athletics. The potentially devastating consequences of concussion should serve to increase concern among sports medicine and coaching staffs regarding inappropriate use or fit of all protective equipment, including mouthguards.
Another noteworthy finding of our study was the reported number of penalties assessed for violation of the NCAA mouthguard rule. The 2001 NCAA Ice Hockey Rules Book10 states in rule 3–4-c, “For initial violation, offending player shall be immediately replaced on the ice, and the referee shall warn the offending team that subsequent violations by any player of that team shall result in the player being assessed a misconduct.” This is a slight change from the wording of the rule in 1997, when a misconduct penalty was immediately assessed. No reason was cited by the NCAA for this change (T. Halpin, unpublished data, February 24, 2001). Our data indicate that about half of Division I and independent athletes and nearly one third of Division II and III athletes do not wear mouthguards during competition. However, only 19 penalties were reported to have been assessed during the entire previous season at all levels of play. The number of penalties is surprisingly low in light of the number of athletes reported to be in violation of the rule. Eighty-four percent of these penalties were assessed during Division II and III contests, in which our data show greater athlete compliance. These results suggest that the use of mouthguards may be positively influenced by the greater likelihood that a penalty will be assessed for noncompliance.
The purpose of our research was to determine attitudes toward the role of mouthguards in injury prevention, enforcement of their use, and the reported extent to which collegiate male ice hockey players use mouthguards in games during a single competitive season. Our findings indicated that most athletic trainers, team physicians, and coaches recognize the theoretic importance of mouthguard use in injury prevention. Three quarters of NCAA-affiliated men's collegiate ice hockey programs have at least one person on the coaching or athletic training staff encouraging wearing of mouthguards during competition. The other 25% do not report enforcing their use. Our data suggest that although there are no significant differences in the pattern of response to questions related to those issues by division of play, more stringent enforcement occurred at the Division II and III levels. The reported number of athletes actually wearing a mouthguard was, however, significantly different by division. Varsity male collegiate ice hockey players were more likely to wear mouthguards if they played in Divisions II or III as opposed to Division I or independent. These results suggest that higher levels of enforcement by ATCs and coaches may encourage greater compliance. Finally, few penalties were assessed for noncompliance with NCAA rule 3–4-c regarding mouthguard use during competition, especially considering the reported number of athletes playing without mouthguards. More penalties were assessed at the Division II and III levels, which may have had a positive impact on routine use.
Research is continuing into the causes and prevention of sport-related traumatic brain injury. Information obtained from this line of research may produce new and more compelling facts as to the role of mouthguards in the prevention of concussion. Over time, this information may make the appropriate use of mouthguards during practice and competition more common. In the meantime, these data suggest that consistent enforcement of mouthguard use by athletic training and coaching staffs influences compliance among male student-athletes in all divisions. In addition, a consistently applied penalty for noncompliance could have a tremendous impact on adherence and potentially reduce the incidence or severity of concussion or both. These issues raise concerns for further study of mouthguard compliance not only in men's ice hockey but also in any collision sport that presents an athlete with an increased risk of concussion and orofacial injury.
REFERENCES
- Farber M. Heads up! Sports Illustrated. 1996;85(27):100–105. [Google Scholar]
- Daly P J, Sim F H, Simonet W T. Ice hockey injuries: a review. Sports Med. 1990;10:122–131. doi: 10.2165/00007256-199010020-00005. [DOI] [PubMed] [Google Scholar]
- Putukian M, Echemendia R J. Managing successive minor head injuries: which tests guide return to play? Phys Sportsmed. 1996;24(11):25–38. doi: 10.3810/psm.1996.11.1283. [DOI] [PubMed] [Google Scholar]
- National Collegiate Athletic Association . Injury Surveillance System: 1997–97 Ice Hockey. National Collegiate Athletic Association; Indianapolis, IN: 1996–1997. [Google Scholar]
- Dick R. Injuries in collegiate ice hockey. In: Castaldi C R, Hoerner E F, Bishop P J, editors. Safety in Ice Hockey. American Society for Testing and Materials; Philadelphia, PA: 1993. pp. 21–30. [Google Scholar]
- Natt P. Custom made mouthguards for contact sports players. J R Soc Health. 1983;103:180. doi: 10.1177/146642408310300506. [DOI] [PubMed] [Google Scholar]
- Castaldi C R. History and present status: athletic mouthguards. Sportsmed Digest. 1988;10:1–2. [Google Scholar]
- Chapman P. Concussion in contact sports and importance of mouthguards in protection. Aust J Sci Med Sports. 1985;17:23–27. [Google Scholar]
- Kerr I L. Mouthguards for the prevention of injuries in contact sports. Sports Med. 1986;3:415–427. doi: 10.2165/00007256-198603060-00003. [DOI] [PubMed] [Google Scholar]
- National Collegiate Athletic Association . 2001 Men's and Women's Ice Hockey Rules and Interpretations. National Collegiate Athletic Association; Indianapolis, IN: 2001. [Google Scholar]
- Castaldi C R. The sports mouthguard: its use and misuse in ice hockey. In: Castaldi C R, Hoerner E F, Bishop P J, editors. Safety in Ice Hockey. American Society for Testing and Materials; Philadelphia, PA: 1993. pp. 164–173. [Google Scholar]
- Siegal S, Castellan N J., Jr. Nonparametric Statistics for the Behavioral Sciences. 2nd ed McGraw-Hill; New York, NY: 1988. [Google Scholar]
- The College Hockey Alumni page. USA Today com-Sports. Available at: http://www.usatoday.com/sports/hockey/stats/0001/origin.html. Accessed March 1, 2001.
- Francis K T, Brasher J. Physiological effects of wearing mouthguards. Br J Sports Med. 1991;25:227–231. doi: 10.1136/bjsm.25.4.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeYoung A K, Robinson E, Godwin W C. Comparing comfort and wearability: custom-made vs. self-adapted mouthguards. J Am Dent Assoc. 1994;125:1112–1118. doi: 10.14219/jada.archive.1994.0121. [DOI] [PubMed] [Google Scholar]
- Shaull K L. Fabrication of personalized custom mouthguards for athletes in contact sports. Trends Tech Contemp Dent Lab. 1985;2:10–15. [PubMed] [Google Scholar]
- Chapman P J. Players' attitudes to mouthguards and prevalence of orofacial injuries in the 1987 U.S. Rugby Football Team. Am J Sports Med. 1989;17:690–691. doi: 10.1177/036354658901700518. [DOI] [PubMed] [Google Scholar]