

Abstract
Objective: To determine the self-reported physical activities of certified athletic trainers (ATCs), both at work and at leisure.
Design and Setting: We used the Baecke Questionnaire of Habitual Physical Activity and also asked for demographic information, including employment setting, years of experience, education level, and position.
Subjects: The questionnaire was sent to 1200 randomly selected ATCs in the Mid-America Athletic Trainers' Association; the return rate was 53%.
Measurements: We used means, standard deviations, and ranges to describe the age, total fitness index, work, and leisure and sport indexes of men and women subjects. Independent t tests were used to compare the mean total activity index between men and women within this study and with previous studies. We examined differences in activity indexes by employment setting, position, and age with one-way analysis of variance and Fisher pairwise comparison tests. Two-way χ2 analysis was used to determine the relationship between activity level and employment setting and position. Statistical significance was set at P = .05 for all analyses.
Results: Certified athletic trainers who work in a clinical setting had the highest mean total activity score at 9.1 points. Clinic ATCs scored significantly higher than high school ATCs and college ATCs. When compared by position, there were no significant differences among the mean total activity indexes; however, the mean work index of program directors was significantly lower than all other positions and the mean work index of high school and clinic ATCs was significantly higher than all other employment settings.
Conclusions: Female ATCs scored significantly higher in total activity levels on the Baecke Questionnaire than their male counterparts. This is in contrast to the general population, investigated by other authors, in which men scored significantly higher than women on the same scale. Additionally, we compared the total activity levels by age, position, and employment setting. There was a significant difference by position only in the work index. The mean total index activity of the over-36-years-old group was significantly lower than all other age categories. There was no significant difference in mean total activity levels by employment setting.
Keywords: athletic trainer, energy expenditure, physical fitness, Baecke Questionnaire
Certified athletic trainers (ATCs) are the primary health care providers for the physically active. The advice that athletic trainers give to athletes may reflect their own health and fitness beliefs. The ATC should be a role model and proponent for physical activity for the athlete; however, there has been no research to date on ATCs' personal physical fitness or activity levels.
Physical activity may be broadly divided into 2 categories: physical activity in the work setting and leisure-time physical activity. Both categories have been measured among the general population with questionnaires that have been validated through direct measurement and task analysis.1–3 A certain level of physical fitness is necessary in many professions, especially those that require the professional to react in emergency situations, such as firefighters and police officers. Certified athletic trainers could be considered among those professionals needing some level of physical fitness to respond to emergencies. Other physical demands of these professions are lifting, standing for extended periods of time, and the stamina to work many hours. Physical fitness is an important factor in tolerance of long shifts in similar occupations.4 As ATCs are expected to work elongated and irregular days, physical fitness may be an important factor in work tolerance.
The other component of physical activity is leisure-time activity. Leisure-time activity has received the most emphasis of the physical activity components in recent years due to the increased awareness that leisure activity is highly associated with a healthy lifestyle.1–5 With the increasing reliance on technology that results in a general decrease in the physical demands of work, physical activity becomes an important component of a healthy lifestyle, especially for the person who does not have a physically demanding occupation. Higher levels of leisure-time physical activity correlate with decreases in body fat, resting heart rate, and blood pressure5 and decreased incidence of stroke6 and coronary heart disease.7
A variety of methods have been used to evaluate physical activity levels at work and in leisure. Some of these methods include task analysis, job classification, activity diaries, pedometers, accelerometers, and questionnaires.2,3,8,9
Use of all of these except for questionnaires may be time consuming or expensive. Physical activity questionnaires have been used in numerous studies and are closely related to the results obtained by the more time-intensive and expensive methods. A variety of physical activity questionnaires are available, many of which only identify leisure physical activity or work activity. The Baecke Questionnaire of Habitual Physical Activity includes measures for work activities, sport activities, and leisure activities.10
Several studies have used questionnaires to measure the physical activities of the general population; however, information about the physical activities of ATCs at work or during leisure is very limited. Therefore, our purpose was to determine the self-reported physical activities of ATCs.
METHODS
Instrument
We used the Baecke Questionnaire of Habitual Physical Activity. This questionnaire has been validated in several investigations6–9 and has been shown to be an easily administered and accurate instrument. When correlated with physical activity scores, validity coefficients ranged from r = .33 to r = .59 for men and women between the ages of 20 and 59 years. The questionnaire consists of 3 sections: work, sport (exercise), and nonsport leisure activity. Most of the questionnaire is scored on a 5-point Likert scale, with descriptors ranging from never to sometimes or very often. Three additional questions required reporting the type of sporting (exercise) activity and both the number of hours per week and the number of months per year in which the respondent participated in that activity. The original questionnaire was written for Europeans. Our only modification for this study was a slight change of wording so that the questionnaire would be more applicable to Americans in that “sport” was changed to “exercise activity.” In addition, questions including demographic information pertinent to ATCs, such as employment setting, years of experience, education level, and position, were added but did not affect the original questionnaire.
The scoring of the questionnaire included specific scoring criteria for each of the 3 sections: work, sport, and leisure indexes. Each section could receive a maximum score of 5 points, with a maximum of 15 points for the total activity index. Each index was rounded to the nearest tenth of a point.
Data Collection
Approval was received from the University of Nebraska Institutional Review Board before beginning this research. The questionnaire and a cover letter explaining the study were sent to 1200 randomly selected ATCs within District 5, the Mid-America Athletic Trainers' Association (MAATA) of the National Athletic Trainers' Association. Address labels were obtained from the National Athletic Trainers' Association for all athletic trainers living in District 5 (n = 1530). Systematic counting was used to select 1200 potential subjects. Subjects were asked to complete and return the questionnaire in a business reply envelope within 3 weeks. Completion of the questionnaire implied informed consent.
DATA ANALYSIS
We computed means, standard deviations, and ranges to describe the age, total fitness index, and work, leisure, and sport indexes of male and female subjects. An independent t test was used to compare the mean total activity index between men and women. One-way analysis of variance and Fisher pairwise comparison tests were calculated to examine differences in activity indexes by employment setting, position, and age. Frequency counts and 2-way χ2 analyses were used to examine the relationship between activity level and employment setting and activity level and position. Activity level categories were established with percentile ranks, with scores above P75 representing the highest level and those below P25, the lowest. Statistical significance was set at P = .05 for all analyses.
RESULTS
There were 636 respondents (372 men and 264 women) to the survey for a 53% return rate. Of the 636 respondents, 534 (84%) indicated that they were physically active outside of work, while 102 (16%) indicated that they were not. Table 1 shows a comparison using an independent t test between male and female ATCs. Women were significantly more physically active, as indicated by a higher total activity index.
Table 1. Physical Activity Indexes in Men and Women

One-way analysis of variance and Fisher pairwise comparison tests were used to examine differences in activity indexes by employment setting, position, and age as seen in Tables 2,3,4. Certified athletic trainers employed in the clinic were more physically active than high school ATCs and college ATCs (Table 2). The clinic ATCs were more active in sport activity than the high school ATCs, and they are more active at work than the college ATCs1 or those employed in other settings.
Table 2. Activity Indexes by Employment Setting
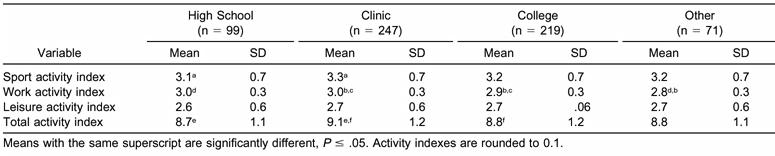
Table 3. Activity Indexes by Position
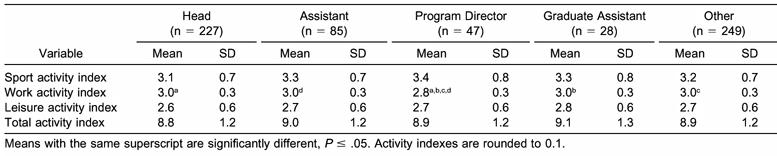
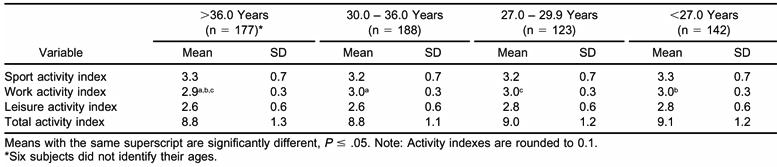
Table 4. Activity Indexes by Age
We found no significant differences among mean total activity indexes by position (Table 3); however, the mean work index of program directors was significantly lower by a mean 0.2 points than all other positions.
There were no significant differences among the mean total activity indexes by age group (Table 4); however, ATCs over the age of 36 years were significantly less active than all other age categories at work.
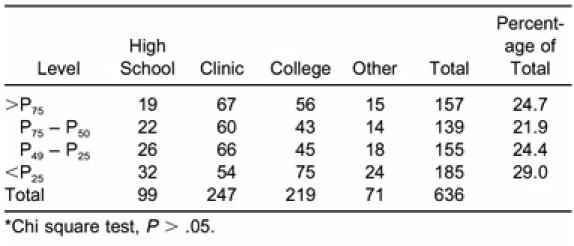
Frequency counts for activity levels by position appear in Table 5. Activity levels were determined by quartiles, with scores above P75 being the highest and those below P25, the lowest. A 2-way χ2 analysis showed there was no significant relationship between the type of position held and the number of subjects in each fitness quartile. This finding suggests that within each position, the fitness levels of ATCs were similarly distributed. Table 6 contains the frequency counts of activity levels by employment setting. A 2-way χ2 analysis revealed no significant relationship between employment setting and the number of subjects in each fitness quartile. This too, suggests comparable distribution within the employment settings.
Table 5. Frequency Counts of Activity Levels by Position*

Table 6. Frequency Counts of Activity Levels by Employment Setting*
DISCUSSION
We surveyed ATCs in the Midwest and found that 16% of the respondents were not physically active. Previous researchers have reported that 9% to 27% of the general population was not physically active.11–13
The difference in the total activity index between men and women is in contrast to data from the general population reported in previous studies. Schramm et al14 studied the relationship between physical activity and flexibility in 64 women. Using the same instrument we used, Schramm et al reported a mean total activity index of 8.1. This was significantly different (t = 4.91, P < .05) from the mean total activity index of female ATCs in our study.
Differences were also noted in the mean total activity index between ATCs in our study and a previous study performed by Richardson et al.2 In the latter study, the Atherosclerosis Risk in Communities/Baecke Questionnaire was administered to 50 women with a reported mean total activity index of 8.5. This is a difference in the total activity index of 0.5 when compared with female ATCs. No differences in the mean total activity index among men were noted among the Schramm et al14 and Richardson et al2 studies and our study. Baecke et al10 and Misigoj-Durakovic et al15 reported that the women's leisure index was significantly higher than that of their male subjects, while Jacobs et al3 found no difference. Previous investigators2,3 have reported men scoring significantly higher on the sport indexes than women, while in our study there was no significant difference. We speculate this may be due, in part, to the women who choose to go into the profession of athletic training.
Age was also a factor in the work activity index differences. The over-36-years-old category had a significantly lower work activity index than the other age categories. A possible explanation may be that older ATCs were in a position for a greater length of time and had advanced to more supervisory or administrative positions. With increasing numbers of administrative tasks, the older ATC may no longer perform as many of the more physically taxing athletic training tasks on a daily basis.
Employment Setting and Position
The mean total activity index between ATCs working in the clinic setting (9.1) was significantly different than their counterparts in the high school (8.7) and college settings (8.8). Significant differences were also found between clinic and high school ATCs in the sport activity index (3.2 and 3.1, respectively). These data suggest that clinic ATCs reported more activity in sport than high school ATCs. This may be due to clinic ATCs having more control over their schedules to allow participation in a regular exercise routine.
High school and clinic ATCs had the highest work activity index (3.0). This was significantly higher than ATCs working in the college or other setting. These data suggest that high school and clinic ATCs perceive their jobs as being more physically demanding than ATCs in other settings. As many clinic ATCs are also contracted to high schools, it makes sense that these 2 work indexes would be similar. The difference between high school and clinic ATCs and other ATCs may be due in part to the high school or clinic ATC often being the only person involved in the day-to-day care of all of the sports at the high school. The college ATCs often have more students or assistants to help with the physical aspect of practices and game preparations.
When examined by position (head athletic trainer, assistant athletic trainer, program director, graduate assistant, or other), the program directors had a significantly lower work index than all other positions. This is most likely because most program director positions involve more sedentary skills and less activity than a typical athletic training position. There was, however, no significant difference in the total fitness index among positions.
The concept that physical activity and physical fitness are contributors to good health has substantial documentation. Work-related and recreational physical activity are associated with decreased risks for coronary artery disease5,16 and stroke.4 Further, Cox and Montgomery17 found that a high level of fitness may be associated with decreased absenteeism and increased job performance.
Certified athletic trainers are proponents of physical fitness for the athlete. One would expect ATCs to have knowledge of the benefits of personal physical fitness and to lead by example. However, for males in this study, the total activity index was no higher than that for the general population, indicating that even though ATCs understand physical fitness, their compliance was not any better than the general population. Boritz18 reported that 93% (n = 126) of physicians surveyed were regular exercisers, while only 84% of the respondents in our study indicated that they were physically active outside of work.
The female ATCs in this study, however, scored higher in total activity than the women in the general population surveyed in previous studies. This may be due to the personal and physical characteristics of the women who pursue athletic training as a profession or to a concerted effort on the part of the female ATCs in this study to participate in physical activities.
Most of the significant differences we found were relatively small in magnitude. This fact should be kept in mind when interpreting the results of this research.
Both the National Athletic Trainers' Association Board of Certification Role Delineation Study19 and the National Athletic Trainers' Association Educational Competencies20 include knowledge of the benefits of physical activity and the design of regular exercise programs as entry-level skills that all ATCs should possess. Why is it, then, that ATCs do not score any better than the regular population on total activity levels?
Numerous reasons not measured in this study may account for the less-than-desirable physical activity scores of the ATCs in this study. Certified athletic trainers tend to work extended hours and are often not in control of their time due to the schedule of games and practices. It may be difficult for many ATCs to find time to exercise routinely. Added responsibilities, such as team travel and home, family, and teaching responsibilities may make regular exercise habits difficult to maintain.
CONCLUSIONS
Our purpose was to determine the self-reported physical activities of ATCs, both at work and at leisure and sport. We compared the total activity levels by sex, employment setting, position, and age. There was a mean difference by position only in the work index. The mean total index activity of the over-36-years-old group was significantly lower than all other age categories. Athletic trainers in the clinic setting had a mean total activity index significantly greater than either the high school or college ATC.
We also found that female ATCs scored significantly higher in total activity levels on the Baecke Questionnaire than their male counterparts. This is in contrast to the findings in the general population, investigated by other authors, which indicated that men scored significantly higher than women on the same scale.
The results of this study suggest several areas for further investigation. Because this study was limited to the Midwest, it would be advantageous to replicate this study nationwide to determine whether there is a difference in the activity level of ATCs. Second, more information needs to be obtained on the actual energy expenditure for ATCs within various settings. Third, further investigation into the perceived barriers to regular exercise for the ATC is needed. Finally, studies including other health habits of ATCs and other health care professionals are beneficial.
Acknowledgments
ACKNOWLEDGMENTS
This study was made possible through a grant from the Mid-America Athletic Trainers' Association. Special acknowledgement goes to Lisa Schniepp, ATC, and the athletic training students of the University of Nebraska at Omaha for their assistance in the study.
REFERENCES
- Lamb K L, Brodie D A. The assessment of physical activity by leisure-time physical activity questionnaires. Sports Med. 1990;10:159–180. doi: 10.2165/00007256-199010030-00003. [DOI] [PubMed] [Google Scholar]
- Richardson M T, Ainsworth B E, Wu H C, Jacobs D R, Jr, Leon A S. Ability of the Atherosclerosis Risk in Communities (ARIC)/Baecke Questionnaire to assess leisure-time physical activity. Int J Epidemiol. 1995;24:685–693. doi: 10.1093/ije/24.4.685. [DOI] [PubMed] [Google Scholar]
- Jacobs D R, Jr, Ainsworth B E, Hartman T J, Leon A S. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc. 1993;25:81–91. doi: 10.1249/00005768-199301000-00012. [DOI] [PubMed] [Google Scholar]
- Harma M, Ilmarinen J, Knauth P. Physical fitness and other individual factors relating to the shiftwork tolerance of women. Chronobiol Int. 1998;5:417–424. doi: 10.3109/07420528809067787. [DOI] [PubMed] [Google Scholar]
- Klesges R C, Eck L H, Isbell T R, Fulliton W, Hanson C L. Physical activity, body composition, and blood pressure: a multimethod approach. Med Sci Sports Exerc. 1991;23:759–765. [PubMed] [Google Scholar]
- Evenson K R, Rosamond W D, Cai J, et al. Physical activity and ischemic stroke risk: the atherosclerosis risk in communities study. Stroke. 1999;30:1333–1339. doi: 10.1161/01.str.30.7.1333. [DOI] [PubMed] [Google Scholar]
- Lee I M, Paffenbarger R S. Preventing coronary heart disease: the role of physical activity. Physician Sportsmed. 2001;29(2):37–52. doi: 10.3810/psm.2001.02.366. [DOI] [PubMed] [Google Scholar]
- Pols M A, Peeters P HM, Bueno-De-Mesquita H B, et al. Validity and repeatability of a modified Baecke Questionnaire on physical activity. Int J Epidemiol. 1995;24:381–388. doi: 10.1093/ije/24.2.381. [DOI] [PubMed] [Google Scholar]
- Miller D J, Freedson P S, Kline G M. Comparison of activity levels using the Caltrac accelerometer and five questionnaires. Med Sci Sports Exerc. 1994;26:376–382. [PubMed] [Google Scholar]
- Baecke J A, Burema J, Frijters J E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr. 1982;36:936–942. doi: 10.1093/ajcn/36.5.936. [DOI] [PubMed] [Google Scholar]
- Salmon J, Owen N, Bauman A, Schmitz M K, Booth M. Leisure-time, occupational, and household physical activity among professional, skilled, and less-skilled workers and homemakers. Prev Med. 2000;30:191–199. doi: 10.1006/pmed.1999.0619. [DOI] [PubMed] [Google Scholar]
- Prevalence of leisure-time and occupational physical activity among employed adults—United States, 1990. MMWR Morb Mortal Wkly Rep. 2000;49:420–424. [PubMed] [Google Scholar]
- Sternfeld B, Ainsworth B E, Quesenberry C P. Physical activity patterns in a diverse population of women. Prev Med. 1999;28:313–323. doi: 10.1006/pmed.1998.0470. [DOI] [PubMed] [Google Scholar]
- Schramm T M, Latin R W, Berg K, Stuberg W. The relationship between physical activity and flexibility. Int Sports J. 2001;5:1–9. [Google Scholar]
- Misigoj-Durakovic M, Heimer S, Matkovic B R, Ruzic L l, Prskalo I. Physical activity of urban adult population: questionnaire study. Croat Med J. 2000;41:428–432. [PubMed] [Google Scholar]
- Powell K E, Thompson P D, Caspersen C J, Kendrick J S. Physical activity and the incidence of coronary heart disease. Annu Rev Public Health. 1987;8:253–287. doi: 10.1146/annurev.pu.08.050187.001345. [DOI] [PubMed] [Google Scholar]
- Cox C L, Montgomery A C. Fitness and absenteeism among hospital workers: clarifying the connection. AAOHN J. 1991;39:189–198. [PubMed] [Google Scholar]
- Boritz W M. Health behavior and experiences of physicians. West J Med. 1992;156:4–5. [PMC free article] [PubMed] [Google Scholar]
- National Athletic Trainers' Association Board of Certification . Role Delineation Study. 4th ed National Athletic Trainers' Association Board of Certification; Omaha, NE: 2001. [Google Scholar]
- National Athletic Trainers' Association . Athletic Training Clinical Proficiencies. National Athletic Trainers' Association; Dallas, TX: 1999. [Google Scholar]