

Abstract
Objective: To provide a comprehensive review of the literature regarding the role of external ankle support on joint kinematics, joint kinetics, sensorimotor function, and functional performance.
Data Sources: We searched MEDLINE and SPORT Discus databases from 1960–2001 for the key words ankle bracing, ankle support, ankle taping, and ankle prophylaxes. We also used personal libraries based on our own research to complement the existing literature.
Data Synthesis: The effects of external ankle support have been studied on a plethora of dependent measures. Here, we specifically discuss the role of external ankle support on joint kinematics, joint kinetics, sensorimotor function, and functional performance and present a general consensus regarding the overall effects of these prophylactic devices.
Conclusions/Recommendations: The effects of ankle support on joint kinematics during static joint assessment and on traditional functional-performance measures (ie, agility, sprint speed, vertical jump height) are well understood. However, the potential effects of ankle support on joint kinetics, joint kinematics during dynamic activity (eg, a cutting maneuver), and various sensorimotor measures are not well known. Future research investigating the role of external ankle bracing needs to focus on these areas.
Keywords: ankle bracing, joint mechanics, sensorimotor function, functional performance
Individuals who participate in athletic activities are particularly susceptible to ankle injuries1–5; of these injuries, approximately 86% are sprains.2 Acute ankle sprains occur during dynamic movement, particularly when rapidly changing directions. The lateral ligaments of the ankle-foot complex, which provide static support, are frequently torn, and the stability provided by the peroneal muscles is insufficient to limit forced inversion.4 It has been suggested that the peroneal muscle group plays a large role in dynamically stabilizing the lateral ankle-foot complex against an injurious inversion moment6–8; however, the extent to which this dynamic defense mechanism can protect the ankle-foot complex from injury is still unclear.
Because of the frequency of ankle injuries, a considerable amount of epidemiologic research has been conducted to examine the causes and effects of various methods used to prevent such injuries.9–12 The high incidence of trauma to the lower extremity, most notably the ankle-foot complex, has contributed to the proliferation of external ankle-stabilizing devices.13,14 Ankle taping, lace-up style braces, and semirigid orthoses are used in an effort to prevent ankle injuries and to stabilize patients who suffer from chronic ankle instability (CAI). Ankle bracing and taping reduce ankle injury9–12 and injury frequency rates,2,3,9–12,15,16 principally due to the mechanical support offered by these devices, although increased sensorimotor function offered by external ankle support may be a contributing factor.17,18
Many comparative studies have evaluated the efficacy of these different types of external ankle support on ankle-foot range of motion (ROM),19–41 functional performance,32,42–48 and various sensorimotor values1,8,17,18,49–64 in subjects with healthy and chronically unstable ankles. Thus, our purpose is to discuss and critically analyze the literature regarding the effects of external ankle support on joint kinematics, joint kinetics, sensorimotor function, and functional performance.
ANKLE PROPHYLAXES AND JOINT KINEMATICS
Most studies classifying the effects of external ankle support on joint kinematics have involved passive ROM evaluation using an isokinetic dynamometer19,22,26–28 or a goniometric device20,24,25,32–34,36,65–67 after some type of exercise. Little consideration has been given to using video32 or film analyses68 to assess the joint restriction provided by an ankle support after exercise consisting of a dynamic movement.
Gross et al26–28 compared the effects of adhesive tape and selected prophylactic ankle appliances on passive inversion and eversion before and after exercise. The tape condition, a softshell stabilizer, and a semirigid orthosis reduced inversion and eversion before exercise.26–28 After a 10-minute exercise session, tape still offered significant support compared with pre-exercise measures; however, the semirigid orthosis provided greater restriction.26 With a semirigid brace, eversion increased after exercise, although differences between a lace-up style brace and a semirigid stabilizer have not been found.26,27 With respect to inversion ROM, tape and semirigid orthoses28 have demonstrated greater restriction than a softshell or lace-up style brace,27 yet this result has not been supported by other work.21 Additionally, the DonJoy Ankle Ligament Protector (dj Orthopedics Inc, Vista, CA) provided greater inversion restraint, comfort, and perceived stability than the Aircast Sport Stirrup (Aircast Inc, Summit, NJ).28 It is interesting to note that eversion ROM increased after exercise during tape, lace-up, and semirigid conditions, while inversion ROM remained restricted.25,27,28 A plausible explanation may be that the braces are designed with more emphasis on restricting inversion, because that is the common mechanism of injury in ankle sprains; however, it does not appear to be supported or refuted by brace manufacturers.
A few authors24,25,34 have evaluated the effects of adhesive tape and selected ankle appliances on passive ROM after prolonged exercise sessions lasting more than 10 minutes. In as little as 10 minutes of exercise during a squash match, 2 ankle-support conditions (tape and lace-up style appliance) ineffectively supported the ankle.34 Additionally, after 1 hour of exercise, the adhesive tape lost its restrictive properties, resulting in greater plantar flexion and inversion and combined motions of plantar flexion with inversion and eversion. Similarly, after 20 minutes of exercise, inversion and eversion ROM increased with a lace-up style brace, while the Aircast Sport Stirrup maintained inversion support after 90 minutes of exercise.24 During the entire 90-minute practice session, the DonJoy Ankle Ligament Protector demonstrated no decrement in support. The authors24 concluded that the DonJoy Ankle Ligament Protector might be more beneficial than the Aircast Sport Stirrup for people who suffer from CAI. Adhesive tape substantially decreased its restrictive properties after 20 minutes of volleyball practice, while the braced ankles demonstrated diminished eversion restriction after 3 hours of practice, but in the latter group, inversion ROM restriction was maintained.25 Many of these researchers have concluded that either a lace-up brace or semirigid orthosis may be more effective than athletic tape in restricting subtalar joint ROM after exercise bouts lasting longer than 10 minutes.24,25,34
Although agreement exists concerning the effectiveness of different ankle prophylactic devices on passive subtalar-joint motion, little research has examined the role of external ankle devices in controlling such motion while running. In comparison with the abundance of published works regarding the role of external ankle supports on passive ankle-foot ROM after exercise, little information is available on the effects of different ankle prophylaxes on subtalar joint motion during dynamic activities such as walking, running, and lateral-cutting maneuvers. It may be evident that these various braces may behave differently when dynamically evaluated. Investigators in 2 ankle-support studies32,68 quantitatively measured rearfoot motion during running using motion-analysis technology. In an earlier study,68 the effectiveness of different types of ankle-tape support on pronation restriction while walking was measured. All ankle-strapping techniques were equally effective in maintaining consistent restriction for 10 minutes of continuous walking on a treadmill. Furthermore, all strapping techniques caused the foot to be excessively supinated before heel strike compared with the barefoot condition. More recently, inversion restraint provided by different ankle support devices was compared before and after walking and running.32 On subjects walking at 6.44 km/h (4 mph), the Aircast Sport Stirrup permitted the least amount of inversion (7.6° before exercise, 10.7° after exercise) compared with the Swede-O Universal lace-up (10° before exercise, 11.5° after exercise) brace (Swede-O Inc, North Branch, MN) and adhesive tape (10.7° before exercise, 14.8° after exercise). With subjects running at 14.48 km/h (9 m/h), the Aircast Sport Stirrup brace and Swede-O-Universal lace-up brace demonstrated no difference in average maximum inversion before and after exercise. They concluded that athletic tape is ineffective in restricting inversion under a dynamic load, while the Sport Stirrup and lace-up brace were similar in limiting inversion during walking and running.
In an attempt to statistically synthesize the related literature in this area,39 we used a meta-analysis approach to evaluate ankle-support effects on ankle and foot ROM before and after exercise. We evaluated 253 effects from 19 studies (that met all of the inclusion criteria) published between 1966 and 1997. Standardized effect sizes were calculated to establish the overall restrictive effect of each treatment condition (tape, lace-up braces, and semirigid braces) compared with the control condition within each study. The average ROM restriction in degrees compared with the control condition was calculated from the standardized effect sizes (Table 1). Because we applied a quantitative statistical analysis to published research in this area, the following conclusions can be considered a consensus regarding the effects of external ankle support on ankle-foot ROM:
Table 1. Standardized Effect Sizes and Average Range-of-Motion Restriction Using Tape, Lace-Up, and Semirigid Ankle Supports during Pre- and Postexercise Movements*
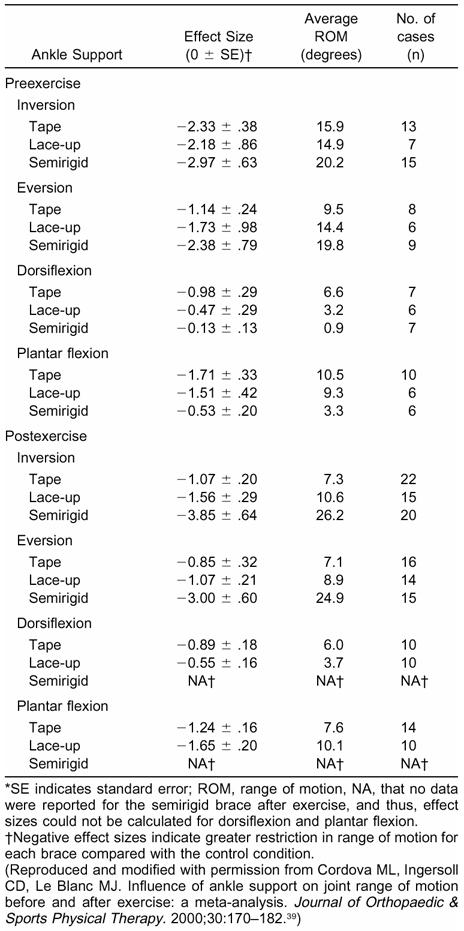
Before exercise, semirigid braces restricted inversion ROM 21.3% more than tape and 26.2% more than lace-up braces.
After exercise, semirigid braces restricted inversion ROM 72.1% more than tape and 59.5% more than lace-up braces.
No significant difference existed in inversion ROM restriction between the tape and lace-up brace conditions before (15.9° and 14.9°, respectively) or after exercise (7.3° and 10.6°, respectively).
Semirigid braces provided greater eversion ROM restraint compared with the tape and lace-up brace conditions before (19.8° semirigid, 9.5° tape, 14.4° lace-up) and after exercise (24.9° semirigid, 7.1° tape, 8.9° lace-up).
Lace-up braces provided greater overall eversion ROM restriction (9.8°) than tape (7.2°).
Dorsiflexion ROM was restricted 38.3% more with taping than with a lace-up brace.
No significant difference existed between tape (9.1°) and lace-up style braces (9.7°) on overall plantar flexion ROM restriction.
Historically, the assessment of talocrural-talocalcaneal joint displacement has been the primary research focus in understanding the mechanical effects of external ankle support. Surprisingly, little emphasis has been placed on studying the effects of ankle support on other kinematic variables such as angular velocity and angular acceleration. Quantifying talocrural and talocalcaneal angular velocity can provide the scientific community with detailed information regarding the mechanical-restriction properties of external ankle support in addition to angular displacement. The amount of subtalar-joint angular displacement an ankle brace may offer only provides information regarding the change in position of the subtalar joint with respect to time. Angular joint displacement does not measure the rate at which the change in angular position occurs. Often, joint injuries occur due to the rate at which the joint is displaced and not the amount of displacement itself. Each support device (tape, semirigid, or lace-up brace) contains some degree of elasticity. Accordingly, each type of ankle support exhibits viscoelastic properties, and the level of strain (percentage deformation) that each support can undergo depends on the rate at which the stress is applied.69 Thus, it is quite possible that 2 different ankle braces offer the same amount of joint-motion restriction but exhibit entirely different strain rates. Quantifying the amount of angular velocity at the ankle-foot complex can provide additional information regarding the mechanical efficacy of external ankle support.
Recently, investigators have quantified rearfoot angular velocity under various ankle-support conditions during a sudden inversion movement using an electrogoniometer41 and high-speed videography.70 In both studies, an inversion trapdoor was used to simulate the mechanism of injury of a traditional lateral ankle sprain. Rearfoot inversion average velocity decreased significantly with adhesive tape41 (40%) and a lace-up brace (38%)70 compared with a control condition. Additionally, the semirigid brace substantially decreased inversion average velocity (51%) compared with the lace-up style brace.70 These findings provide critical insight regarding the ability of external ankle support to reduce the rate of rearfoot movement during sudden inversion. Although a direct assessment of joint moments was not performed,41,70 these studies offer preliminary data suggesting that external ankle support may reduce the forces that cause subtalar joint motion during a simulated lateral ankle injury. More research is necessary to understand how external ankle support may modify talocrural and talocalcaneal angular velocity and acceleration during dynamic activity.
ANKLE PROPHYLAXES AND JOINT KINETICS
Greater evidence exists supporting the application of external ankle support in limiting ankle and foot passive ROM during static or quasistatic conditions. However, whether external ankle support reduces the forces that cause joint motion has been questioned. Because external ankle support reduces joint angular displacement and angular velocity, we may surmise that external ankle support attenuates the external forces that cause angular motion. The moments created at the talocrural and talocalcaneal joints under various ankle-brace conditions when the lower extremity is positioned in the closed kinetic chain have not been directly assessed. Yet isolated joint torque production22,71 and ground-reaction force components have been assessed during ankle-support applications (Table 2).8,72,73
Table 2. Examination of External Ankle Support on Joint Kinetics
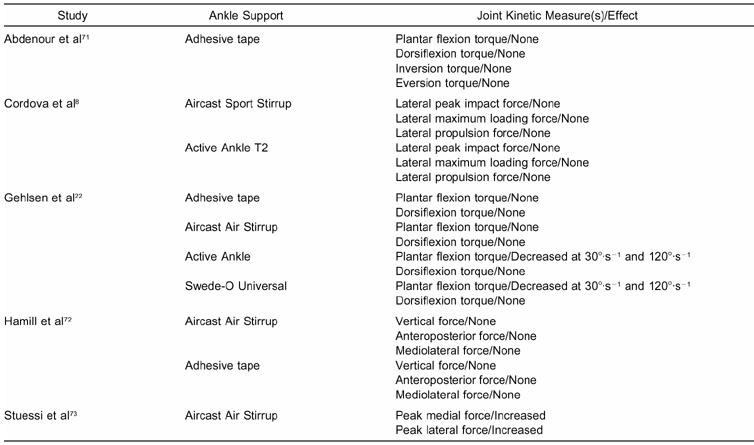
The question of whether external ankle support affects isolated ankle-foot torque production is not new.22,71 In one of the earliest studies assessing the influence of ankle taping, traditional application of adhesive tape had no adverse effects on isokinetic plantar-flexion, dorsiflexion, inversion, or eversion torque production.71 Although no treatment effect was reported, only 7 subjects participated in the study. Based on the data presented, it appears that a type I statistical error influenced the results. In a similar study investigating talocrural joint torque and total work,22 the Swede-O-Universal brace diminished plantar-flexion and dorsiflexion force production compared with the Aircast Sport Stirrup and Active Ankle Support but not tape at 30°·s−1. Also, dorsiflexion peak torque was not affected by the application of an ankle appliance. Further, the no-support condition and the Active Ankle brace were associated with significantly higher plantar-flexion work values than the Swede-O-Universal brace and adhesive tape.
The role of external ankle supports on the ground-reaction forces produced during a dynamic task has not been greatly explored. Developing insight into the pattern, magnitude, and temporal characteristics of the ground-reaction forces that occur in various ankle-support conditions could help to explain some of the kinematic changes affecting the ankle-foot complex. Evaluating the kinetics of movement allows for accurate assessment of the support mechanics used. In the few existing studies, some researchers72,73 evaluated the effects of the Aircast Sport Stirrup on ground-reaction forces during running, while another group8 evaluated these potential effects during a dynamic inversion shuffling movement.
Hamill et al72 evaluated the 3-dimensional components of ground-reaction force data using 2 common ankle-stabilizing appliances while subjects ran at a controlled speed of 5 m·s−1. The time to peak vertical impact force and the time to minimum vertical force were larger for the preexercise tape condition than the ankle-stabilizer conditions. In the anteroposterior (AP) force, the relative time to zero force was larger between the tape and ankle-stabilizer conditions. No difference was reported between ankle-support conditions for the mediolateral (ML) component. Although the external ankle support did not affect the magnitude of the ground-reaction forces, the time in which the forces were produced was slower. This suggests that the external support may attenuate forces at the ankle-foot complex by extending the amount of time in which they act. In a similar study73 of subjects with functionally unstable ankles while running, an Aircast Sport Stirrup brace increased peak medial force compared with the control condition. Additionally, the lateral forces generated in the brace condition decreased compared with those produced during the unbraced treatment. Moreover, the stability offered in the braced ankle reduced the ML velocity at foot contact compared with the control condition. These data suggest that the stiffness offered by the brace does, in fact, allow the forces generated at the ankle-foot complex to be attenuated and, perhaps, controlled.
More recently, the effects of the Active Ankle and Aircast Sport Stirrup semirigid brace on lateral ground-reaction forces were assessed while subjects performed a controlled shuffling movement. This movement was designed to produce a dynamic inversion loading on the ankle-foot complex in the lateral direction.8 Ankle bracing did not alter peak impact force, maximum loading force, or peak propulsion force in the lateral direction compared with the control condition. Thus, ankle bracing may not act as a force bypass when the talocural and subtalar joints are dynamically loaded in the lateral direction. A significant limitation exists when trying to compare the data presented in the 3 studies previously discussed.8,72,73 Earlier studies72,73 assessing the influence of ankle support on ground-reaction forces were performed on subjects running on a treadmill. External ankle supports are designed to be stressed in the frontal plane; running does not produce frontal-plane motion at the rearfoot and midfoot articulations, and so the devices are not stressed in the intended manner. Thus, the differences found in the Stuessi et al73 study may have been due to individual variability in gait among the 11 subjects. Cordova et al8 imposed a demand on the ankle-foot complex similar to what the external support is intended to control against. Although differences in lateral ground-reaction forces were not found, more work using similar methods is needed to further validate these effects.
It may be argued that assessing ground-reaction force data may not be the most direct method for estimating the forces exerted on the ankle-foot complex. Additional inquiry is required to estimate talocrural and talocalcaneal joint moments, either through inverse dynamics or forward solution modeling, under dynamic loads among various support conditions. Until this direct assessment is performed, researchers can only speculate as to the role external ankle support may have in reducing the forces imposed on the ankle-foot complex under dynamic loads.
ANKLE PROPHYLAXES AND SENSORIMOTOR FUNCTION
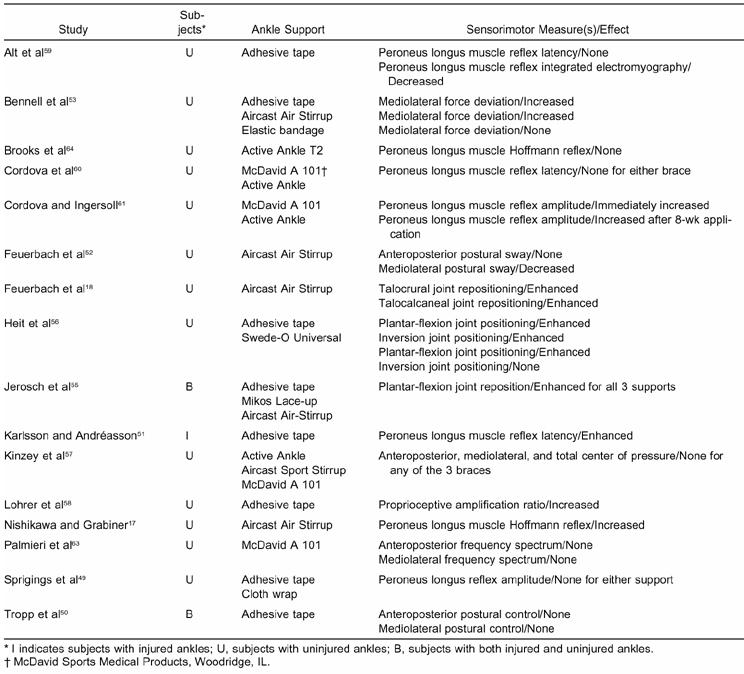
The effect of external ankle support on joint kinematics has been widely studied. Evidence is substantial that ankle support, offered through tape or a ready-made stabilizer, provides mechanical stability to the ankle-foot complex.39 To a much lesser degree, the potential effects of external ankle support on a few sensorimotor variables have been studied. Various sensorimotor values have been measured under the influence of external ankle support (Table 3). Such measures include peroneus longus (PL) muscle reaction time or latency,49,51,58–60 PL reflex amplitude,58,61 PL Hoffmann reflex,17,64 joint position sense or joint replication,18,55,56,74 and various measures of postural control.50,52,53,57,63 The sensorimotor variables in question have been measured during static and dynamic conditions.
Table 3. Examination of External Ankle Support on Sensorimotor Function
Ankle Support and Peroneus Longus Muscle Response
Peroneus longus neuromuscular function is critical in dynamically supporting the ankle-foot complex against an inversion mechanism of injury.6,7 As a result, PL reaction time, or latency, during a simulated ankle sprain has been predominantly studied in normal and chronically unstable ankles,6,7,75–81 while the effect of ankle support on PL function has not been studied as extensively.49,51,58–60 The duration of the PL latency quantified in these studies involves activation of the group Ia afferent fibers of the muscle spindle located in the muscle belly, which results in an efferent motor response and contraction of the same muscle.82 Although a large amount of research has been done examining peroneal muscle-reflex temporal characteristics during sudden inversion, this work has used a quasistatic model for assessment. The time and amplitude in which the peroneal muscles fire under this condition may not reflect what occurs during an injury. Ideally, peroneal muscle function would be assessed during a true dynamic state; however, due to the difficulty in controlling many extraneous variables under a true dynamic model, the use of inversion trapdoors and platforms to simulate an ankle injury has been widely accepted.6,7,49,51,58–60,75–81
In an earlier study of external ankle support and leg muscle function, Glick et al1 proposed that another benefit of taping the ankle, beyond its apparent mechanical restriction, is the stimulating effect on the peroneus brevis muscle. Individuals who suffered from excessive inversion talar tilt and whose ankles were taped initiated peroneus brevis contraction before heel strike during running gait.1 This theory suggests a potential proprioceptive benefit of applying adhesive tape51,58,59,65 or an ankle brace17,61 and that the prophylactic benefits of applying such devices may be more than just mechanical. When considering the effects of external ankle support on PL reflex latency, evidence exists regarding adhesive tape's efficacy. Peroneus longus reaction time was measured during sudden inversion in subjects with CAI whose ankles were taped.51 Chronically unstable ankles supported with tape demonstrated faster reaction times of the PL and peroneus brevis during rapid inversion compared with the unsupported condition.
Some researchers have shown no alteration in PL latency after the application of either adhesive tape or a ready-made ankle brace. In subjects with healthy ankles,59 no change in PL reflex latency with ankle taping was found before or after exercise. Their results were also supported by similar work,58 in which the PL response in healthy, uninjured ankles supported by athletic tape was not altered after sudden inversion. Additionally, Cordova et al60 reported that PL reaction time remained unaffected by a sudden inversion perturbation immediately after the application of a lace-up or semirigid ankle brace. Although none of these investigators58–60 found a significant reduction in PL latency, their findings can be viewed as a positive result regarding the application of external ankle support. The application of external ankle support (tape, lace-up brace, or semirigid brace) does not affect the latency of the reflex circuitry of the muscle spindles within the PL during sudden inversion.
Specifically, clinicians have surmised anecdotally that long-term application of an ankle brace weakens the ankle's supporting structures and causes remodeling that induces these structures to become dependent on this support. With the extended use of an ankle brace, the leg musculature's ability to respond to an external stimulus or perturbation may be delayed, thereby diminishing neuromuscular function and potentially placing the ankle-foot complex at risk for injury. Researchers have investigated the potential long-term effects of external ankle support on PL muscle function.60,61 Peroneus longus muscle latency during sudden inversion was assessed in subjects before and after having a lace-up and semirigid style brace applied 8 h·d−1 for 5 d·wk−1 over an 8-week period.60 No changes were observed in latency across subjects who were assigned to the lace-up or semirigid brace conditions compared with the control condition; thus, athletes with healthy ankles who wish to wear external ankle support for prophylactic considerations throughout the course of a season do not appear at risk for compromising the PL response to sudden inversion.
Understanding the time delay of the PL in the supported ankle as it responds to a sudden perturbation is certainly important; however, others have begun to evaluate neuromuscular characteristics such as electromyographic reflex amplitude.17,58,59,61,64 Although not much research has been done in this specific area, the data that do exist are promising in demonstrating the proprioceptive value of external ankle support. Lohrer et al58 explored the effects of adhesive tape on the proprioceptive amplification ratio (PAR) in healthy subjects. This variable is the ratio of integrated electromyographic activity of the peroneal muscles over the maximum inversion angle produced during sudden inversion. This value is then normalized to the ratio obtained during the control condition. After the application of tape, the PAR increased significantly. Increases in the PAR were found to occur as a result of increases in integrated electromyographic activity along with decreases in the maximum inversion angle.
The immediate and chronic effects of ankle bracing on PL reflex amplitude during sudden inversion have been studied.61 Normalized PL amplitude was significantly enhanced after a lace-up style brace was applied. Additionally, after 8 weeks of chronic brace use, normalized PL amplitude also increased. The results of this work are in agreement with a group17 that considered the effects of a semirigid brace on the PL Hoffmann reflex in a non-weight-bearing, recumbent seated position. Peroneus longus motoneuron pool excitability increased 10% after the application of a semirigid brace. They electrically stimulated the PL muscle group Ia afferent nerve fibers percutaneously and not through deformation of the muscle spindles using a trapdoor testing apparatus (simulated ankle sprain). This result may be viewed positively, as it suggests that these types of braces have an excitatory effect on the PL muscle. These data may support the hypothesis that ankle bracing positively enhances PL function through heightened afferent input from cutaneous mechanoreceptors.
Others have found decreases59 or no change64 in PL muscle amplitude after the application of external ankle support. In an attempt to evaluate joint stabilization provided by adhesive taping during a simulated inversion trauma, Alt et al59 found that PL-integrated electromyographic activity reduced significantly by 18% after adhesive tape was applied. They attributed this decrease in PL muscle activity to the decrease in inversion velocity found with the application of adhesive tape. Brooks et al64 assessed the PL Hoffmann reflex once a week over a 5-week period during semirigid ankle brace and control conditions in uninjured subjects. Use of an ankle brace over a 5-week period did not facilitate or inhibit PL muscle function. The proprioceptive effect of tape and ankle bracing on the underlying muscle groups may be an additional factor in preventing injury in individuals who suffer from CAI. This is critical, as the control and reflexive response of the peroneal muscles appears to have a substantial effect in preventing injury to the ankle-foot complex.
Ankle Support and Joint Proprioception
The importance of coordination and proprioceptive training in reducing the frequency of recurrent ankle sprains has been documented.9 Evidence indicating that mechanical stability is the main function of external ankle support is substantial.39 Others contend that not only does external ankle support provide mechanical stability, but it may also facilitate proprioceptive input of the ankle musculature.17,58,83 Although the role of external ankle support in providing mechanical joint stability is known, its effect on joint kinesthesia is less well understood. The ability to improve proprioception occurs not only through the use of exercise and rehabilitation84–86 but also through stimulation of cutaneous mechanoreceptors near and around the ankle by the application of various types of ankle support.17,18,55,56
One of the first well-controlled studies to determine the effects of a semirigid ankle brace on ankle-joint kinesthesia was reported in the mid 1990s.18 Joint position sense was measured 3-dimensionally using a motion-analysis system before and after applying a semirigid brace and anesthetizing the anterior talofibular and calcaneofibular ligamants.18 No significant differences were noted in the constant, variable, or absolute errors between the anesthetized and nonanesthetized conditions; however, both the constant and variable errors in matching reference points were significantly less with the brace than without the brace. Thus, mechanoreceptors within the ligaments tested contributed very little to ankle-joint proprioception as measured by joint replication. Afferent feedback from the cutaneous receptors in the foot and shank appears to be enhanced after application of an ankle brace. More recently, the positive effects of external ankle support on joint kinesthesia were reported.55 The authors investigated the effects of adhesive tape, a lace-up brace, and a semirigid brace on replicating ankle-joint position. The lace-up brace was associated with less angle-reproduction error than the semirigid brace or tape condition. Each ankle-support condition also demonstrated less angle error than the control condition. In a similar investigation, the effects of a lace-up style brace and adhesive tape on the ability to replicate inversion and plantar-flexion joint position in normal subjects were studied.56 Plantar-flexion and inversion joint replication was enhanced in the brace and tape conditions, but the 2 conditions did not differ from each other. Although the scientific evidence in this area is somewhat promising, more research is needed to clearly substantiate the positive effects of external ankle support on joint proprioception.
Ankle Support and Postural Control
Individuals with decreased postural control are believed to be more susceptible to ankle injury than those with better postural control.9,84 Rehabilitation programs employing coordination and balance training are effective in reducing recurrent ankle sprains.9,52,53 Ankle-joint function directly correlates with an individual's ability to maintain an upright stance.83 The potential effects of ankle bracing on postural control have been evaluated using stabilometry, in which many indices of postural control were assessed.50,52,53,57,63 Some of the more common postural-control dependent variables measured include center-of-pressure (COP) displacement in the AP and ML directions, total COP excursion, and frequency analysis of AP and ML COP data.
In an earlier investigation,50 subjects with a history of previous ankle sprains and functional instability were observed to determine if postural control could be improved with ankle taping. Stabilometric recordings of 38 soccer players with and without ankle taping showed that taping did not influence these measures. This work demonstrated that ankle taping had no influence on postural sway. In another study57 assessing the effects of ankle support on postural control, subjects wearing 3 selected ankle appliances were evaluated for COP trajectories in the AP and ML planes under 6 variations of a modified Romberg test. Application of external ankle support did not affect any of the COP measures in question. Thus, bracing did not interfere with the coherence of the 3 sensory systems (vision, vestibular, somatosensory) that integrate and collectively control the maintenance of upright stance.
In another study assessing the influence of ankle support on postural control,52 the scientists hypothesized that application of an ankle brace would decrease the amplitude and frequency of unilateral postural sway. Testing consisted of static and dynamic trials in which COP trajectories in the AP and ML planes were measured under a control condition and a semirigid brace condition. A decrease in lateral sway with the semirigid brace was observed, suggesting an improvement in lateral postural control. The findings of this study suggest that the semirigid brace acts to provide cutaneous afferent feedback in maintaining postural control. This feedback may be through the same neurologic pathways in which external ankle bracing has been shown to enhance the replication of joint position. In a similar investigation,53 different types of ankle support were compared for the number of foot contacts made by the subject's nonsupporting leg and on ML force produced during a 1-legged stance. In complete disagreement with previously reported data,52 the authors showed that ankle taping and a lace-up brace increased deviations in the ML force when compared with the control condition. In addition, the number of foot contacts made by the nonsupporting foot was increased in the braced conditions.53 Although these findings might suggest that ankle bracing has an adverse effect on postural control, caution should be taken in interpreting these results, as the methods and dependent variables assessed in this study are not representative of traditional postural-control investigations.
To further investigate external ankle support and postural control, researchers63 applied a lace-up ankle brace for 4 days to determine whether the spectral qualities of AP and ML COP excursions during a 1-legged stance would be affected by extensive reliance on the ankle support. The frequency content of the COP trajectories was assessed in an attempt to identify alterations in somatosensory control of posture. No differences existed between the brace and control conditions in AP and ML mean power frequencies. Therefore, application of an ankle brace may not require a modification in the postural-control strategy during a 1-legged stance in healthy subjects.57 Due to the conflicting evidence in the literature, the effect of external ankle support on postural control remains unclear. Research assessing the potential influence of external ankle support in chronically unstable ankles is lacking. As work continues in this area, scientists should focus on quantifying more sensitive aspects of postural control, using such methods as Fourier and time-frequency analyses of the COP coordinate data. These measures are more sensitive than traditional evaluation of COP displacement and are more revealing with regard to our understanding of how the somatosensory system may be affected by the application of external ankle support.
ANKLE PROPHYLAXES AND FUNCTIONAL PERFORMANCE
Of all the empirical data surrounding the use of external ankle support, the impact of these devices on functional performance is probably most important. Although these devices are beneficial in preventing ankle injury,9–11,14 athletes will avoid wearing ankle supports if they perceive that athletic performance will be hindered. The main purpose of ankle prophylactic devices is to restrict frontal-plane motion occurring at the subtalar joint; however, movement in the sagittal plane is constrained as well, which may interfere with the execution of functional tasks. Prophylactic ankle taping and bracing are not likely to gain wide acceptance in the athletic population if they impede performance. Therefore, it is essential to recognize whether external ankle support hinders an individual's ability to carry out sport-specific tasks. The impact of various ankle prophylaxes on different facets of functional performance will be discussed.
Ankle Support and Running Speed
A dominant movement included in most aspects of physical activity is running. Running speed is an important component for successful performance in many competitive athletic events. The design of an external ankle support may restrict foot and ankle motions that are necessary to propel the body at adequate speeds; thus, the beneficial effects of ankle support in preventing injury may come at the cost of hindering performance. Several investigators30,44,45,87–91 have examined the effects of ankle taping and bracing on speed. The type of ankle stabilizer, distance of the sprint test, and how the external support potentially affected this performance varied for each of the studies reported (Table 4). Most subjects were competitive athletes, but several investigators28,87 observed ankle-support effects in recreational athletes.
Table 4. Examinations of External Ankle Support on Sprint Performance
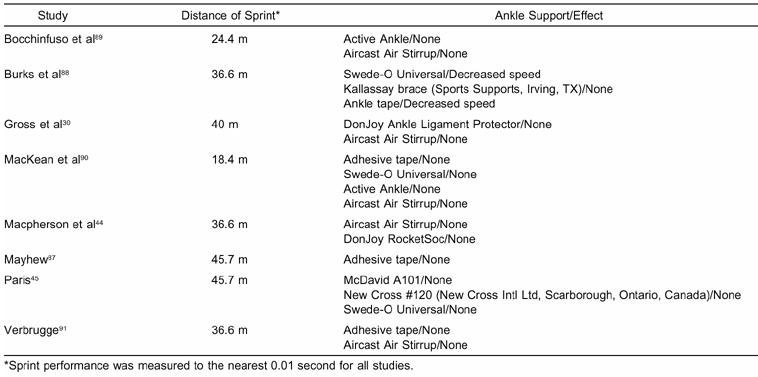
Overwhelmingly, sprint time was not affected by the application of an external ankle device30,44,45,87,89–91; however, others found a decrease in sprint performance.88 The description of the testing procedures used in this latter study is vague, which complicates the comparison of these results with those of similar studies. The authors failed to report subject-exclusion criteria, the testing instruments used, and how each test was performed. Therefore, the results presented may be flawed and should be applied cautiously. Due to the convincing evidence indicating that applying external ankle support does not hinder sprint performance, clinicians should not be concerned about healthy subjects using ankle stabilizers for prophylactic reasons.
Ankle Support and Agility
To determine if external ankle stabilizers affect agility, many testing protocols were created to challenge the coordination and speed of subjects (Table 5). The agility drills required quick changes in direction, moments of accelerations and deceleration, and sprinting. The prophylactic ankle devices generally did not alter agility; however, a few studies revealed variations from this majority upon application of an external ankle stabilizer.24,43
Table 5. Examinations of External Ankle Support on Agility Performance
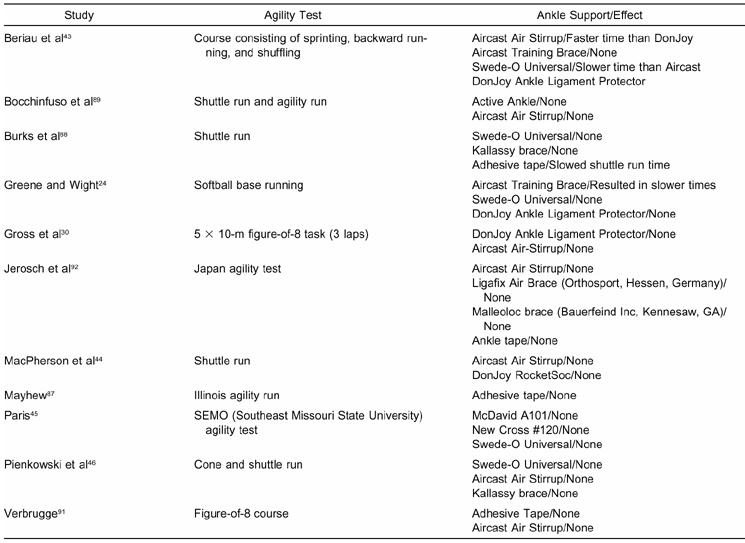
Performance restrictions were evaluated in subjects tested while wearing an external ankle device.43 Subjects wearing the Aircast Training brace performed faster (22.3 seconds) on the agility course when compared with subjects wearing the DonJoy Ankle Ligament Protector (22.7 seconds). Although this time difference was statistically significant, the observed increase would be irrelevant when applied to an actual agility-type event. No detrimental effects were noted for any of the ankle stabilizers when compared with the control condition. This suggests that the agility drills used in the study were unaffected by the use of ankle bracing. Greene and Wight24 found that the Aircast Training brace resulted in significantly slower base-running times (13.79 seconds versus 12.84 seconds without support), while the other external ankle-support devices (Swede-O Universal and DonJoy Ankle Ligament Protector) did not impede base-running performance. The decreased running speed was attributed to the design of the Aircast training brace. The Aircast contains an air cylinder and a rigid material useful in restricting frontal-plane motion. The excess material in this ankle stabilizer may have hindered the subjects' ability to make the sharp directional changes required to run the bases; however, numerous other researchers examining the effect of the Aircast Sport Stirrup on agility found no differences from the control condition.30,43,44,46,89–92 After examining the collective research, it becomes apparent that external ankle support has virtually no effect on agility.
Ankle Support and Vertical Jump
Lace-up style ankle support and traditional adhesive-tape application incorporate material anterior and posterior to the talocrural joint axis, which may restrict the extremes of sagittal-plane motion. Restriction of plantar-flexion and dorsiflexion movement is likely to impede vertical-jump performance. Therefore, if ankle taping and bracing prevent optimal performance of this task, it is unlikely that athletes will use these devices, which could potentially predispose these individuals to ankle-foot injury. The most commonly reported method of assessing vertical jump involves measuring the difference in distance between the subject's highest reach on a wall when standing (using the tip of the middle finger as the indicator) and the highest point reached during the jump. Some investigators allowed subjects to gain a running start when measuring the highest point of their jump,93,94 while others did not report the procedures used to measure vertical-jump height.87,88
Similar to the other results examining motor performance after the application of external ankle support, most evidence suggests that these devices do not alter vertical-jump height (Table 6).30,44–46,89–91 However, some data suggest otherwise.45,87,88,93 In 2 of the earliest studies, authors87,93 evaluating the effects of prophylactic ankle taping on vertical-jump performance in healthy subjects observed a significant decrease in vertical height when compared with a control condition. Moreover, other researchers45 observed significant deficits in vertical-jump performance with the application of the New Cross lace-up style brace, the Swede-O Universal brace, and the Kallassy brace.88 The decrement in vertical jump in these studies ranged from 3.4% to 5.4% compared with control conditions.
Table 6. Examinations of External Ankle Support on Vertical Jump Performance
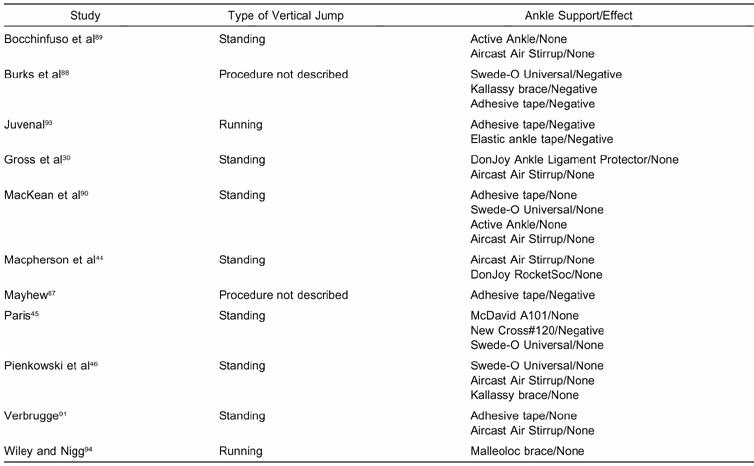
The different results among studies examining vertical jump are likely due to the various testing procedures employed. A variety of starting positions was used, and some investigations allowed the dominant foot to step forward first,30,91 while others required a step approach.93,94 Most researchers placed the subjects in a crouched position before they performed the vertical jump.44,46,89,90,93,94 Additionally, each study's protocol required a different number of trials (ranging from 1 to 5) in order to determine the vertical-jump height.
The mechanism for diminished vertical-jump performance in the presence of lace-up style bracing and adhesive taping can be best explained by the inherent design of these devices. The lace-up stabilizers and ankle taping may have produced plantar-flexion ROM restrictions that contributed to a diminished jump height. Vertical-jump height can certainly become impaired if the external ankle support decreases this functional ROM. Talocrural motion and torque production in the sagittal plane are critical components of any jumping task, as they assist in propulsion from the ground. Restricted plantar flexion from an external ankle stabilizer would likely impair jump height. Although restricting plantar flexion may contribute to the ability of external ankle support to help prevent injury, it may also hinder vertical-jump performance.
The effect of ankle prophylaxes on functional performance has been examined with speed, agility, and vertical jump as the primary dependent measures. The functional ROM allowed at the ankle-foot complex upon application of external ankle stabilizers is determined by the structure and design of the brace. Plantar flexion is restricted by ankle taping and lace-up style bracing, which may contribute to impeding functional performance. Although the results of the studies presently reviewed are not 100% conclusive, most of the information currently available suggests that external ankle support produces minimal to small decrements on lower extremity functional-performance tests evaluating speed, agility, and vertical-jump ability.
CONCLUSIONS
The use of external ankle supports in sports medicine will continue due to the high incidence of ankle injuries that occur in sport and recreational activity each year. Prophylactic ankle support is primarily advocated for the mechanical stability these devices provide. An abundant amount of research exists to document the effectiveness of external ankle support in restricting ankle and foot range of motion during static positions. Unfortunately, few data exist to help us understand how external ankle supports may act to control joint motion and attenuate joint forces during dynamic activities such as running and lateral-cutting maneuvers. More scientific inquiry is necessary to define the potential role of ankle support in reducing forces and loads placed on the ankle-foot complex. Evidence is emerging that external-ankle support use may also be beneficial by enhancing proprioceptive function of the ankle-foot complex. The implications surrounding this area of study are large, and other factors may be further delineated as we understand the mechanisms by which external ankle supports help prevent injury. It is our contention that this area should be the primary focus of future study involving the use of external ankle support. The potential influence of external ankle supports on lower extremity functional performance has been the subject of many research investigations. The literature shows quite clearly that external ankle support does not impair an individual's sprint time and agility. Although some work has shown vertical-jump performance to be negatively affected with the use of external ankle support, most of the literature in this area has demonstrated no deleterious effects of such appliances.
REFERENCES
- Glick J M, Gordon R B, Nishimoto D. The prevention and treatment of ankle injuries. Am J Sports Med. 1976;4:136–141. doi: 10.1177/036354657600400402. [DOI] [PubMed] [Google Scholar]
- Garrick J G. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains. Am J Sports Med. 1977;5:241–242. doi: 10.1177/036354657700500606. [DOI] [PubMed] [Google Scholar]
- Garrick J G, Requa R K. The epidemiology of foot and ankle injuries in sports. Clin Sports Med. 1988;7:29–36. [PubMed] [Google Scholar]
- Lassiter T E, Jr, Malone T R, Garrett W E., Jr Injury to the lateral ligaments of the ankle. Orthop Clin North Am. 1989;20:629–640. [PubMed] [Google Scholar]
- Miller E A, Hergenroeder A C. Prophylactic ankle bracing. Pediatr Clin North Am. 1990;37:1175–1185. doi: 10.1016/s0031-3955(16)36982-6. [DOI] [PubMed] [Google Scholar]
- Isakov E, Mizrahi J, Solzi P. Response of the peroneal muscles to sudden inversion of the ankle during standing. Int J Sport Biomech. 1986;2:100–109. [Google Scholar]
- Konradsen L, Voigt M, Hojsgaard C. Ankle inversion injuries: the role of the dynamic defense mechanism. Am J Sports Med. 1997;25:54–58. doi: 10.1177/036354659702500110. [DOI] [PubMed] [Google Scholar]
- Cordova M L, Armstrong C W, Rankin J M, Yeasting R A. Ground reaction forces and EMG activity with ankle bracing during inversion stress. Med Sci Sports Exerc. 1998;30:1363–1370. doi: 10.1097/00005768-199809000-00004. [DOI] [PubMed] [Google Scholar]
- Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med. 1985;13:259–262. doi: 10.1177/036354658501300408. [DOI] [PubMed] [Google Scholar]
- Rovere G D, Clarke T J, Yates C S, Burley K. Retrospective comparison of taping and ankle stabilizers in preventing ankle injuries. Am J Sports Med. 1988;16:228–233. doi: 10.1177/036354658801600305. [DOI] [PubMed] [Google Scholar]
- Surve I, Schwellnus M P, Noakes T, Lombard C. A fivefold reduction in the incidence of recurrent ankle sprains in soccer players using the Sport-Stirrup orthosis. Am J Sports Med. 1994;22:601–606. doi: 10.1177/036354659402200506. [DOI] [PubMed] [Google Scholar]
- Sitler M, Ryan J, Wheeler B, et al. The efficacy of a semirigid ankle stabilizer to reduce acute ankle injuries in basketball: a randomized clinical study at West Point. Am J Sports Med. 1994;22:454–461. doi: 10.1177/036354659402200404. [DOI] [PubMed] [Google Scholar]
- Löfvenberg R, Kärrholm J. The influence of an ankle orthosis on the talar and calcaneal motions in chronic lateral instability of the ankle: a stereophotogrammetric analysis. Am J Sports Med. 1993;21:224–230. doi: 10.1177/036354659302100211. [DOI] [PubMed] [Google Scholar]
- Sitler M R, Horodyski M. Effectiveness of prophylactic ankle stabilisers for prevention of ankle injuries. Sports Med. 1995;20:53–57. doi: 10.2165/00007256-199520010-00005. [DOI] [PubMed] [Google Scholar]
- Garrick J G. Epidemiologic perspective. Clin Sports Med. 1982;1:13–18. [PubMed] [Google Scholar]
- Bahr R, Karlsen R, Lian O, Ovrebo R V. Incidence and mechanisms of acute ankle inversion injuries in volleyball: a retrospective cohort study. Am J Sports Med. 1994;22:595–600. doi: 10.1177/036354659402200505. [DOI] [PubMed] [Google Scholar]
- Nishikawa T, Grabiner M D. Peroneal motoneuron excitability increases immediately following application of a semirigid ankle brace. J Orthop Sports Phys Ther. 1999;29:168–176. doi: 10.2519/jospt.1999.29.3.168. [DOI] [PubMed] [Google Scholar]
- Feuerbach J W, Grabiner M D, Koh T J, Weiker G G. Effect of an ankle orthosis and ankle ligament anesthesia on ankle joint proprioception. Am J Sports Med. 1994;22:223–229. doi: 10.1177/036354659402200212. [DOI] [PubMed] [Google Scholar]
- Alves J W, Alday R V, Ketcham D L, Lentell G L. A comparison of the passive support provided by various ankle braces. J Orthop Sports Phys Ther. 1992;15:10–18. doi: 10.2519/jospt.1992.15.1.10. [DOI] [PubMed] [Google Scholar]
- Anderson D L, Sanderson D J, Henning E M. The role of external nonrigid ankle bracing in limiting ankle inversion. Clin J Sport Med. 1995;5:18–24. doi: 10.1097/00042752-199501000-00004. [DOI] [PubMed] [Google Scholar]
- Bunch R P, Bednarski K, Holland D, Macinanti R. Ankle joint support: a comparison of reusable lace-on braces with taping and wrapping. Physician Sportsmed. 1985;13(3):59–62. doi: 10.1080/00913847.1985.11708789. [DOI] [PubMed] [Google Scholar]
- Gehlsen T A, Pearson D, Bahamonde R. Ankle joint strength, total work, and ROM: comparison between prophylactic devices. J Athl Train. 1991;26:62–65. [Google Scholar]
- Greene T A, Roland G C. A comparative isokinetic evaluation of a functional ankle orthosis on talocalcaneal function. J Orthop Sports Phys Ther. 1989;11:245–252. doi: 10.2519/jospt.1989.11.6.245. [DOI] [PubMed] [Google Scholar]
- Greene T A, Wight C R. A comparative support evaluation of three ankle orthoses before, during, and after exercise. J Orthop Sports Phys Ther. 1990;11:453–466. doi: 10.2519/jospt.1990.11.10.453. [DOI] [PubMed] [Google Scholar]
- Greene T A, Hillman S K. Comparison of support provided by a semirigid orthosis and adhesive ankle taping before, during, and after exercise. Am J Sports Med. 1990;18:498–506. doi: 10.1177/036354659001800509. [DOI] [PubMed] [Google Scholar]
- Gross M T, Bradshaw M K, Ventry L C, Weller K H. Comparison of support provided by ankle taping and semirigid orthosis. J Orthop Sports Phys Ther. 1987;9:33–39. doi: 10.2519/jospt.1987.9.1.33. [DOI] [PubMed] [Google Scholar]
- Gross M T, Lapp A K, Davis J M. Comparison of Swede-O-Universal Ankle Support and Aircast Sport-Stirrup orthoses and ankle tape in restricting eversion-inversion before and after exercise. J Orthop Sports Phys Ther. 1991;13:11–19. [Google Scholar]
- Gross M T, Ballard C L, Mears H G, Watkins E J. Comparison of Donjoy Ankle Ligament Protector and Aircast Sport-Stirrup orthoses in restricting foot and ankle motion before and after exercise. J Orthop Sports Phys Ther. 1992;16:60–67. [Google Scholar]
- Gross M T, Batten A M, Lamm A L, et al. Comparison of DonJoy Ankle Ligament Protector and subtalar sling ankle taping in restricting foot and ankle motion before and after exercise. J Orthop Sports Phys Ther. 1994;19:33–41. doi: 10.2519/jospt.1994.19.1.33. [DOI] [PubMed] [Google Scholar]
- Gross M T, Everts J R, Roberson S E, Roskin D S, Young K D. Effect of DonJoy Ankle Ligament Protector and Aircast Sport-Stirrup orthoses on functional performance. J Orthop Sports Phys Ther. 1994;19:150–156. doi: 10.2519/jospt.1994.19.3.150. [DOI] [PubMed] [Google Scholar]
- Kimura I F, Nawoczenski D A, Epler M, Owen M G. Effect of the Air Stirrup in controlling ankle inversion stress. J Orthop Sports Phys Ther. 1987;9:190–193. doi: 10.2519/jospt.1987.9.5.190. [DOI] [PubMed] [Google Scholar]
- Martin N, Harter R A. Comparison of inversion restraint provided by ankle prophylactic devices before and after exercise. J Athl Train. 1993;28:324–329. [PMC free article] [PubMed] [Google Scholar]
- Paris D L, Vardaxis V, Kokkaliaris J. Ankle ranges of motion during extended activity periods while taped and braced. J Athl Train. 1995;30:223–228. [PMC free article] [PubMed] [Google Scholar]
- Myburgh K H, Vaughan C L, Isaacs S K. The effects of ankle guards and taping on joint motion before, during, and after a squash match. Am J Sports Med. 1984;12:441–446. doi: 10.1177/036354658401200607. [DOI] [PubMed] [Google Scholar]
- Pederson T S, Ricard M D, Merrill M S, Schulthies S S, Allsen P E. The effects of spatting and ankle taping on inversion before and after exercise. J Athl Train. 1997;32:29–33. [PMC free article] [PubMed] [Google Scholar]
- Seitz C J, Goldfuss A J. The effect of taping and exercise on passive foot inversion and ankle plantarflexion. Athl Train. 1984;19:178–182. [Google Scholar]
- Simpson K J, Cravens S, Higbie E, Theodorou C, DelRey P. A comparison of the SportStirrup, Malleoloc, and Swede-O ankle orthoses for the foot-ankle kinematics of a rapid lateral movement. Int J Sports Med. 1999;20:396–402. doi: 10.1055/s-2007-971151. [DOI] [PubMed] [Google Scholar]
- Wilkerson G B. Comparative biomechanical effects of the standard method of ankle taping and a taping method designed to enhance subtalar stability. Am J Sports Med. 1991;19:588–595. doi: 10.1177/036354659101900606. [DOI] [PubMed] [Google Scholar]
- Cordova M L, Ingersoll C D, LeBlanc M J. Influence of ankle support on joint range of motion before and after exercise: a meta-analysis. J Orthop Sports Phys Ther. 2000;30:170–182. doi: 10.2519/jospt.2000.30.4.170. [DOI] [PubMed] [Google Scholar]
- Nishikawa T, Kurosaka M, Mizuno K, Grabiner M. Protection and performance effects of ankle bracing. Int Orthop. 2000;24:285–288. doi: 10.1007/s002640000170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ricard M D, Sherwood S M, Schulthies S S, Knight K L. Effects of tape and exercise on dynamic ankle inversion. J Athl Train. 2000;35:31–37. [PMC free article] [PubMed] [Google Scholar]
- Robinson J R, Frederick E C, Cooper L B. Systematic ankle stabilization and the effect on performance. Med Sci Sports Exerc. 1986;18:625–628. [PubMed] [Google Scholar]
- Beriau M R, Cox W B, Manning J. Effects of ankle braces upon agility course performance in high school athletes. J Athl Train. 1994;29:224–230. [PMC free article] [PubMed] [Google Scholar]
- Macpherson K, Sitler M, Kimura I, Horodyski M. Effects of a semirigid and softshell prophylactic ankle stabilizer on selected performance tests among high school football players. J Orthop Sports Phys Ther. 1995;21:147–152. doi: 10.2519/jospt.1995.21.3.147. [DOI] [PubMed] [Google Scholar]
- Paris D L. The effects of the Swede-O, New Cross, and McDavid ankle braces and adhesive ankle taping on speed, balance, agility, and vertical jump. J Athl Train. 1992;27:253–256. [PMC free article] [PubMed] [Google Scholar]
- Pienkowski D, McMorrow M, Shapiro R, Caborn D N, Stayton J. The effect of ankle stabilizers on athletic performance: a randomized prospective study. Am J Sports Med. 1995;23:757–762. doi: 10.1177/036354659502300621. [DOI] [PubMed] [Google Scholar]
- Bot S D, van Mechelen W. The effect of ankle bracing on athletic performance. Sports Med. 1999;27:171–178. doi: 10.2165/00007256-199927030-00003. [DOI] [PubMed] [Google Scholar]
- Hals T M, Sitler M R, Mattacola C G. Effect of a semi-rigid ankle stabilizer on performance in persons with functional ankle instability. J Orthop Sports Phys Ther. 2000;30:552–556. doi: 10.2519/jospt.2000.30.9.552. [DOI] [PubMed] [Google Scholar]
- Sprigings E J, Pelton J D, Brandell B R. An EMG analysis of the effectiveness of external ankle support during sudden ankle inversion. Can J Appl Sci. 1981;6:72–75. [PubMed] [Google Scholar]
- Tropp H, Ekstrand J, Gillquist J. Factors affecting stabilometry recordings of single limb stance. Am J Sports Med. 1984;12:185–188. doi: 10.1177/036354658401200302. [DOI] [PubMed] [Google Scholar]
- Karlsson J, Andréasson G O. The effect of external ankle support in chronic lateral ankle joint instability: an electromyographic study. Am J Sports Med. 1992;20:257–261. doi: 10.1177/036354659202000304. [DOI] [PubMed] [Google Scholar]
- Feuerbach J W, Grabiner M D. Effect of the Aircast on unilateral postural control: amplitude and frequency variables. J Orthop Sports Phys Ther. 1993;17:149–154. doi: 10.2519/jospt.1993.17.3.149. [DOI] [PubMed] [Google Scholar]
- Bennell K L, Goldie P A. The differential effects of external ankle support on postural control. J Orthop Sports Phys Ther. 1994;20:287–295. doi: 10.2519/jospt.1994.20.6.287. [DOI] [PubMed] [Google Scholar]
- Robbins S, Waked E, Rappel R. Ankle taping improves proprioception before and after exercise in young men. Br J Sports Med. 1995;29:242–247. doi: 10.1136/bjsm.29.4.242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surg Sports Traumatol Arthrosc. 1995;3:39–46. doi: 10.1007/BF01553524. [DOI] [PubMed] [Google Scholar]
- Heit E J, Lephart S M, Rozzi S L. The effect of ankle bracing and taping on joint position sense in the stable ankle. J Sport Rehabil. 1996;5:206–213. [Google Scholar]
- Kinzey S J, Ingersoll C D, Knight K L. The effects of selected ankle appliances on postural control. J Athl Train. 1997;32:300–303. [PMC free article] [PubMed] [Google Scholar]
- Lohrer H, Alt W, Gollhofer A. Neuromuscular properties and functional aspects of taped ankles. Am J Sports Med. 1999;27:69–75. doi: 10.1177/03635465990270012001. [DOI] [PubMed] [Google Scholar]
- Alt W, Lohrer H, Gollhofer A. Functional properties of adhesive ankle taping: neuromuscular and mechanical effects before and after exercise. Foot Ankle Int. 1999;20:238–245. doi: 10.1177/107110079902000406. [DOI] [PubMed] [Google Scholar]
- Cordova M L, Cardona C V, Ingersoll C D, Sandrey M A. Long-term ankle brace use does not affect peroneus longus muscle latency during sudden inversion in normal subjects. J Athl Train. 2000;35:407–411. [PMC free article] [PubMed] [Google Scholar]
- Cordova M L, Ingersoll C D. The effect of chronic ankle brace use on peroneus longus stretch reflex amplitude [abstract] Med Sci Sports Exerc. 2000;32(suppl):274. [Google Scholar]
- Refshauge K M, Kilbreath S L, Raymond J. The effect of recurrent ankle inversion sprain and taping on proprioception at the ankle. Med Sci Sports Exerc. 2000;32:10–15. doi: 10.1097/00005768-200001000-00003. [DOI] [PubMed] [Google Scholar]
- Palmieri R P, Ingersoll C D, Cordova M L, Kinzey S J. Prolonged ankle brace application does not affect the spectral properties of postural sway [abstract] Med Sci Sports Exerc. 2001;33(suppl):153. [Google Scholar]
- Brooks J, De La Garza B, Laramee M, Cordova M L, Ingersoll C D, Merrick M A. Effects of 5-week ankle brace use on peroneus longus H-reflex and eversion strength [abstract] J Athl Train. 2001;33:S51. [Google Scholar]
- Fumich R M, Ellison A E, Guerin G J, Grace P D. The measured effect of taping on combined foot and ankle motion before and after exercise. Am J Sports Med. 1981;9:165–170. doi: 10.1177/036354658100900307. [DOI] [PubMed] [Google Scholar]
- Hughes L Y, Stetts D M. A comparison of ankle taping and a semirigid support. Physician Sportsmed. 1983;11(4):99–103. [Google Scholar]
- Shapiro M S, Kabo J M, Mitchell P W, Loren G, Tsenter M. Ankle sprain prophylaxis: an analysis of the stabilizing effects of braces and tape. Am J Sports Med. 1994;22:78–82. doi: 10.1177/036354659402200114. [DOI] [PubMed] [Google Scholar]
- McIntyre D R, Smith M A, Denniston N L. The effectiveness of strapping techniques during prolonged dynamic exercises. J Athl Train. 1983;18:52–55. [Google Scholar]
- Whiting W C, Zernicke R F. Human Kinetics; Champaign, IL: 1998. Biomechanics of Musculoskeletal Injury. [Google Scholar]
- Dorrough J L, Orton K L, Cordova M L, Ingersoll C D, Merrick M L. Effects of ankle bracing on rearfoot motion during sudden inversion [abstract] J Athl Train. 2001;33(suppl):S-51. [Google Scholar]
- Abdenour T E, Saville W A, White R C, Abdenour M A. The effect of ankle taping upon torque and range of motion. Athl Train. 1979;14:227–228. [Google Scholar]
- Hamill J, Knutzen K M, Bates B T, Kirkpatrick G. Evaluation of two ankle appliances using ground reaction force data. J Orthop Sports Phys Ther. 1986;7:244–249. doi: 10.2519/jospt.1986.7.5.244. [DOI] [PubMed] [Google Scholar]
- Stuessi E, Tiegermann V, Gerber H, Raemy H, Stacoff A. A biomechanical study of the stabilization effect of the Aircast Ankle Brace. In: Jonsson B, editor. Biomechanics X. Human Kinetics; Champaign, IL: 1987. pp. 159–164. [Google Scholar]
- Simoneau G G, Degner R M, Kramper C A, Kittleson K H. Changes in ankle joint proprioception resulting from strips of athletic tape applied over the skin. J Athl Train. 1997;32:141–147. [PMC free article] [PubMed] [Google Scholar]
- Nawoczenski D A, Owen M G, Ecker M L, Altman B, Epler M. Objective evaluation of peroneal response to sudden inversion stress. J Orthop Sports Phys Ther. 1985;7:107–109. doi: 10.2519/jospt.1985.7.3.107. [DOI] [PubMed] [Google Scholar]
- Konradsen L, Ravn J B. Ankle instability caused by prolonged peroneal reaction time. Acta Orthop Scand. 1990;61:388–390. doi: 10.3109/17453679008993546. [DOI] [PubMed] [Google Scholar]
- Konradsen L, Ravn J B. Prolonged peroneal reaction time in ankle instability. Int J Sports Med. 1991;12:290–292. doi: 10.1055/s-2007-1024683. [DOI] [PubMed] [Google Scholar]
- Johnson M B, Johnson C L. Electromyographic response of peroneal muscles in surgical and nonsurgical injured ankles during sudden inversion. J Orthop Sports Phys Ther. 1993;18:497–501. doi: 10.2519/jospt.1993.18.3.497. [DOI] [PubMed] [Google Scholar]
- Vaes P, Van Gheluwe B, Duquet W. Control of acceleration during sudden ankle supination in people with unstable ankles. J Orthop Sports Phys Ther. 2001;31:741–752. doi: 10.2519/jospt.2001.31.12.741. [DOI] [PubMed] [Google Scholar]
- Löfvenberg R, Karrholm J, Sundelin G, Ahlgren O. Prolonged reaction time in patients with chronic lateral instability of the ankle. Am J Sports Med. 1995;23:414–417. doi: 10.1177/036354659502300407. [DOI] [PubMed] [Google Scholar]
- Ebig M, Lephart S M, Burdett R G, Miller M C, Pincivero D M. The effect of sudden inversion stress on EMG activity of the peroneal and tibialis anterior muscles in the chronically unstable ankle. J Orthop Sports Phys Ther. 1997;26:73–77. doi: 10.2519/jospt.1997.26.2.73. [DOI] [PubMed] [Google Scholar]
- Leonard C T. Mosby; St Louis, MO: 1998. The Neuroscience of Human Movement. [Google Scholar]
- Freeman M A, Dean M R, Hanham I W. The etiology and prevention of functional instability of the foot. J Bone Joint Surg Br. 1965;47:678–685. [PubMed] [Google Scholar]
- Goldie P A, Evans O M, Bach T M. Postural control following inversion injuries of the ankle. Arch Phys Med Rehabil. 1994;75:969–975. [PubMed] [Google Scholar]
- Sheth P, Yu B, Laskowski E R, An K N. Ankle disk training influences reaction times of selected muscles in a simulated ankle sprain. Am J Sports Med. 1997;25:538–543. doi: 10.1177/036354659702500418. [DOI] [PubMed] [Google Scholar]
- Docherty C L, Moore J H, Arnold B L. Effects of strength training on strength development and joint position sense in functionally unstable ankles. J Athl Train. 1998;33:310–314. [PMC free article] [PubMed] [Google Scholar]
- Mayhew J L. Effects of ankle taping on motor performance. Athl Train. 1972;7:10–11. [Google Scholar]
- Burks R T, Bean B G, Marcus R, Barker H B. Analysis of athletic performance with prophylactic ankle devices. Am J Sports Med. 1991;19:104–106. doi: 10.1177/036354659101900202. [DOI] [PubMed] [Google Scholar]
- Bocchinfuso C, Sitler M R, Kimura I F. Effects of two semirigid prophylactic ankle stabilizers on speed, agility, and vertical jump. J Sport Rehabil. 1994;3:125–134. [Google Scholar]
- MacKean L C, Bell G, Burnham R S. Prophylactic ankle bracing vs. taping: effects on functional performance in female basketball players. J Orthop Sports Phys Ther. 1995;22:77–81. doi: 10.2519/jospt.1995.22.2.77. [DOI] [PubMed] [Google Scholar]
- Verbrugge J D. The effects of semirigid Air-Stirrup bracing vs. adhesive ankle taping on motor performance. J Orthop Sports Phys Ther. 1996;23:320–325. doi: 10.2519/jospt.1996.23.5.320. [DOI] [PubMed] [Google Scholar]
- Jerosch J, Thorwesten L, Frebel T, Linnenbecker S. Influence of external stabilizing devices of the ankle on sport-specific capabilities. Knee Surg Sports Traumatol Arthrosc. 1997;5:50–57. doi: 10.1007/s001670050025. [DOI] [PubMed] [Google Scholar]
- Juvenal J P. The effects of ankle taping on vertical jumping ability. Athl Train. 1972;7:146–149. [Google Scholar]
- Wiley J P, Nigg B M. The effect of an ankle orthosis on ankle range of motion and performance. J Orthop Sports Phys Ther. 1996;23:362–369. doi: 10.2519/jospt.1996.23.6.362. [DOI] [PubMed] [Google Scholar]