

Abstract
Objective: Chronic instability after lateral ankle sprain has been shown to cause balance deficits during quiet standing. Although static balance assessment in those with ankle instability has been thoroughly examined in the literature, few researchers have studied performance on more dynamic tasks. Our purpose was to determine if the Star Excursion Balance Tests (SEBTs), lower extremity reach tests, can detect deficits in subjects with chronic ankle instability.
Design and Setting: We performed all testing in a university athletic training facility. We tested lower extremity reach using the SEBTs, which incorporates single-leg stance with maximal reach of the contralateral leg.
Subjects: Twenty subjects with unilateral, chronic ankle instability (age = 19.8 ± 1.4 years, height = 176.8 ± 4.5 cm, mass = 82.9 ± 21.2 kg) and 20 uninjured subjects matched by sex, sport, and position (age = 20.2 ± 1.4 years, height = 178.7 ± 4.1 cm, mass = 82.7 ± 19.9 kg).
Measurements: We measured the reach distances in centimeters (cm) and averaged 3 reaches in each of the 8 directions while the subjects stood on each leg for data analysis.
Results: The group with chronic ankle instability demonstrated significantly decreased reach while standing on the injured limb compared with the matched limb of the uninjured group (78.6 cm versus 82.8 cm). Additionally, subjects with chronic ankle instability reached significantly less when standing on their injured limbs as compared with their uninjured limbs (78.6 cm versus 81.2 cm).
Conclusions: The SEBTs appear to be an effective means for determining reach deficits both between and within subjects with unilateral chronic ankle instability.
Keywords: functional reach, dynamic balance, postural control, ankle sprain
Lateral ankle sprain (LAS) is among the most common injuries in sport.1–5 The incidence of residual symptoms and development of chronic ankle instability (CAI) after LAS have been reported to be between 31% and 40%.6–9 When LAS occurs, damage not only occurs to the structural integrity of the ligaments but also to various mechanoreceptors in the joint capsules, ligaments, and tendons about the ankle complex.9–12 Collectively, these receptors offer feedback regarding joint pressure and tension, ultimately providing a sense of joint movement and position.9,12 Via afferent nerve fibers, this information is integrated with the visual and vestibular sensory systems into a complex control system that acts to control posture and coordination.13 When afferent input is altered after injury, appropriate corrective muscular contractions may be altered. Thus, damage to the mechanoreceptors surrounding the ankle joint with an LAS may contribute to functional impairments and chronic instability subsequent to initial injury.9,12,14
Postural-control deficits during quiet standing after acute LAS and in those with CAI have been frequently reported6–7,15–20; however, the sensitivity of these measures has been questioned.21 Balance is a motor skill of clinical relevance, as balance deficits may result in multiple episodes of recurrent LAS and diminished lower extremity function.22–24 In order to maintain postural control, the body is in a state of continuous movement, adjusting to keep the center of gravity over the base of support.13 Balance is maintained by strategies at the hip, knee, and ankle and may be disturbed when joint positions cannot be properly sensed or when corrective movements are not executed in a coordinated fashion.25 Sensory information obtained from the somatosensory, visual, and vestibular systems is interpreted in the central nervous system, and appropriate signals are relayed to the muscles of the trunk and extremities in order to maintain postural stability.26,27 Maintenance of postural control also requires factors such as preprogrammed reactions, nerve-conduction velocity, joint range of motion, and muscle strength.28
To evaluate proprioceptive and neuromuscular deficits after lower extremity injury, postural control has typically been assessed with variations of the Romberg test. Instrumented devices such as forceplates have often been used to quantify postural control during variations of quiet standing.25,28 A criticism of static balance testing is that these assessment techniques may not be sensitive enough to detect motor-control deficits related to impaired functional activity and sport performance.21 The task of maintaining posture during quiet standing may not place adequate demands on the postural-control system to detect deficits stemming from ankle-joint injury. In addition, due to the space and cost requirements associated with these instrumented devices, they are not affordable or practical for many clinical settings. Thus, a simple, reliable, and valid method of lower extremity functional performance is needed.29 The Star Excursion Balance Tests (SEBTs) may offer a simple, reliable, low-cost alternative to more sophisticated instrumented methods that are currently available.30–32 The SEBTs are tests of dynamic stability that may provide a more accurate assessment of lower extremity function than tests involving only quiet standing.
The goal of the SEBTs is to reach as far as possible with one leg in each of 8 prescribed directions while maintaining balance on the contralateral leg (Figure 1). The stance leg requires ankle-dorsiflexion, knee-flexion, and hip-flexion range of motion and adequate strength, proprioception, and neuromuscular control to perform these reaching tasks. The SEBTs are best described as functional tests that quantify lower extremity reach while challenging an individual's limits of stability. The reliability of the SEBTs has been investigated in 2 previous studies.31,32 While measures from the SEBTs are reliable, the ability of this tool to detect impairments between healthy and injured subjects has yet to be determined. Therefore, our purpose was to determine if the SEBTs could detect reach deficits in subjects with unilateral CAI.
Figure 1.

A subject performing the posteromedial-reach component of the Star Excursion Balance Tests.
METHODS
Subjects
Twenty subjects with unilateral CAI (10 men, 10 women; age = 19.8 ± 1.4 years; height = 176.8 ± 4.5 cm; mass = 82.9 ± 21.2 kg; leg length = 93.3 ± 7.1 cm) and 20 uninjured subjects (10 men, 10 women; age = 20.2 ± 1.4 years; height = 178.7 ± 4.1 cm; mass = 82.7 ± 19.9 kg; leg length = 95.5 ± 5.2 cm) were recruited from the general athletic population at an NCAA Division III university. Chronic ankle instability was operationally defined for this study as recurrent episodes of ankle instability (“giving way”), regardless of the existence of neuromuscular deficits or pathologic laxity. Volunteers were selected for the CAI group according to the following criteria: (1) at least one episode of an acute LAS but none within the past 6 weeks, (2) multiple episodes of the ankle giving way within the past 12 months, (3) free of cerebral concussions, vestibular disorders, and lower extremity injuries for 3 months before testing, (4) no ear infection, upper respiratory infection, or head cold at the time of the study, and (5) no prior balance training.
Volunteers were selected for the uninjured group according to the following criteria: (1) no history of injury to either ankle, (2) free of cerebral concussions, vestibular disorders, and lower extremity injuries for 3 months before testing, (3) no ear infection, upper respiratory infection, or head cold at the time of the study, and (4) no prior balance training. Subjects with CAI were matched with controls according to sex, sport, and position.
All subjects read and signed an informed consent form approved by the university's institutional review board, which also approved the study. All subjects completed a medical history questionnaire concerning previous ankle injuries and the other inclusion and exclusion criteria.
Procedure
The SEBTs are functional tests that incorporate a single-leg stance on one leg with maximum reach of the opposite leg. The SEBTs are performed with the subject standing at the center of a grid placed on the floor, with 8 lines extending at 45° increments from the center of the grid. The 8 lines positioned on the grid are labeled according to the direction of excursion relative to the stance leg: anterolateral (AL), anterior (A), anteromedial (AM), medial (M), posteromedial (PM), posterior (P), posterolateral (PL), and lateral (L) (Figure 2). The grid was constructed in an athletic training facility using a protractor and 3-in (7.62-cm)-wide adhesive tape and was enclosed in a 182.9-cm by 182.9-cm square on the hard tile floor.
Figure 2.

The 8 directions of the Star Excursion Balance Tests are based on the stance limb.
A verbal and visual demonstration of the testing procedure was given to each subject by the examiner (L.C.O.). Each subject performed 6 practice trials in each of the 8 directions for each leg to become familiar with the task, as recommended by Hertel et al.32 After the practice trials, subjects rode a stationary bike for 5 minutes at a self-selected pace and then stretched the quadriceps, hamstrings, and triceps surae muscle groups before testing. To perform the SEBTs, the subject maintained a single-leg stance while reaching with the contralateral leg (reach leg) as far as possible along the appropriate vector. The subject lightly touched the furthest point possible on the line with the most distal part of the reach foot. The subject was instructed to touch the furthest point on the line with the reach foot as lightly as possible in order to ensure that stability was achieved through adequate neuromuscular control of the stance leg. The subject then returned to a bilateral stance while maintaining equilibrium. The examiner manually measured the distance from the center of the grid to the touch point with a tape measure in centimeters. Measurements were taken after each reach by the same examiner.
Three reaches in each direction were recorded. Subjects were given 15 seconds of rest between reaches. The average of the 3 reaches for each leg in each of the 8 directions was calculated. Reach leg (right, left), order of excursions performed (clockwise, counterclockwise), and direction of the first excursion (A, M, L, P) were counterbalanced to control for any learning or order effect. All trials were then performed in sequential order in either the counterclockwise or clockwise directions.
Trials were discarded and repeated if the subject (1) did not touch the line with the reach foot while maintaining weight bearing on the stance leg, (2) lifted the stance foot from the center grid, (3) lost balance at any point in the trial, or (4) did not maintain start and return positions for one full second. If a subject was judged by the examiner to have touched down with the reach foot in a manner that caused the reach leg to considerably support the body, the trial was discarded and repeated. In other words, if the reach foot was used to widen the base of support, the trial was not recorded. The base of support was the stance foot for the entire trial with the fraction of a second in which the reach foot very lightly touched the ground. It was atypical for subjects to have discarded trials, and none reported fatigue during or after the testing session.
Statistical Analysis
We used a 2 × 2 × 8 repeated-measures analysis of variance for analysis. The between-subjects factor was group with 2 levels (CAI, control), while the within-subjects factors were side with 2 levels (injured, uninjured) and direction with 8 levels (AL, A, AM, M, PM, P, PL, L). Tukey post hoc tests were performed to identify specific differences when significant interactions and main effects were demonstrated. We used the mean of the 3 reaches for each direction and leg for data analysis. The alpha level was set at P < .05 for all analyses.
RESULTS
We identified a significant side-by-group interaction (F1,38 = 3.99, P = .05) (Figure 3). Post hoc comparisons revealed an overall decreased reach in the CAI group while balancing on the injured side compared with the matched side of the uninjured group (78.6 cm versus 82.8 cm) and when compared with their own uninjured side (78.6 cm versus 81.2 cm). The Table lists the means and standard deviations for the 8 specific reach distances for both limbs of the groups.
Figure 3.

Significant differences (P < .05) were found between the injured- and uninjured-limb reaches of the chronic ankle instability (CAI) group (#) and the injured-limb reaches of the CAI and the matched side of the control group (*).
Table 1.
Reach Distances in Each Direction*
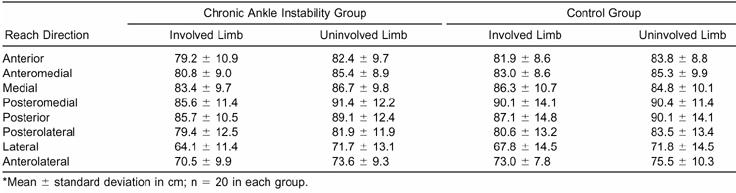
Significant differences in reach distance were found among the 8 directions when data from both limbs of both groups were pooled (F1,19 = 90.8, P = .001) (Figure 4). Post hoc testing revealed that reaches in the L direction were significantly shorter than reaches in the other 7 directions, and reaches in the AL direction were significantly less than all other directions except for L. Additionally, P and PM reaches were significantly longer than reaches in the A, AM, and PL directions.
Figure 4.

The main effect for direction was significant (P < .05), indicating significant differences among the various directions when the data from both groups and both sides were pooled. Reaches in the lateral direction were significantly shorter than reaches in the other 7 directions (*), and reaches in the anterolateral direction were significantly less than all directions except lateral (#). Additionally, posterior and posteromedial reaches were significantly longer than reaches in the anterior, anteromedial, and posterolateral directions (;p0). A indicates anterior; AM, anteromedial; M, medial; PM, posteromedial; P, posterior; PL, posterolateral; L, lateral; and AL, anterolateral.
DISCUSSION
The principal finding of our study was that subjects with CAI reached significantly less when standing on their injured limb compared with their uninjured limb and when compared with uninjured subjects. While previous investigators31–32 have estimated the reliability of the SEBTs, we focused on the ability of these tests to detect impairments in lower extremity reach in subjects with CAI. The SEBTs appear to be sensitive in detecting reach deficits both between and within athletes with unilateral CAI. While the SEBTs appear to have the sensitivity to detect reach deficits in subjects with CAI, their validity has yet to be clearly established. This is a difficult challenge, as no dynamic functional test is considered a gold standard for validation of the SEBTs. Evidence supporting the use of specific functional tests in discriminating between individuals with and without CAI is lacking. Previous researchers33,34 have investigated various hopping tasks but were unable to identify performance deficits between subjects with and without CAI. It is our belief that the SEBTs are the first noninstrumented, functional tests that have been shown to be both highly reliable and sensitive to deficits between subjects with and without CAI.
Assessment of postural control during quiet standing in subjects with a history of ankle sprain has been frequently reported, but the methods used have been inconsistent. Therefore, generalizations about previously reported findings must be made with caution. Some researchers have used objective assessment (derivatives of center-of-pressure measures), while others have used subjective assessment (subject and examiner ratings of apparent stability). Some35–37 have reported no side-to-side differences among ankle-injured subjects; others9,16,18,38,39 have identified such differences. Differences between groups of ankle-injured and uninjured subjects were reported in 2 studies,15,36 but other studies35,37 showed no group differences. It may be that static assessment of postural control does not provide sufficient challenge to consistently detect functional deficits in subjects after LAS.21 Ross et al40–42 have presented preliminary results of dynamic postural-control deficits in those with CAI by measuring time to stabilization after jump landings on a single limb. While these methods hold promise as a means to quantify functional performance deficits in athletes with CAI, more research in this area is needed.
Dynamic assessment, such as time-to-stabilization measures or the SEBTs, may be better than static postural-control assessment to determine functional deficits in those with CAI. The differences between static postural-control tests and the SEBTs must be considered. Static postural control is the ability to remain as still as possible while maintaining one's balance over a stable base of support. Static postural impairment with CAI is thought to be caused by impaired proprioception and neuromuscular control.9,16,17 When ligaments are torn, articular receptors may be damaged and contribute to the observed postural deficits.9,12,27 Maintenance of balance during dynamic movements, such as those involved in performing the SEBTs, involves the ability to keep the center of gravity over the stable base of support without losing one's balance.25 Dynamic postural stability has been defined as the extent to which a person can lean or reach without moving the feet and still maintain balance.43 We believe that performance of the SEBTs challenges the subject's limits of stability as he or she maximally reaches and is, thus, at least somewhat indicative of dynamic postural stability. Although dynamic postural impairment may be influenced by impaired proprioception and neuromuscular control, other factors may contribute to this condition, including strength and range of motion.
First, strength demands are most likely greater when performing dynamic tasks compared with static tasks. Closed kinetic chain motion at the ankle, knee, and hip must be adequately controlled by the lower extremity musculature in order to execute the SEBTs. Conversely, maintaining single-leg stance while standing on a stable platform places relatively small strength demands on the lower extremity musculature. Second, range-of-motion requirements are greater when performing dynamic tasks such as the SEBTs compared with quiet standing tasks. Maintaining single-leg stance while performing maximum reach with the opposite leg requires the stance leg to have sufficient ankle, knee, and hip motion. After LAS, joint injury resulting in decreased motion in the subtalar or talocrural joint may affect performance on the SEBTs. Finally, subject apprehension may be the most critical performance-inhibiting factor. After LAS, subjects may be more hesitant to perform a dynamic task that requires them to challenge their limits of stability. Several of our subjects with CAI reported feelings of apprehension when performing reaches while balancing on their injured limbs. In a balance task during quiet standing, apprehension may be substantially less because a subject's limits of stability are rarely challenged.
Incorporation of the SEBTs into the clinical assessment of patients with CAI requires an understanding of issues related to measurement reliability and learning effects. Kinzey and Armstrong31 reported intrasession reliability estimates (intraclass correlation coefficient [ICC] 2,1) between 0.67 and 0.87 for the SEBTs and recommended the performance of several practice trials before recording baseline values because of the motor learning associated with this novel task. As subjects in this study were not allowed to touch down with the foot at the point of maximum reach, the examiner was forced to estimate a point on the floor corresponding to maximum reach distance. This may have influenced the ICC values. Hertel et al32 slightly adjusted the procedures for these tests by allowing subjects a very brief touch down with the reach foot at the point of maximum reach. On a second day of testing, estimates of intratester and intertester reliability (ICC 2,1) for the different reach directions ranged from 0.82 to 0.96 and 0.81 to 0.93, respectively. They suggested that at least 6 practice trials on each limb be allowed before any baseline values are recorded.32
A secondary finding of our study was that reach distances varied substantially across the different directions in both limbs of the 2 groups. We chose to include reach direction in our statistical model because we were interested in identifying whether injured subjects reached significantly less than uninjured subjects in any of the specific directions. In fact, reach differences in the different directions were consistent across both limbs of the injured and uninjured groups. This suggests that the 8 directions of the SEBTs may be best used as a battery of tests to identify reach distances among groups.
A potential criticism of this study is that we chose not to exclude subjects who had mechanical instability from our CAI group. In the sports medicine literature, separating individuals with CAI into categories of either mechanical instability or functional instability is a longstanding tradition6,9,24,35,37; however, empirical evidence to support this somewhat arbitrary dichotomy is lacking. An individual who possesses repetitive bouts of ankle instability (giving way) has neuromuscular deficits (the principal criterion for functional instability) regardless of the presence or absence of pathologic laxity (the principal criterion for mechanical instability). As the SEBTs are an assessment of lower extremity reach and functional performance, we chose not to assess subjects for mechanical instability. Because there is no satisfactory evidence to suggest why subjects with mechanical instability would perform differently than subjects without mechanical instability on tests such as the SEBTs, we chose not to exclude subjects with mechanical instability.
A second potential criticism of this study is the possible role of subject height in influencing the reach distances of subjects. Preliminary data suggest that height and leg length are both statistically significant predictors of reach distances on the SEBTs.44 While we did not normalize reach distances to height or leg length in our study, we did match injured and healthy subjects for height as closely as possible. Independent t tests revealed no significant difference in height (P = .58) or leg length (P = .28) between injured and uninjured subjects.
CONCLUSIONS
The SEBTs appear to be a promising means of identifying functional deficits in subjects with CAI via measures of lower extremity reach. Given the dynamic nature of this assessment and the limited equipment needed, the SEBTs hold potential as a cost-effective tool for assessing functional deficits in a variety of lower extremity conditions. Future research should examine the validity of the tests in different injured populations, such as those with anterior cruciate ligament deficiency and patellofemoral pain syndrome. Also, comparing performance of static postural-control tasks on a forceplate with performance on the SEBTs would allow investigation of the correlation between increased postural-control scores and decreased reach distance. Thirdly, using the tests to determine if lower extremity reach improves with rehabilitation would be beneficial. Finally, assessing specific range-of-motion deficits with kinematic measures would provide insight into the movement strategies and sources of impairment resulting in decreased SEBTs performance in specific populations.
REFERENCES
- Jackson D W, Ashley R L, Powell J W. Ankle sprains in your athletes: relation of severity and disability. Clin Orthop. 1974;101:201–215. [PubMed] [Google Scholar]
- Brand R L, Black H M, Cox J S. The natural history of the inadequately treated ankle sprain. Am J Sports Med. 1977;5:248–249. doi: 10.1177/036354657700500609. [DOI] [PubMed] [Google Scholar]
- Garrick J G. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains. Am J Sports Med. 1977;5:241–242. doi: 10.1177/036354657700500606. [DOI] [PubMed] [Google Scholar]
- Balduini F C, Tetzlaff J. Historical perspectives on injuries of the ligaments of the ankle. Clin Sports Med. 1992;1:3–12. [PubMed] [Google Scholar]
- Han K H, Muwanga C L. The incidence of recurrent soft tissue ankle injuries. Br J Clin Pract. 1990;44:609–611. [PubMed] [Google Scholar]
- Freeman M AR. Instability of the foot after injuries to the lateral ligament of the ankle. J Bone Joint Surg Br. 1965;47:678–685. [PubMed] [Google Scholar]
- Staples O S. Result study of ruptures of lateral ligaments of the ankle. Clin Orthop. 1972;85:50–58. doi: 10.1097/00003086-197206000-00011. [DOI] [PubMed] [Google Scholar]
- Bosien W R, Staples O S, Russell S W. Residual disability following acute ankle sprains. J Bone Joint Surg Am. 1955;37:1237–1243. [PubMed] [Google Scholar]
- Freeman M AR, Dean M RE, Hanham I WF. The etiology and prevention of functional instability of the foot. J Bone Joint Surg Br. 1965;47:678–685. [PubMed] [Google Scholar]
- Freeman M AR, Wyke B D. Articular reflexes at the ankle joint: an electromyographic study of normal and abnormal influences of ankle-joint mechanoreceptors upon reflex activity in the leg muscles. Br J Surg. 1967;54:990–1001. doi: 10.1002/bjs.1800541204. [DOI] [PubMed] [Google Scholar]
- Tropp H, Ekstrand J, Gillquist J. Stabilometry in functional instability of the ankle and its value in predicting injury. Med Sci Sports Exerc. 1984;16:64–66. [PubMed] [Google Scholar]
- Michelson J D, Hutchins C. Mechanoreceptors in human ankle ligaments. J Bone Joint Surg Br. 1995;77:219–224. [PubMed] [Google Scholar]
- Nashner L M. Practical biomechanics and physiology of balance. In: Jacobson G P, Newman C W, Kartush J M, editors. Handbook of Balance Function Testing. Mosby-Year Book Inc; Chicago, IL: 1993. pp. 261–279. [Google Scholar]
- Hertel J. Functional instability following lateral ankle sprain. Sports Med. 2000;29:361–371. doi: 10.2165/00007256-200029050-00005. [DOI] [PubMed] [Google Scholar]
- Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med. 1985;13:259–262. doi: 10.1177/036354658501300408. [DOI] [PubMed] [Google Scholar]
- Garn S N, Newton R A. Kinesthetic awareness in subjects with multiple ankle sprains. Phys Ther. 1988;68:1667–1671. doi: 10.1093/ptj/68.11.1667. [DOI] [PubMed] [Google Scholar]
- Tropp H, Odenrick P. Postural control in single-limb stance. J Orthop Res. 1988;6:833–839. doi: 10.1002/jor.1100060607. [DOI] [PubMed] [Google Scholar]
- Lentell G L, Katzmann L L, Walters M R. The relationship between muscle function and ankle instability. J Orthop Sports Phys Ther. 1990;11:605–611. doi: 10.2519/jospt.1990.11.12.605. [DOI] [PubMed] [Google Scholar]
- Pinstaar A, Brynhildsen J, Tropp H. Postural corrections after standardised perturbations of single leg stance: effect of training and orthotic devices in patients with ankle instability. Br J Sports Med. 1996;30:151–155. doi: 10.1136/bjsm.30.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isakov E, Mizrahi J. Is balance impaired by recurrent sprained ankle? Br J Sports Med. 1997;31:65–67. doi: 10.1136/bjsm.31.1.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holme E, Magnusson S P, Becher K, Bieler T, Aagaard P, Kjaer M. The effect of supervised rehabilitation on strength, postural sway, position sense and re-injury risk after acute ankle ligament sprain. Scan J Med Sci Sports. 1999;9:104–109. doi: 10.1111/j.1600-0838.1999.tb00217.x. [DOI] [PubMed] [Google Scholar]
- Harrington K D. Degenerative arthritis of the ankle secondary to long-standing lateral ligament instability. J Bone Joint Surg Am. 1979;61:354–361. [PubMed] [Google Scholar]
- Irrgang J J, Whitney S L, Cox E D. Balance and proprioceptive training for rehabilitation of the lower extremity. J Sport Rehabil. 1994;3:68–83. [Google Scholar]
- Bernier J N, Perrin D H. Effect of coordination training on proprioception of the functionally unstable ankle. J Orthop Sports Phys Ther. 1998;27:264–275. doi: 10.2519/jospt.1998.27.4.264. [DOI] [PubMed] [Google Scholar]
- Guskiewicz K M, Perrin D H. Research and clinical applications of assessing balance. J Sport Rehabil. 1996;5:45–63. [Google Scholar]
- Nashner L M, Black F O, Wall C., III Adaptation to altered support and visual conditions during stance: patients with vestibular deficits. J Neurosci. 1982;2:536–544. doi: 10.1523/JNEUROSCI.02-05-00536.1982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shumway-Cook A, Horak F B. Assessing the influence of sensory interaction of balance: suggestion from the field. Phys Ther. 1986;66:1548–1550. doi: 10.1093/ptj/66.10.1548. [DOI] [PubMed] [Google Scholar]
- Palmieri R M, Ingersoll C D, Stone M B, Krause B A. Center-of-pressure parameters used in the assessment of postural control. J Sport Rehabil. 2002;11:51–66. [Google Scholar]
- Cohen H, Blatchly C A, Gombash L L. A study of the clinical test of sensory interaction and balance. Phys Ther. 1993;73:346–354. doi: 10.1093/ptj/73.6.346. [DOI] [PubMed] [Google Scholar]
- Gray G W. Wynn Marketing Inc; Adrian, MI: 1995. Lower Extremity Functional Profile. [Google Scholar]
- Kinzey S J, Armstrong C W. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther. 1998;27:356–360. doi: 10.2519/jospt.1998.27.5.356. [DOI] [PubMed] [Google Scholar]
- Hertel J, Miller S J, Denegar C R. Intratester and intertester reliability during the Star Excursion Balance Tests. J Sport Rehabil. 2000;9:104–116. [Google Scholar]
- Worrell T W, Booher L D, Hench K M. Closed kinetic chain assessment following inversion ankle sprain. J Sport Rehabil. 1994;3:197–203. [Google Scholar]
- Munn J, Beard D J, Refshauge K M, Lee R W. Do functional-performance tests detect impairment in subjects with ankle instability? J Sport Rehabil. 2002;11:40–50. [Google Scholar]
- Tropp H, Ekstrand J, Gillquist J. Factors affecting stabilometry recordings of single limb stance. Am J Sports Med. 1984;12:185–188. doi: 10.1177/036354658401200302. [DOI] [PubMed] [Google Scholar]
- Tropp H. Pronator weakness in functional instability of the ankle joint. Int J Sports Med. 1986;7:291–194. doi: 10.1055/s-2008-1025777. [DOI] [PubMed] [Google Scholar]
- Bernier J N, Perrin D H, Rijke A. Effect of unilateral functional instability of the ankle on postural sway and inversion and eversion strength. J Athl Train. 1997;32:226–232. [PMC free article] [PubMed] [Google Scholar]
- Friden T, Zatterstrom R, Lindstrand A, Moritz U. A stabilometric technique for evaluation of lower limb instabilities. Am J Sports Med. 1989;17:118–122. doi: 10.1177/036354658901700120. [DOI] [PubMed] [Google Scholar]
- Orteza L C, Vogelbach W D, Denegar C R. The effect of molded and unmolded orthotics on balance and pain while jogging following inversion ankle sprain. J Athl Train. 1992;27:80–84. [PMC free article] [PubMed] [Google Scholar]
- Ross S E, Guskiewicz K M, Yu B. Comparison of time to stabilization measures in functionally unstable versus stable ankles [abstract] J Athl Train. 2001;36(suppl):S-76. [Google Scholar]
- Ross S E, Guskiewicz K M, Yu B, Garrett W E. Landing pattern difference between functionally stable and unstable ankles [abstract] Med Sci Sports Exerc. 2002;34(suppl):173. [Google Scholar]
- Ross S E, Guskiewicz K M, Yu B. Time to stabilization differences in functionally unstable and stable ankles [abstract] J Athl Train. 2002;37(suppl):S-22. [Google Scholar]
- Goldie P A, Bach T M, Evans O M. Force platform measures for evaluating postural control: reliability and validity. Arch Phys Med Rehabil. 1989;70:510–517. [PubMed] [Google Scholar]
- Gribble P A, Hertel J, Piegaro A B. Consideration for normalization of measures of the Star Excursion Balance Tests. Measure Phys Educ Exer Sci. (in press)