

Abstract
Objective: To investigate the tendency of undergraduate athletic training students to think critically, to assess their likelihood of using specific components of critical thinking, and to study the effect of selected demographic and educational variables on critical-thinking tendencies in this sample of students.
Design and Setting: Data were collected before regularly scheduled athletic training classes at the beginning of the spring semester.
Subjects: Ninety-one students enrolled in 3 Commission on Accreditation of Allied Health Education Programs-accredited undergraduate athletic training education programs in the southeast. The subjects ranged in age from 19 to 29 years (mean age = 22.33 ± 1.94). Forty-six (50.5%) of the subjects were men and 45 (49.5%) were women.
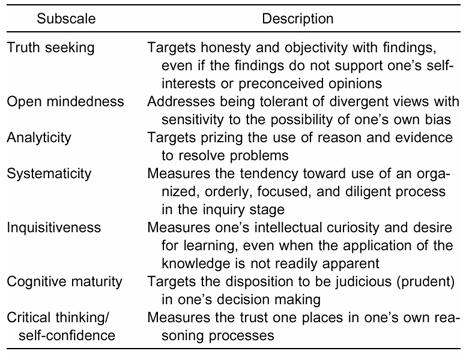
Measurements: The California Critical Thinking Disposition Inventory contains 75 Likert-type items assessing 7 components of critical thinking: truth seeking, open mindedness, analyticity, systematicity, inquisitiveness, cognitive maturity, and critical-thinking self-confidence.
Results: The overall mean indicated a general but mild trend toward critical thinking, with weak scores on the truth-seeking subscale. One-way analysis of variance reflected significant differences among the schools for truth seeking, open mindedness, and maturity subscales and for the overall mean score for the entire inventory. Only the open-mindedness difference persisted between 2 of the schools after post hoc testing. Correlation analyses indicated no significant relationship between total score and age, sex, ethnicity, year in athletic training program, cumulative grade point average, completed semester hours, or clinical-experience hours.
Conclusions: Athletic training students are inclined toward critical thinking, but this tendency is relatively weak. Classroom and clinical instructors should use teaching methods and techniques that facilitate the components of critical thinking. The promotion of critical thinking and critical-thinking skills has implications for athletic training education and the advancement of certified athletic trainers and the profession of athletic training.
Keywords: California Critical Thinking Disposition Inventory, metacognition, education
The concept of critical thinking has been a concern related to the development of society since the time of the Greek philosophers thousands of years ago. John Dewey brought critical thinking to the attention of educators in 1916,1 and it has been a focal point in higher education for the past 2 decades. The National Education Goals Panel advocated critical thinking and effective communication and problem-solving abilities as indicators of success in higher education,2 and the United States Congress included significant improvement in the critical-thinking skills of all college graduates in the Goals 2000: National Goals for Education Act.3 Critical thinking was also delineated as an outcome measure for the accreditation of baccalaureate and graduate degree programs in nursing.4 Understandably, this inclusion resulted in multiple studies of critical thinking in baccalaureate and certificate programs in nursing.5–21 Critical thinking has also been investigated in athletic training,22 dentistry,23 medicine,24,25 pharmacy,26 and respiratory therapy.27
Several factors have confounded the recent attention to critical thinking. Chief among these has been the lack of a consistent operational definition of critical thinking. Critical thinking has been defined as reflective and reasonable thinking that is focused on deciding what to believe or do28; thinking about your thinking while you are thinking in order to make your thinking better29; and the process of purposeful, self-regulatory judgment that gives reasoned consideration to evidence, contexts, conceptualization, methods, and criteria.30 Based on its consensus definition of critical thinking, the American Philosophical Association30 characterized the ideal critical thinker as being habitually inquisitive, well-informed, trustful of reason, open minded, flexible, fair minded in evaluation, honest in facing personal biases, prudent in making judgments, willing to reconsider, clear about issues, orderly in complex matters, diligent in seeking relevant information, reasonable in the selection of criteria, focused in inquiry, and persistent in seeking results that are as precise as the subject and the circumstances of inquiry permit.
This definition implies the presence of a “critical spirit”31 that disposes one to critical thinking. Facione et al32 described the disposition to critical thinking as the consistent internal motivation to employ one's own critical-thinking abilities in judging what to believe or do in any situation. Simply put, if there is no disposition toward critical thinking, then critical thinking will not take place, regardless of the presence or absence of the necessary skills.
Additionally, preliminary research has not demonstrated a relationship between critical-thinking ability and professional competence.16 This paradox lies in the fact that critical thinking is nonlinear and not synonymous with logical thinking. Many professionals associate critical-thinking ability with the ability to problem solve and arrive at a sound and rational judgment. Purposeful evaluation is crucial in medical and allied medical professions: practitioners must be able to analyze multiple pieces of information and render sound decisions regarding clinical care on a consistent and repetitive basis. However, a clinician can follow a prescribed template, conduct an efficient and orderly evaluation, and arrive at a workable solution without ever thinking critically. This clinician is competent, but the barrier that keeps him or her from success and expert status is the key critical-thinking component of reflection. The truly outstanding clinician follows the same template, analyzes the same pieces of information, and then compares the data with previous experience before forming a decision. This clinician has the ability to generate alternative theories or solutions to solve a particular problem, which distinguishes him or her from a merely competent peer.
While critical thinking has direct implications for the quality of patient care, it also influences individual growth and professional-development decision processes. Athletic training is characterized by the need for flexibility, creativity, and the capacity to “think on the go.” These qualities are even more important in the current health care and economic climates, when the ability to create novel solutions, readily adapt to new situations, and integrate multiple tasks is paramount. Certified athletic trainers (ATCs) who are competent and disposed toward critical thinking will thrive and advance in today's uncertain workplace environments. By promoting the disposition toward critical thinking and teaching critical-thinking skills, athletic training educators will help prepare ATCs who are optimally positioned for career success.
The purposes of our study were to use the California Critical Thinking Disposition Inventory (CCDTI)33 to investigate the tendency of undergraduate athletic training students to think critically and to assess their likelihood of using specific components of critical thinking. We also studied the effect of selected demographic and educational variables on critical-thinking tendencies.
METHODS
The California Critical Thinking Disposition Inventory
The CCTDI is composed of 75 Likert-type items scored on a 6-point scale anchored by “agree strongly” and “disagree strongly.” The items measure 7 aspects of critical thinking: truth seeking, open mindedness, analyticity, systematicity, inquisitiveness, cognitive maturity, and critical-thinking self-confidence (Table 1). A subscale score of 30 or less indicates consistent opposition to the characteristic or attribute represented by that subscale, while scores between 40 and 50 suggest progressive strength. Within this range, scores closer to 40 reflect some ambivalence, while scores closer to 50 indicate affirmation of the corresponding trait. A subscale score over 50 reflects a strong tendency toward that dimension. The possible overall score ranges from 70 to 420, with a total score of 280 to 349 indicating a general disposition for critical thinking.33 Reliability of the overall instrument (Cronbach α = .92) and the subscales (Cronbach α = .60 to .78) was established in an administration of the CCTDI to 1019 college freshmen.31 The internal consistency for our total sample was .72. For psychological tests, a Cronbach alpha level greater than .60 indicates an acceptable level of reliability.34
Table 1. California Critical Thinking Disposition Inventory Subscale Descriptions
Subjects
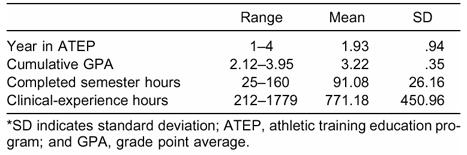
Ninety-one students (mean age = 22.33 ± 1.94 years) enrolled in 3 Commission on Accreditation of Allied Health Education Programs (CAAHEP)-accredited undergraduate athletic training education programs in the southeast served as subjects. All of the schools were public; 2 were comprehensive universities, and 1 was a regional university. Forty-six (50.5%) of the subjects were men and 45 (49.5%) were women. Eighty percent (n = 73) of the subjects were white, 14.3% (n = 13) were black, and the remaining 5.5 % (n = 5) identified themselves as American Indian, Asian/Pacific Islander, Hispanic, or other. The subjects completed an information sheet that included items on total credit hours, grade point average, and other relevant variables (Table 2).
Table 2. Subject Demographic Information*
Inventory Administration
We administered the CCTDI to the subjects before a regularly scheduled athletic training class at the start of the spring semester. The subjects also completed a demographic information sheet and provided informed consent before the testing session began. The institutional review boards of all participating institutions approved this study.
Data Analysis
We scored each subject's inventory by hand and calculated descriptive statistics for each school using SPSS (version 8.0, SPSS Inc, Chicago, IL). Using one-way analysis of variance (ANOVA), we assessed differences within the mean subscale scores and mean total scores for the 3 schools. We used Scheffé post hoc analyses to investigate differences indicated by the ANOVA and further refined the results by employing the SPSS feature of automatically grouping the variables by means into homogeneous subsets after the post hoc tests. Pearson and Spearman rho correlation analyses were used to assess the relationship between the continuous and categoric demographic variables and CCTDI total score, respectively. We set the a priori alpha level at P = .05 for all analyses.
RESULTS
The mean scores for each subscale ranged from the low- to mid-40s, except for truth seeking, which scored 35.10 (Table 3). The mean total score for this sample was 293 ± 26.05, with a range from 229 to 356. Although this score is within the range indicating a disposition toward critical thinking, it falls close to the lower limits, indicating that the disposition is weak.
Table 3. Mean California Critical Thinking Disposition Inventory Scores*
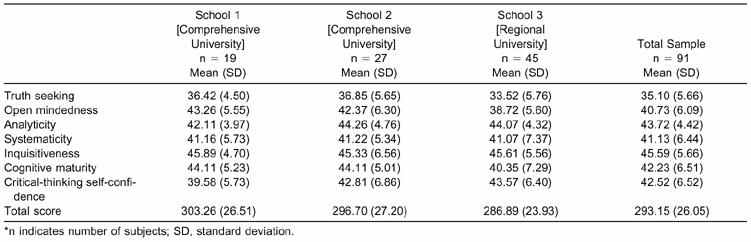
One-way ANOVA indicated significant differences between the schools for the truth seeking (F2,89 = 3.818, P = .026), open mindedness (F2,89 = 5.655, P = .005), and maturity (F2,89 = 4.098, P = .020) subscales and for total score (F2,89 = 3.154, P = .048). Only the open-mindedness subscale difference persisted after post hoc tests, with subjects from one of the comprehensive institutions scoring significantly higher than those from the regional university. Correlation analyses indicated no significant relationship between the demographic variables and the total score.
DISCUSSION
Components of Critical-Thinking Disposition
We were disappointed but not surprised that our sample had weak truth-seeking scores. This finding is consistent with other studies of nursing,10,14,15 general college,32,35 and community college students36 using the CCTDI. Like most allied medical and medical professions, competencies and facts drive the educational process for athletic training. Students are then tested on these facts and, thus, are often primarily concerned with knowing the right answer. Knowing why the answer is correct and knowing equally correct alternative responses are not often considered. This type of atmosphere can stifle the desire for the best knowledge that is characteristic of truth seeking, as the student often becomes a passive learner who is not encouraged to exchange ideas or pursue parallel lines of discussion.10
Our subjects' other subscale scores and total scores were similar to those of a sample of 100 senior nursing students studied by Colucciello10 but much higher than those reported by Ip et al,14 who administered the CCTDI to 125 Chinese nursing undergraduates. This disparity most likely lies in the educational atmosphere in China, where the educational system is authoritarian and learners are expected to conform and passively absorb knowledge.
The literature does not include between-school comparisons using the CCTDI. Our data do not allow us to explain the differences we observed in the open-mindedness scores between the regional university and one of the comprehensive universities. However, we believe that this difference is not specific to the athletic training students or the athletic training education programs at these 2 schools. Rather, we believe that it reflects a difference in the general characteristics of these types of universities and the attributes of the students who attend them. Generally, students at larger universities interact with a more diverse segment of the population and encounter a broader range of opposing ideas. Exposure to such divergent opinions and varied student backgrounds would tend to attract students who are comfortable in such a setting. This comfort is reinforced and expanded by the exposure itself. As a result, students at larger universities would be expected to have higher open-mindedness scores.
Correlation Analyses
Research has suggested that critical-thinking skills do increase significantly after entry into clinical practice,16 but investigations of enrolled students have been somewhat equivocal. Some evidence suggests that critical-thinking skills increase over time5,17 but most studies12,16,18,21 have found no difference between nursing students at 2 points in their educational programs.
Results from critical-thinking investigations have been similar. Leppa15 administered the CCTDI to students in the first and fourth quarters of an undergraduate nursing program and found significant increases in total score. Colucciello10 and Ip et al14 reported increases in CCTDI scores from the sophomore to junior years of baccalaureate nursing programs, but significant decreases were seen from the junior to senior year14 and during both years.10 Differences in study design may account for these incongruent findings. Leppa15 conducted test-retest investigations on the same students at 2 points in their educational program, while the other research10,14 was cross-sectional in nature. Our finding of no correlation between year in program or total credit hours and subscale and total score is supported by Facione et al,32,35 who suggested that increases in subscale scores and total score are possible but that overall disposition toward critical thinking appears to be stable over a period of years.
The lack of a relationship between sex, age, and race and critical-thinking disposition is consistent with the literature. Facione et al37 found no difference in total dispositional score between the sexes in their study of general college students, while Ip et al14 found no relationship between nursing students' mean total score or subscale scores and sex or work experience. These findings all further reinforce the concept that critical-thinking disposition is a trait that does not depend on general personal characteristics.
The reflective component of critical thinking requires the existence of some body of experience to consider and reflect upon in the decision-making process. This concept is supported by Goodfellow,27 who reported that years of clinical experience were associated with self-perceived increases in critical-thinking ability among practicing respiratory therapists. Therefore, initially, we were somewhat surprised that there was no correlation between critical-thinking disposition and clinical-experience hours. Aside from the obvious differences in types of measurement and samples between our study and Goodfellow's27 work, we speculate that our findings are also explained by the concept of quality versus quantity. The accumulation of a large number of clinical hours does not guarantee the accumulation of valuable experience, clinical competence, or the use of critical thinking during that time. Indeed, this disparity may be one driving force behind the transition to competency-based education in the allied medical and medical professions.
Previous research using the CCTDI in nursing students14 has indicated significant correlations between grade point average (GPA) and mean total score and the mean scores for the open-mindedness, analyticity, systematicity, inquisitiveness, self-confidence, and cognitive maturity subscales. The disparity between our findings and these results could be related to the method used by Ip et al14 to calculate GPA. Their process was based on an honors grading system and differed from the system used by American universities. Other research7 involving nursing students has found no relationship between critical-thinking skill and GPA.
Recommendations for the Educator
Promoting Truth Seeking. Truth seeking incorporates the concept of intellectual courage: the student desires the best knowledge even if such knowledge fails to support or undermines his or her own beliefs, preconceptions, or self-interests. Facilitating this attribute requires an instructor who is also willing to seek the truth. Truth seeking demands self-examination on the instructor's part and the willingness to discuss instances when he or she was challenged by information that was inconsistent with values or previous knowledge. In these situations, the instructor should also provide information about strategies used to reconcile such inconsistencies. Thinking aloud and talking students through decision-making processes are helpful in this regard. Finally, both classroom and clinical instructors can improve truth seeking by using the Socratic method of teaching with open-ended questioning techniques and case studies or scenarios specifically designed not to fit into the patterns that would be expected based on readings or class discussions. Many of these techniques require planning and take time, so it is unrealistic to view them as the sole teaching method. However, their consistent, varied, and strategic use throughout the curriculum is beneficial.
Promoting Reflection. Because reflection distinguishes great practitioners from their peers, classroom and clinical instructors should consistently seek to promote student reflection. Journals and directed writings are 2 traditional methods that can force a student to look back on and analyze actions and clinical decisions. Written simulations are also beneficial in forcing the student to draw on previous experience while dealing with a current situation. Oral or written critiques of relevant research can also be helpful in this regard, particularly if the student is required to provide a clear explanation of his or her positions and statements and to apply this information to previous clinical experiences. A final technique for improving reflection is the use of situational learning, in which the student is allowed to make a mistake without compromising the safety of the patient. When the student sees the mistake and then is guided through possible solutions by the clinical instructor, he or she begins to identify patterns that will enable recognition of similar situations in the future. As the student improves, the clinical instructor provides less guidance to the point when the student self-corrects and avoids the mistake altogether.
The athletic training students in our study were disposed to think critically, but these tendencies were weak overall. While critical-thinking ability is not an absolute requirement for minimal professional competence, it is crucial for true quality practice and for maximal professional development. Critical-thinking disposition also has implications for job satisfaction and security. As a result, athletic training educators must strive to develop the disposition for critical thinking in their students. Doing so requires purposeful planning and teaching on the part of classroom and clinical instructors, but the potential outcomes will benefit the profession as a whole.
Clearly, the disposition to think critically does not imply the ability to think critically. Additional investigations are needed to assess the critical-thinking skills of athletic training students and the relationship between critical-thinking skill and critical-thinking disposition among this population. Changes in these measures during the transition from student to entry-level ATC should also be studied. Finally, professional competence does not imply critical-thinking ability, but there is certainly some relationship between clinical judgment and critical thinking. Further research is needed to define these factors and their relationship in the practicing ATC.
REFERENCES
- Dewey J. Democracy and Education. Macmillan; New York, NY: 1916. [Google Scholar]
- Banta T W. Toward a plan for using national assessment to ensure continuous improvement of higher education. J Gen Educ. 1993;42:33–58. [Google Scholar]
- US Congress . Goals 2000: National Goals for Education Act. US Government Printing Office; Washington, DC: 1994. [Google Scholar]
- National League for Nursing . Criteria and Guidelines for the Evaluation of Baccalaureate and Higher Degree Programs in Nursing. National League for Nursing; New York, NY: 1992. Publication #15-2474. [Google Scholar]
- Angel B F, Duffey M, Belyea M. An evidence-based approach for evaluating strategies to improve knowledge acquisition and critical-thinking performance in nursing students. J Nurs Educ. 2000;39:219–228. doi: 10.3928/0148-4834-20000501-07. [DOI] [PubMed] [Google Scholar]
- Behrens P J. The Watson-Glaser Critical Thinking Appraisal and academic performance of diploma school students. J Nurs Educ. 1996;35:34–36. doi: 10.3928/0148-4834-19960101-10. [DOI] [PubMed] [Google Scholar]
- Berger M C. Clinical thinking ability and nursing students. J Nurs Educ. 1984;23:306–308. doi: 10.3928/0148-4834-19840901-10. [DOI] [PubMed] [Google Scholar]
- Bethune E, Jackling N. Critical thinking skills: the role of prior experience. J Adv Nurs. 1997;26:1005–1012. doi: 10.1046/j.1365-2648.1997.00394.x. [DOI] [PubMed] [Google Scholar]
- Brooks K L, Shepherd J M. Professionalism versus general critical thinking abilities of senior nursing students in four types of nursing curricula. J Prof Nurs. 1992;8:87–95. doi: 10.1016/8755-7223(92)90068-a. [DOI] [PubMed] [Google Scholar]
- Colucciello M L. Critical thinking skills and dispositions of baccalaureate nursing students: a conceptual model for evaluation. J Prof Nurs. 1997;13:236–245. doi: 10.1016/s8755-7223(97)80094-4. [DOI] [PubMed] [Google Scholar]
- Colucciello M L. Relationships between critical thinking dispositions and learning styles. J Prof Nurs. 1999;15:294–301. doi: 10.1016/s8755-7223(99)80055-6. [DOI] [PubMed] [Google Scholar]
- Daly W M. The development of an alternative method in the assessment of critical thinking as an outcome of nursing education. J Adv Nurs. 2001;36:120–130. doi: 10.1046/j.1365-2648.2001.01949.x. [DOI] [PubMed] [Google Scholar]
- Perciful E G, Nester P A. The effect of an innovative clinical teaching method on nursing students' knowledge and critical thinking skills. Nurs Educ. 1996;35:23–28. doi: 10.3928/0148-4834-19960101-07. [DOI] [PubMed] [Google Scholar]
- Ip W Y, Lee D T, Lee I F, Chau J P, Wootton Y S, Change A M. Disposition towards critical thinking: a study of Chinese undergraduate nursing students. J Adv Nurs. 2000;32:84–90. doi: 10.1046/j.1365-2648.2000.01417.x. [DOI] [PubMed] [Google Scholar]
- Leppa C J. Standardized measures of critical thinking: experience with the California Critical Thinking Tests. Nurse Educ. 1997;22:29–33. doi: 10.1097/00006223-199709000-00012. [DOI] [PubMed] [Google Scholar]
- Maynard C A. Relationship of critical thinking ability to professional nursing competence. J Nurs Educ. 1996;35:12–18. doi: 10.3928/0148-4834-19960101-05. [DOI] [PubMed] [Google Scholar]
- Pepa C A, Brown J M, Alverson E M. A comparison of critical thinking abilities between accelerated and traditional baccalaureate nursing students. J Nurs Educ. 1997;36:46–48. doi: 10.3928/0148-4834-19970101-10. [DOI] [PubMed] [Google Scholar]
- Saucier B L. Critical thinking skills of baccalaureate nursing students. J Prof Nurs. 1995;11:351–357. doi: 10.1016/s8755-7223(95)80054-9. [DOI] [PubMed] [Google Scholar]
- Sedlak C A. Critical thinking of beginning baccalaureate nursing students during the first clinical nursing course. J Nurs Educ. 1997;36:11–18. doi: 10.3928/0148-4834-19970101-05. [DOI] [PubMed] [Google Scholar]
- Thompson C, Rebeschi L M. Critical thinking skills of baccalaureate nursing students at program entry and exit. Nurs Health Care Perspect. 1999;20:248–252. [PubMed] [Google Scholar]
- Vaughan-Wrobel B C, O'Sullivan P, Smith L. Evaluating critical thinking skills of baccalaureate nursing students. J Nurs Educ. 1997;36:485–488. doi: 10.3928/0148-4834-19971201-09. [DOI] [PubMed] [Google Scholar]
- Fuller D V. Critical thinking in undergraduate athletic training education. J Athl Train. 1997;32:242–247. [PMC free article] [PubMed] [Google Scholar]
- Behar-Horenstein L S, Dolan T A, Courts F J, Mitchell G S. Cultivating critical thinking in the clinical learning environment. J Dent Educ. 2000;64:610–615. [PubMed] [Google Scholar]
- Lieberman S A, Trumble J M, Smith E R. The impact of structured student debates on critical thinking and informatics skills of second-year medical students. Acad Med. 2000;75(10 suppl):84–86. doi: 10.1097/00001888-200010001-00027. [DOI] [PubMed] [Google Scholar]
- West D C, Pomeroy J R, Park J K, Gerstenberger E A, Sandoval J. Critical thinking in graduate medical education: a role for concept mapping assessment? JAMA. 2000;284:1105–1110. doi: 10.1001/jama.284.9.1105. [DOI] [PubMed] [Google Scholar]
- Allen D D, Bond C A. Prepharmacy predictors of success in pharmacy school: grade point averages, pharmacy college admissions test, communication abilities, and critical thinking skills. Pharmacotherapy. 2001;21:842–849. doi: 10.1592/phco.21.9.842.34566. [DOI] [PubMed] [Google Scholar]
- Goodfellow L T. Respiratory therapists and critical-thinking behaviors: a self-assessment. J Allied Health. 2001;30:20–25. [PubMed] [Google Scholar]
- Ennis R H. A logical basis for measuring critical thinking skills. Educ Leadership. 1985;43:44–98. [Google Scholar]
- Paul R. Critical Thinking: How to Prepare Students for a Rapidly Changing World. Foundation for Critical Thinking; Santa Rosa, CA: 1993. [Google Scholar]
- American Philosophical Association . American Philosophical Association; Newark, DE: 1990. Critical Thinking: A Statement of Expert Consensus for Purposes of Educational Assessment and Instruction. (ERIC document ED 315–423.) [Google Scholar]
- Facione N C, Facione P A, Sanchez C A. Critical thinking disposition as a measure of competent clinical judgment: the development of the California Critical Thinking Disposition Inventory. J Nurs Educ. 1994;33:345–350. doi: 10.3928/0148-4834-19941001-05. [DOI] [PubMed] [Google Scholar]
- Facione P A, Facione N C, Giancarlo C A. The motivation to think in working and learning. In: Jones E, editor. Defining Expectations for Student Learning. Jossey-Bass; San Francisco, CA: 1996. [Google Scholar]
- Facione P A, Facione N C. The California Critical Thinking Disposition Inventory (CCTDI): Test Administration Manual. California Academic Press; Millbrae, CA: 1992. [Google Scholar]
- Cronbach L J. Essentials of Psychological Testing. 3rd ed Harper and Row; New York, NY: 1970. [Google Scholar]
- Facione P A, Facione N C, Giancarlo C A. Professional Judgment and the Disposition Toward Critical Thinking. California Academic Press; Millbrae, CA: 1998. [Google Scholar]
- Bers T H, McGowan M, Rubin A. The disposition to think critically among community college students: The California Critical Thinking Disposition Inventory. J Gen Educ. 1996;45:197–221. [Google Scholar]
- Facione P A, Giancarlo C A, Facione N C. Are College Students Disposed to Think? California Academic Press; Millbrae, CA: 1993. [Google Scholar]