

Abstract
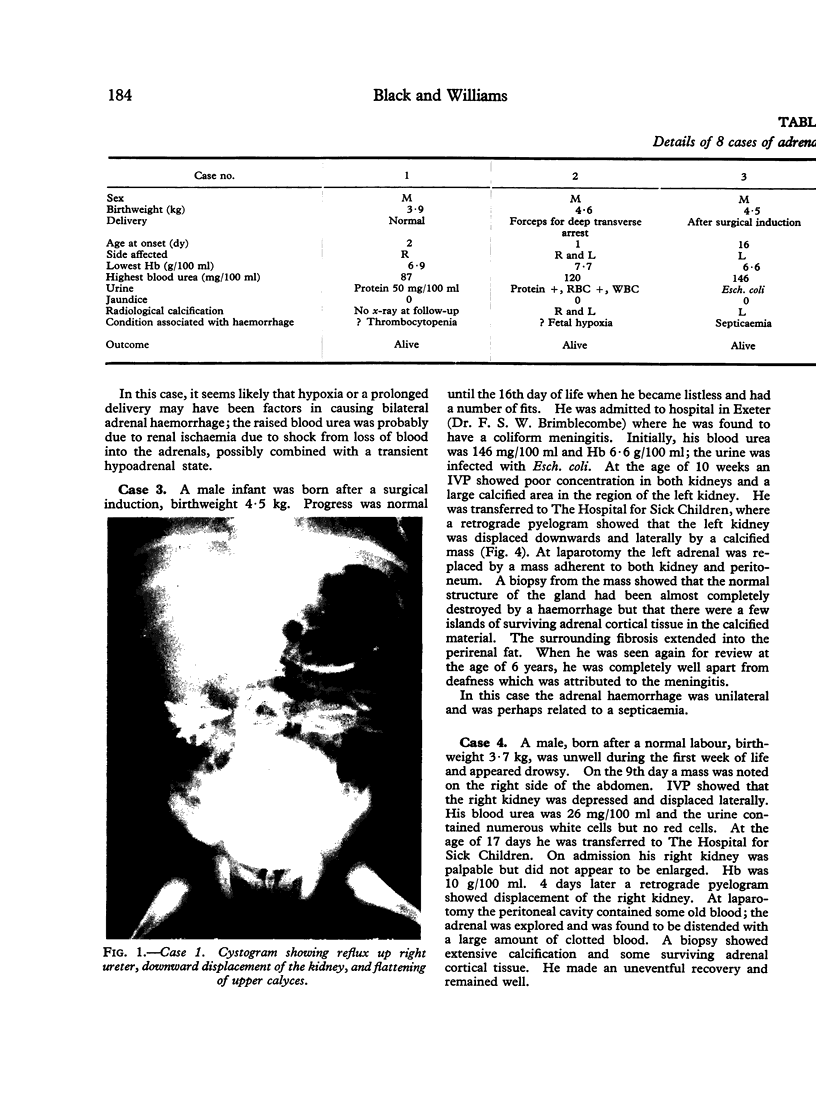
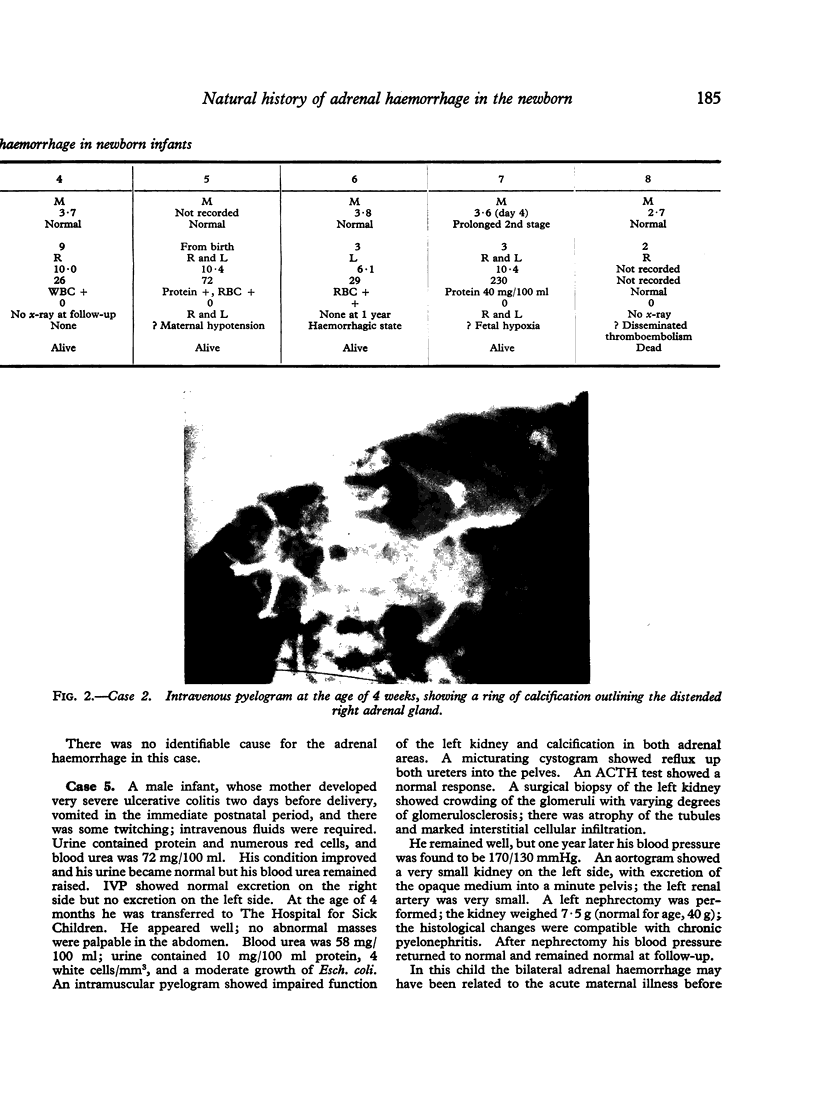
5 cases of unilateral and 3 cases of bilateral haemorrhage are described. Only 1 infant died, from venous thromboses elsewhere. Apart from this case, all had an above average birthweight. Probable predisposing causes apart from large size were fetal hypoxia, septicaemia, thrombocytopenia, coagulation defect, and disseminated thromboembolic disease. The condition must be distinguished from renal vein thrombosis. In the acute stage pyelography shows depression of the kidney on the affected side, with flattening of the upper calyces. Calcification develops rapidly round the periphery of the mass, then slowly contracts into an area of the size and shape of the original gland. Treatment is with antibiotics and blood transfusion, with intravenous corticosteroids in severely shocked or bilateral cases. Adrenal insufficiency is rarely found on follow-up even in bilateral cases, but renal hypertension should be looked for. No single cause for the haemorrhage could be discovered, but the preponderance of haemorrhage into the right adrenal gland is probably due to anatomical differences between the venous drainage of the two sides.
Full text
PDF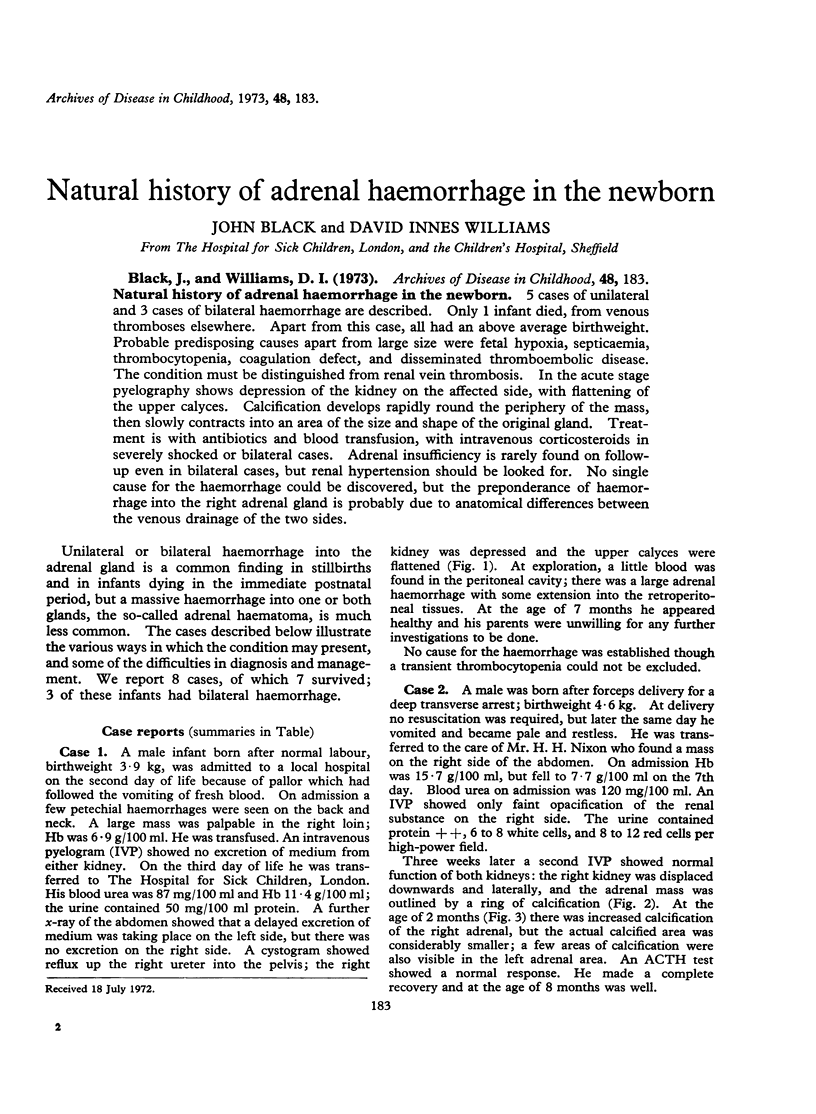

Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boyd J. F. Disseminated fibrin thrombo-embolism in stillbirths: a histological picture similar to one form of maternal hypofibrinogenaemia. J Obstet Gynaecol Br Commonw. 1966 Aug;73(4):629–639. doi: 10.1111/j.1471-0528.1966.tb15544.x. [DOI] [PubMed] [Google Scholar]
- Boyd J. F. Disseminated fibrin thromboembolism among neonates dying within 48 hours of birth. Arch Dis Child. 1967 Aug;42(224):401–409. doi: 10.1136/adc.42.224.401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dobbie J. W., Symington T. The human adrenal gland with special reference to the vasculature. J Endocrinol. 1966 Apr;34(4):479–489. doi: 10.1677/joe.0.0340479. [DOI] [PubMed] [Google Scholar]
- Fox B. Adrenal haemorrhage and necrosis resulting from abdominal operations. Lancet. 1969 Mar 22;1(7595):600–602. doi: 10.1016/s0140-6736(69)91535-9. [DOI] [PubMed] [Google Scholar]
- Fox B. Unilateral adrenal necrosis and haemorrhage following operations on the stomach. J Pathol. 1969 Jan;97(1):127–135. doi: 10.1002/path.1710970116. [DOI] [PubMed] [Google Scholar]
- GAGNON R. The arterial supply of the human adrenal gland. Rev Can Biol. 1957 Dec;16(4):421–433. [PubMed] [Google Scholar]
- GAGNON R. The venous drainage of the human adrenal gland. Rev Can Biol. 1956 Feb;14(4):350–359. [PubMed] [Google Scholar]
- HILL E. E., WILLIAMS J. A. Massive adrenal haemorrhage in the newborn. Arch Dis Child. 1959 Apr;34(174):178–182. doi: 10.1136/adc.34.174.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SEVITT S. Post-traumatic adrenal apoplexy. J Clin Pathol. 1955 Aug;8(3):185–194. doi: 10.1136/jcp.8.3.185. [DOI] [PMC free article] [PubMed] [Google Scholar]