

Abstract
Objective:
Our objectives were to describe the preoperative mood levels and psychological readiness levels of patients undergoing primary reconstruction of the anterior cruciate ligament (ACL) and to examine differences between adolescent and adult sports medicine patients relative to psychological readiness for ACL surgery.
Design and Setting:
Subjects prospectively completed assessments of preoperative mood and psychological readiness for ACL surgery and rehabilitation.
Subjects:
The sample consisted of subjects (N = 121) involved, on average, in sport or exercise participation 12.5 h/wk (SD = 7.5); subgroups included adolescents (15–19 years of age, n = 67) and adults (≥30 years of age, n = 32).
Measurements:
Subjects preoperatively provided self-reported assessments of demographics, mood disturbances, 10 psychological processes of change (consciousness raising, dramatic relief, environmental reevaluation, social liberation, self-reevaluation, counterconditioning, helping relationships, reinforcement management, stimulus control, and self-liberation), decisional balance (pros versus cons of surgery), and self-efficacy.
Results:
Relative to the first objective, subjects reported more pros than cons associated with surgery and relatively high levels of self-efficacy. Relative to the second objective, a significant main effect was noted (Wilks lambda = 0.58, P < .01), with 42% of the variance in the dependent variables being attributed to differences among adolescents as compared with adults. Follow-up analyses indicated that, as compared with adults, adolescents reported higher mood disturbances, more pros associated with surgery, and greater use of dramatic relief, environmental reevaluation, social liberation, helping relationships, and self-liberation.
Conclusions:
It may be advantageous to screen patients preoperatively relative to their psychological readiness for surgery and rehabilitation. Also, adolescents reported higher preoperative mood-disturbance levels than adults but higher levels of what would be considered “psychological readiness” for surgery.
Keywords: transtheoretic model, rehabilitation, patient education
Recent advances in anterior cruciate ligament (ACL) surgical techniques and rehabilitation protocols have resulted in improved patient outcomes (eg, faster return to desired activities, fewer long-term complications); however, ACL surgery still requires vigorous and extensive rehabilitation efforts from patients.1 Thus, for optimal recovery from ACL surgery to occur, there must not only be expert medical care (eg, surgical skill, an appropriate rehabilitation program) but also “patient readiness” and commitment.2 Patients' psychological readiness may be particularly important when one considers that numerous sports medicine patients schedule ACL surgery on the basis of logistical considerations (eg, a break in the semester for students, insurance objectives) rather than when they are psychologically ready for the rehabilitation demands associated with ACL surgery.
In this study—part of a larger investigation on the psychological aspects of the injury3,4—we adapted the Psychological Readiness for Change (PRC) model (also referred to as the stages of change or transtheoretic model) for use within a sports medicine rehabilitation context. The PRC model has been successfully used as a way of understanding a wide range of health behavior, including exercise adherence,5 chronic pain management,6 and smoking cessation.7 We examined several components of the PRC model because it related to ACL surgery, including processes of change, decisional balance (ie, pros versus cons of surgery and rehabilitation), self-efficacy, and mood disturbances.
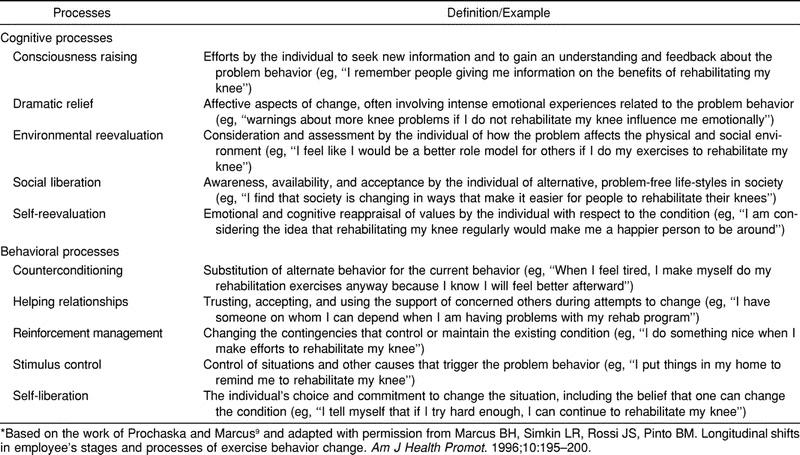
First, processes of change are cognitive or behavioral activities that people use to alter their experiences or their environments (or both) as a way of modifying their behavior.8 Ten processes of change are thought to be relevant when considering health-behavior change, with 5 of these processes focusing on cognitive strategies and 5 capturing behavioral strategies7 (Table 1). Second, we considered decisional balance or individuals' perceptions of the pros (ie, benefits) and cons (ie, costs) associated with engaging in a behavior.8 Earlier research has indicated that individuals are typically ill prepared to make significant health-related changes when they perceive the cons as outweighing the pros.9
Table 1.
The Processes of Change for Rehabilitation*
Third, self-efficacy, which is defined as the belief that one can successfully execute a desired behavior10 (eg, complete rehabilitation when fatigued), increases linearly as individuals become more psychologically ready for health-related changes.11 A final component believed to be relevant to ACL patients' readiness is mood-disturbance levels. Past researchers have documented that among physically active populations, injuries are associated with increases in mood disturbances.12 Although not a component of the original PRC model, mood disturbances, in our clinical experience, may impair patients' ability to take in relevant surgery-related cues and, thereby, indirectly influence their psychological readiness for surgery.
To date, research using the PRC model in a sports medicine context has been limited, with an exception being the work of Wong.13 Wong provided initial psychometric data for the PRC model in a sports medicine setting but used a sample that was heterogenous with respect to injury type and severity. We attempted to extend Wong's work by using a homogenous sample relative to injury type and adapting the PRC model to explore possible differences between adolescents and adults. Because many individuals who undergo ACL surgery are young, we considered it important to understand whether adolescents are different from adults with respect to PRC-related variables.
Thus, the 2 objectives of this study were to (1) describe the mood-disturbance levels and psychological readiness levels of preoperative ACL patients and (2) examine differences between adolescent and adult sports medicine patients relative to psychological readiness for ACL surgery. Because of the exploratory nature of the investigation, no specific hypotheses were forwarded.
METHODS
Subjects
Eligible subjects included individuals who were diagnosed with ACL injury and scheduled for primary ACL reconstruction using a contralateral autogenous patellar tendon graft (N = 121). All subjects had undergone similar patient-education efforts conducted by the participating sports medicine facility. All subjects were operated upon by the same surgeon and subsequently followed similar rehabilitation protocols as outlined by the participating sports medicine facility.
Subjects' mean age was 21.6 years (SD = 8.0), with the ages of subjects ranging from 15 to 48 years. Males composed 65% of the sample, and in terms of ethnicity, 95% categorized themselves as white, 2% as African American, 2% as Hispanic, and 1% as other. On average, the subjects were involved in sports or regular physical activity 12.5 h/wk (SD = 7.5). Ninety percent of the sample indicated that they were undergoing surgery to return to sports or regular exercise, whereas 10% indicated the primary reason for having surgery was to be able to return to daily activities.
For those analyses comparing adolescents with adults, adolescents were operationally defined as subjects 19 years of age or younger (n = 67). Within the participating sports medicine clinic in this investigation, ACL surgery is typically not conducted on individuals less than 15 years of age because of medication considerations. Thus, no subjects were younger than 15 years of age. To help ensure that the comparison group of adults was developmentally distinct from the adolescents, we defined adults as patients who were 1 standard deviation older than the mean age of the sample. Thus, the adult group (n = 32) was defined as subjects 30 years of age or older (ie, 22 years of age plus 8 years = 30 years).
Measures
Demographics and Background Information
We assessed subjects on demographic and background information through a questionnaire designed for the objectives of this study. Specifically, subjects provided information such as age, sex, ethnicity, previous injury history, and hours per week of sport or exercise participation.
Processes of Change
Subjects reported on the extent to which they engaged in the 10 previously identified processes of change (see Table 1) through a modified version of Wong's 30-item Processes of Change Questionnaire for Injury Rehabilitation (POCQ-IR).13 Each of the 10 subscales on the POCQ-IR contained 3 items. Subjects responded using a 5-point Likert scale (1 = never, 5 = frequently) on the basis of the extent to which they engaged in or made use of a particular cognitive or behavioral strategy. Minor wording changes were made in Wong's questionnaire to render it more specific for ACL patients and to improve its readability for adolescent patients.
Decisional Balance
Subjects reported on the perceived pros (eg, “I would feel good about myself if I kept up my commitment to rehabilitate my knee”) and cons (eg, “rehabilitating my knee would take too much of my time”) associated with engaging in their rehabilitation program through a 15-item questionnaire originally developed by Marcus et al.14 Minor wording changes to the original questionnaire made it more specific for ACL injury rehabilitation. Subjects responded using a 5-point Likert scale (1 = not at all important, 5 = extremely important) on the basis of the extent to which they believed that a given statement was a relevant benefit or cost associated with their injury rehabilitation.
Self-Efficacy
Self-efficacy was assessed through a self-efficacy measure originally developed by Marcus et al15 and subsequently modified by Wong13 for use in an injury rehabilitation setting (SE-IR). The SE-IR used by Wong contained 5 items on a 5-point scale (1 = not at all confident, 5 = very confident) assessing how confident individuals feel about their performance in rehabilitation when faced with myriad obstacles (eg, “I feel I don't have the time”). Given the potential influence of medical insurance on rehabilitation behavior, we added a sixth item to the SE-IR: “my insurance does not cover the cost of rehabilitating my injury.”
Mood Disturbances
Mood-disturbance levels were assessed through the short-form Profile of Mood States (POMS-SF),16 which is a version of the full-length POMS.17 The POMS-SF includes 6 subscales; 5 assess negative mood states (ie, tension, depression-dejection, anger, fatigue, and confusion) and 1 assesses positive mood (ie, vigor). However, for the objectives of this study, only a total mood-disturbance value was calculated. Subjects rated the degree to which they experienced various emotions on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). The POMS-SF appears to have adequate psychometric properties, with scores on the POMS-SF being highly correlated with scores on the full-length POMS (r = .99).16,18 To reduce time demands on subjects, the 37-item POMS-SF was used rather than the 65-item POMS.
Protocol
Before data collection was initiated, the local institutional review board approved the study, and written informed consent was obtained from subjects. We made initial contact with potential subjects when they came to the participating sports medicine facility for an office visit resulting from a knee injury. If subjects agreed to participate, they completed the demographic questionnaire during this initial office visit and before their consultation with their sports medicine physician. Subjects completed the PRC and mood-disturbance assessments on the day of their surgery once they had received extensive patient education that focused on what to expect relative to their surgery and recovery.
Data Analysis
Data analysis took place in several stages. First, we conducted preliminary analyses to verify that the questionnaires demonstrated adequate reliability and that the assumptions associated with the statistical methods used were met. Second, we calculated descriptive statistics on selected variables. Finally, we used multiple analysis-of-variance procedures, with univariate follow-up to examine differences between adolescents and adults relative to the PRC variables and mood disturbances.
RESULTS
Preliminary Analyses
We conducted 2 types of preliminary analyses using the entire data set. First, we conducted preliminary analyses to verify that the self-report measures used in the study demonstrated adequate internal reliability. A scale that provided a Cronbach alpha of .70 or greater was considered to demonstrate adequate internal reliability.19 All scales or subscales met this criterion except for the consciousness-raising subscale from the POCQ-IR questionnaire. Specifically, the consciousness-raising subscale had an internal reliability level of .58. By removing the first item from this subscale (and making the adjustments to calculate the subscale's scores based on 2 rather than 3 items), the modified consciousness-raising subscale met the .70 criteria level for internal consistency.
Second, we conducted preliminary analyses to verify that the assumptions of equal variances between the adolescent and adult groups on variables used in the multiple analyses of variance were correct.20 This was important, given the unequal sizes of the adolescent and adult groups. None of the tests of the equality of variances on the variables of interest reached significance, indicating that the assumption of homogeneity of variances was correct.
Objective I: Descriptive Findings
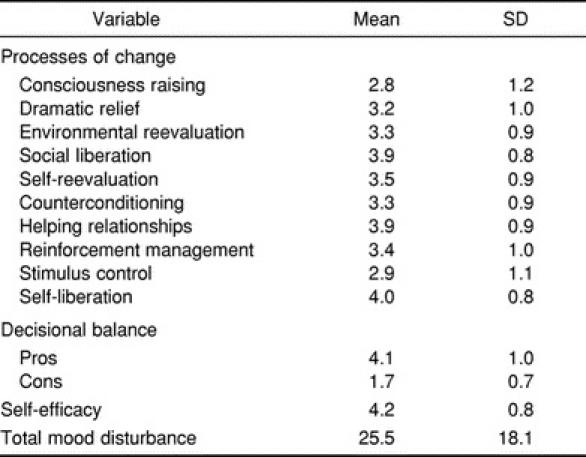
Means and standard deviations for the variables of interest are displayed in Table 2. Subjects tended to perceive more pros than cons associated with ACL surgery and had relatively high levels of self-efficacy as related to injury rehabilitation. In terms of the 10 processes of change, self-liberation, helping relationships, and social liberation were the most used strategies. Alternatively, consciousness raising and stimulus control were the least used strategies.
Table 2.
Processes of Change, Decisional Balance, Self-Efficacy, and Mood Disturbances
Objective II: Adolescent Versus Adult Comparisons
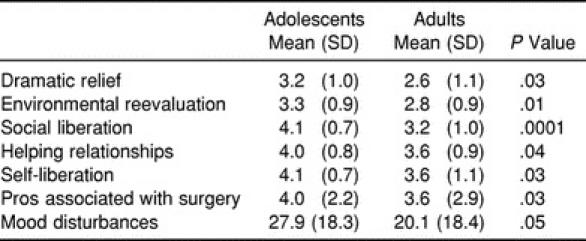
A significant main effect was noted on PRC variables (Wilks lambda = 0.58, P < .0001), with 42% of the variance in the dependent variables being attributable to differences among adolescents as compared with adults. Follow-up analyses indicated that, as compared with adults, adolescents reported higher levels of mood disturbances, more pros associated with surgery, and greater use of dramatic relief, environmental reevaluation, social liberation, helping relationships, and self-liberation, (Table 3).
Table 3.
Significant Comparisons Between Adolescents and Adults
DISCUSSION
Our first objective was to obtain descriptive data relative to an adaptation of the PRC model. We found that, among a group of physically active sports medicine patients who were approaching ACL surgery, psychological readiness for surgery and rehabilitation appeared relatively high. Specifically, subjects reported high levels of self-efficacy, saw more pros than cons associated with surgery, and reported greater use of behavioral as compared with cognitive processes of change. Previous researchers in the exercise–behavior-change literature have suggested that individuals who are less psychologically ready to make behavior changes reported low levels of self-efficacy, more cons than pros associated with the behavior change, and greater use of cognitive processes of change as compared with behavioral processes.5
The data from this investigation can be compared with those reported by Wong.13 A distinct difference between our subjects and those in Wong's study is that we assessed subjects before their rehabilitation began. In contrast, Wong's subjects were already involved in their rehabilitation. Nonetheless, like Wong, we found that the 3 most used processes of change were social liberation, helping relationships, and self-liberation. Marcus et al5 noted that the processes of change and the specific patterning of these processes may vary depending on the domain (eg, exercise behavior versus injury rehabilitation). On the basis of this study and the work of Wong,13 it appears that the above-mentioned processes are particularly salient in the injury-rehabilitation domain, both preoperatively and postoperatively.
The second objective of this investigation was to identify age-related differences among adolescents and adults relative to the psychological processes associated with ACL surgery and rehabilitation. We found significant differences between adolescents and adults, with 42% of the variance in the dependent variables being attributable to group differences. Follow-up analyses indicated that, as compared with adults, adolescents reported higher levels of mood disturbances, more pros associated with surgery, and greater use of 5 of the 10 processes of change (ie, dramatic relief, environmental reevaluation, social liberation, helping relationships, and self-liberation).
The differences we found between adolescents and adults can be examined from a number of perspectives. First, it appears that from a psychological-readiness perspective, adolescents may be more ready for surgery than their adult counterparts because they reported greater use of a number of cognitive and behavioral processes of change and saw more pros associated with surgery. Perhaps among physically active adolescents, the return to a physically active lifestyle is a more salient and desirable outcome than among adults. Thus, adolescents may be more invested in using the cognitive and behavioral strategies they perceive will bring them closer to the goal of returning to physical activity. It could be argued that the adolescents in this sample attempted to provide the “socially desirable” responses and so simply reported using 5 of the 10 processes of change to a greater extent. This explanation seems unlikely, however, given that adolescents also reported higher levels of mood disturbances than their adult counterparts. If adolescents were concerned with presenting themselves in a socially desirable manner, it is likely that they would downplay their mood-disturbance levels.
The finding that adolescents reported higher levels of mood disturbances with respect to their injuries is not completely unexpected. On the one hand, it is generally thought that mood disturbances are more common among adolescents21,22; thus, it may be that the higher mood-disturbance levels reported by the adolescents in this study would have been present irrespective of their injuries. Alternatively, it may be that adolescent patients simply experienced more negative effects after their injuries. Future research is needed to explore whether the higher levels of mood disturbances reported among adolescents were present before their injuries or are the result of their ACL injuries. In the meantime, from a clinical perspective, it is important for sports medicine providers to be aware that mood disturbances are likely to be higher among adolescent ACL patients as compared with their adult counterparts.
Adolescents in this sample reported using 3 cognitive and 2 behavioral processes of change to a greater extent than adults. These results are somewhat unexpected given findings in the health psychology realm. Specifically, researchers have suggested that adolescents are more likely to use behavioral strategies to a greater extent as compared with cognitive processes.23,24 The tendency for adolescents to rely more on behavioral strategies is thought to occur because behavioral processes are more likely to be overtly observed, whereas cognitive processes are more subtle. Thus, it has been thought that it may take until adulthood before individuals learn to incorporate these cognitive strategies. Future research is needed to explore the conditions under which adolescents are more likely than adults to rely on cognitive strategies.
Limitations of the Investigation and Future Research Directions
In terms of future research directions, additional investigation is needed to examine if psychological readiness and related variables are linked to rehabilitation adherence or recovery outcomes or both. Should this be the case, it may be possible to preoperatively screen patients and encourage those who do not appear to be in an optimal psychological state to postpone or reconsider surgery. A limitation of this study is that subjects did not complete their preoperative assessments until the day of their surgery. Using this approach, it would be difficult from a logistic perspective to reschedule patients for ACL surgery. Thus, future researchers should consider assessing patients' readiness closer to when patients initially visit the sports medicine clinic.
Finally, future researchers should be encouraged to examine psychological readiness-for-change factors among a more ethnically and motivationally diverse sample. As noted previously, the personnel of the sports medicine clinic in this investigation dedicate what they believe to be considerable time and energy toward preoperative patient education. Therefore, to what extent they may have contributed to patients' psychological readiness for ACL surgery, and, in turn, patients' motivations and mood levels, is unknown.
Clinical Implications
Without ignoring the above-mentioned limitations, a number of clinical implications can be drawn from this study. First, many health care providers take into account presurgical physical factors (eg, amount of tissue damage, swelling) when scheduling surgery; it may be worthwhile to also consider psychological factors such as patients' readiness for surgery. Second, because the psychological profile of the adult patient is different from that of the adolescent patient, the approach of the sports medicine provider toward patient care should be flexible. In particular, adolescents tend to demonstrate a more negative affect, which may make working with adolescent patients more taxing for the sports medicine provider.
ACKNOWLEDGMENTS
This study is part of a larger investigation of the psychological processes associated with ACL surgery among sports medicine patients. The interested reader is referred to references 3 and 4. This research was supported by an Internal Grant-In-Aid from the Indiana University–Purdue University at Indianapolis. We thank Danielle Gross and Jared Sigler, who helped with data collection and entry.
REFERENCES
- 1.Brewer BW, Van Raalte JL, Cornelius AE, et al. Psychological factors, rehabilitation, adherence, and rehabilitation outcome after anterior cruciate ligament reconstruction. Rehabil Psychol. 2000;45:20–37. doi: 10.1037/a0031297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hellman EA. Use of the stages of change in exercise adherence model among older adults with a cardiac diagnosis. J Cardiopulm Rehabil. 1997;17:145–155. doi: 10.1097/00008483-199705000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Udry E, Shelbourne KD, Gray T, Williams L. Preliminary psychometric evaluation of the transtheoretical model within a sports injury rehabilitation setting. Paper presented at: Annual Conference of the Association for the Advancement of Applied Sport Psychology; October 30–November 3, 2002; Tucson, AZ. [Google Scholar]
- 4.Udry E, Shelbourne KD, Gray T. Perioperative mood changes and its relationship to recovery in patients following ACL reconstruction. Paper presented at: Annual Conference of the American College of Sports Medicine; May 29–June 1, 2002; St. Louis, MO. [Google Scholar]
- 5.Marcus BH, Rossi JS, Selby VC, Niaura RS, Abrams DB. The stages and processes of exercise adoption and maintenance in a worksite sample. Health Psychol. 1992;11:386–395. doi: 10.1037//0278-6133.11.6.386. [DOI] [PubMed] [Google Scholar]
- 6.Kerns RD, Rosenberg R, Jamison RN, Caudill MA, Haythornwaite J. Readiness to adopt a self-management approach to chronic pain: The Pain Stages of Change Questionnaire (PSOCQ) Pain. 1997;72:227–234. doi: 10.1016/s0304-3959(97)00038-9. [DOI] [PubMed] [Google Scholar]
- 7.Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51:390–395. doi: 10.1037//0022-006x.51.3.390. [DOI] [PubMed] [Google Scholar]
- 8.Marcus BH, Simkin LR. The transtheoretical model: applications to exercise behavior. Med Sci Sports Exerc. 1994;26:1400–1404. [PubMed] [Google Scholar]
- 9.Prochaska JO, Marcus BH. The transtheoretical model. In: Dishman RK, editor. Advances in Exercise Adherence. Champaign, IL: Human Kinetics; 1994. pp. 161–180. [Google Scholar]
- 10.Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- 11.Gorely T, Gordon S. An examination of the transtheoretical model and exercise behavior among older adults. J Sport Exerc Psychol. 1995;17:312–324. [Google Scholar]
- 12.Leddy MH, Lambert MJ, Ogles BM. Psychological consequences of athletic injury among high level competitors. Res Q Exerc Sport. 1994;65:347–354. doi: 10.1080/02701367.1994.10607639. [DOI] [PubMed] [Google Scholar]
- 13.Wong IE. Injury Rehabilitation Behavior: An Investigation of Stages and Processes of Change in the Athlete-Therapist Relationship [master's thesis] Eugene, OR: University of Oregon; 1998. [Google Scholar]
- 14.Marcus BH, Rakowski W, Rossi JS. Assessing motivational readiness and decision making for exercise. Health Psychol. 1992;11:257–261. doi: 10.1037//0278-6133.11.4.257. [DOI] [PubMed] [Google Scholar]
- 15.Marcus BH, Selby VC, Niaura RS, Rossi JS. Self-efficacy and the stages of exercise behavior change. Res Q Exerc Sport. 1992;63:60–66. doi: 10.1080/02701367.1992.10607557. [DOI] [PubMed] [Google Scholar]
- 16.Shacham S. A shortened version of the Profile of Mood States. J Pers Assess. 1983;47:305–306. doi: 10.1207/s15327752jpa4703_14. [DOI] [PubMed] [Google Scholar]
- 17.McNair D, Lorr M, Droppelman L. Manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service; 1971. [Google Scholar]
- 18.Curran SL, Andrykowski MA, Studts JL. Short form of the Profile of Mood States (POMS-SF): psychometric information. Psychol Assess. 1995;7:80–83. [Google Scholar]
- 19.Nunnally J. Psychometric Theory. New York, NY: McGraw-Hill; 1978. [Google Scholar]
- 20.Tabachnick B, Fidell L. Using Multivariate Statistics. 3rd ed. New York, NY: HarperCollins; 1996. [Google Scholar]
- 21.Hall GS. Adolescence: Its Psychology and Its Relations to Physiology, Anthropology, Sociology, Sex, Crime, Religion, and Education. Englewood Cliffs, NJ: Prentice Hall; 1904. [Google Scholar]
- 22.Cicchetti D, Rogosch F. A developmental psychopathology perspective on adolescence. J Consult Clin Psychol. 2002;70:6–20. doi: 10.1037//0022-006x.70.1.6. [DOI] [PubMed] [Google Scholar]
- 23.Gil KM, Wilson JJ, Edens JL. The stability of pain coping strategies in young children, adolescents, and adults with sickle cell disease over an 18-month period. Clin J Pain. 1997;13:110–115. doi: 10.1097/00002508-199706000-00005. [DOI] [PubMed] [Google Scholar]
- 24.Thompson RJ, Gustafson KE, editors. Adaptation to Chronic Childhood Illness. Washington, DC: American Psychological Association; 1996. [Google Scholar]