

Abstract
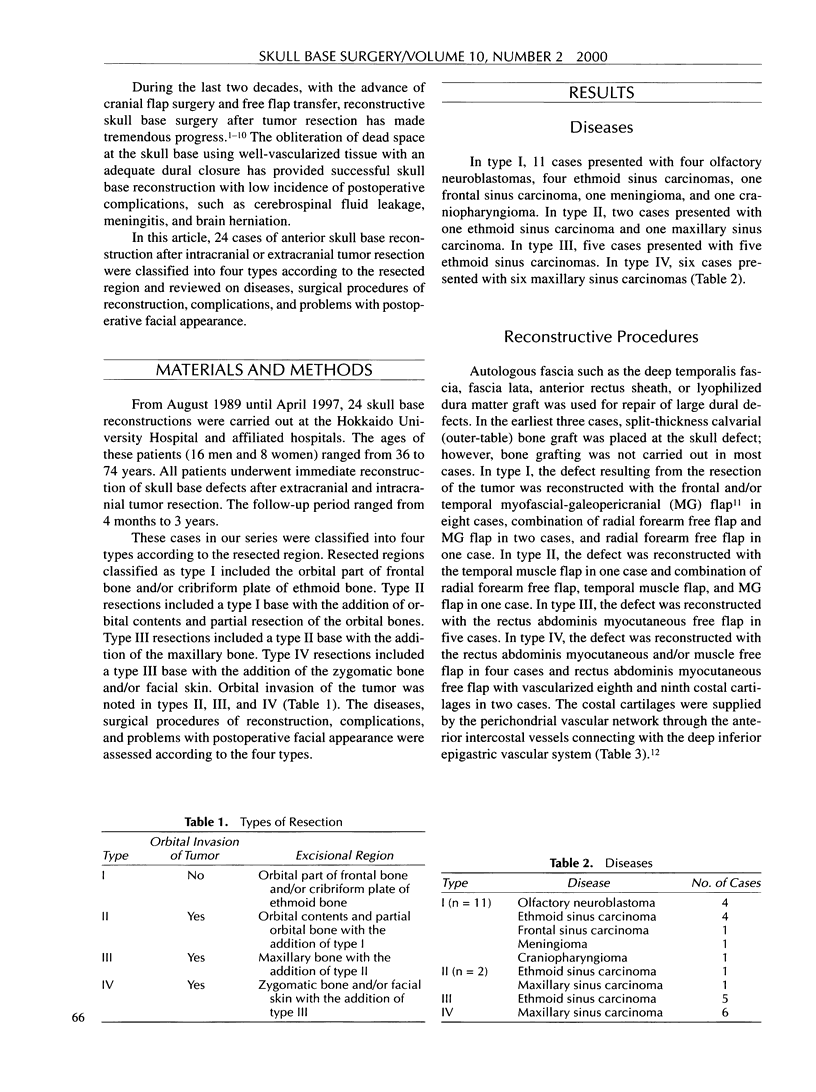
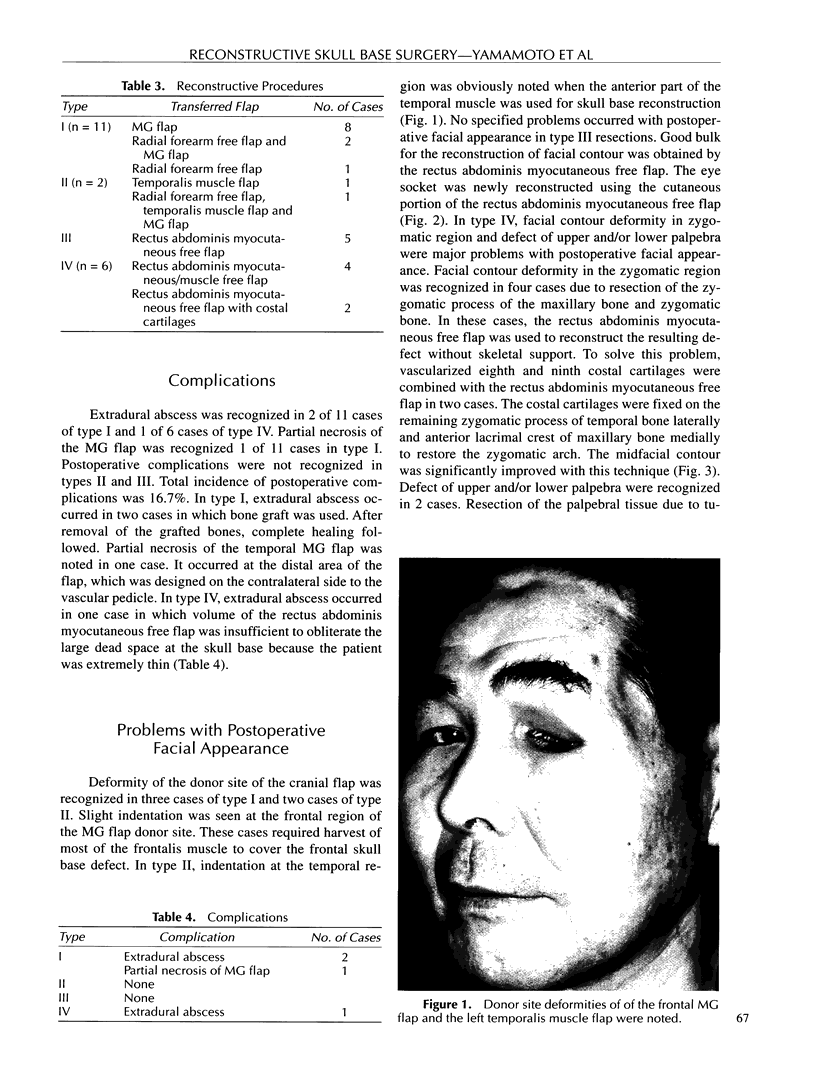
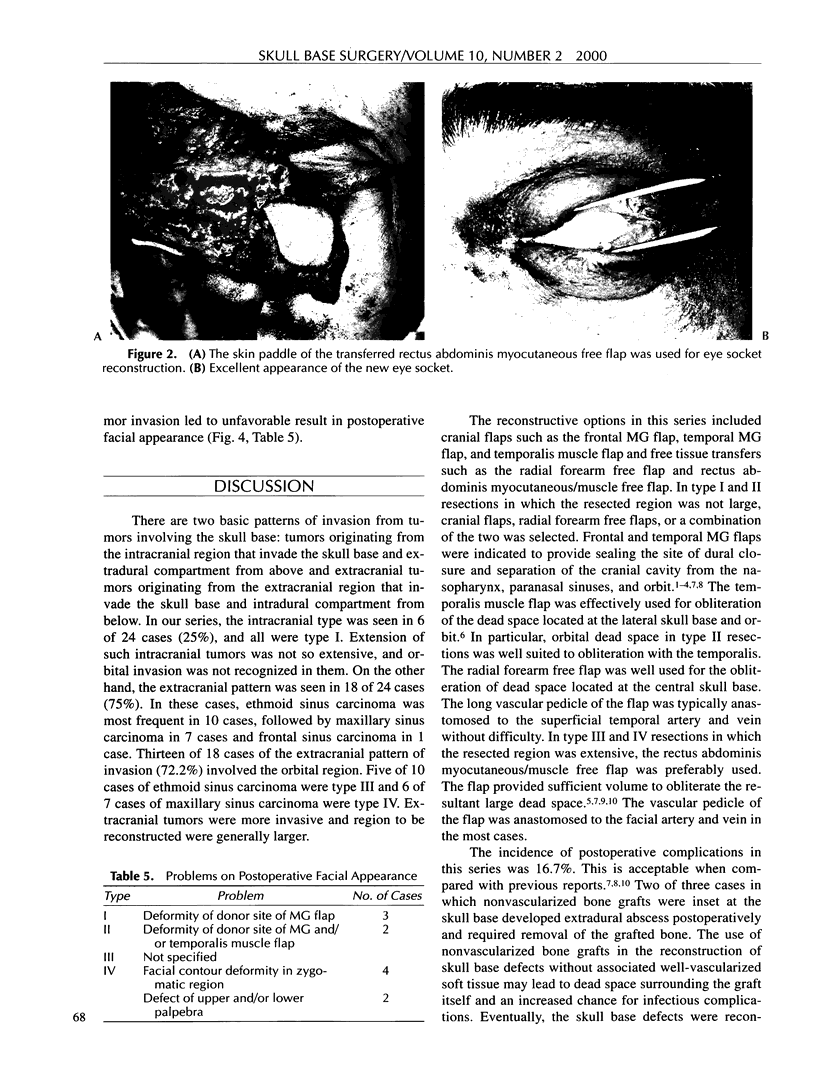
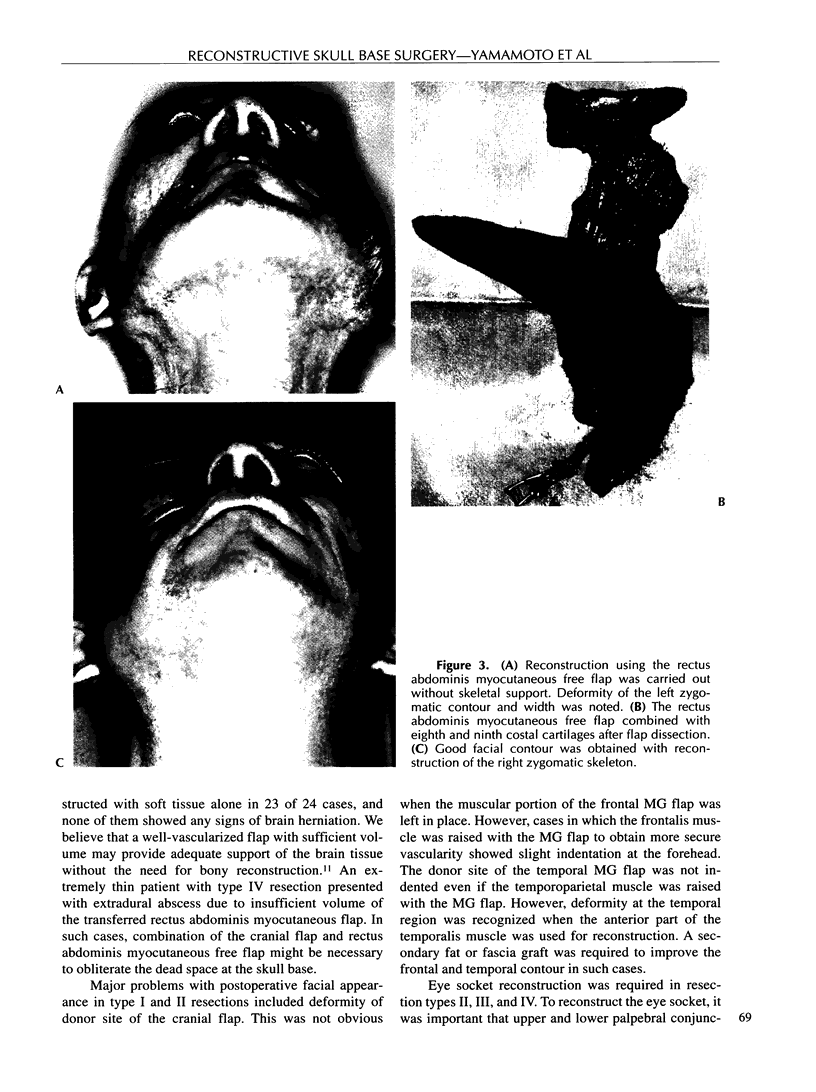
This article details our experience with 24 cases of anterior skull base reconstruction after tumor resection. They were classified into four types according to the resected region. In 11 cases of type I resection, the orbital part of frontal bone and/or cribriform plate of ethmoid bone were resected. In two cases of type II resection, the orbital contents and partial orbital bone were resected with the addition of type I. In five cases of type III resection, the maxillary bone was resected with the addition of type II. In six cases of type IV resection, the zygomatic bone and/or facial skin were resected with the addition of type III. The tumor originating from intracranial region was 25% of this series and all of them belonged to type I. The tumor originating from extracranial region tumor was 75% and its resected region was more extensive. In type I and II resections, the cranial flap, radial forearm free flap, or a combination of the two was used for reconstruction. The rectus abdominis myocutaneous/muscle free flap was used for reconstruction of massive defects in type III and IV defects. Total incidence of postoperative complications was 16.7%. Donor site deformity of the cranial flap at the frontal and temporal region in types I and II resections and facial contour deformity in zygomatic region and defect of upper and/or lower palpebra in type IV resection were major problems with postoperative facial appearance. Although use of the rectus abdominis myocutaneous free flap combined with costal cartilages improved the midfacial contour, palpebral reconstruction remained an unsolved problem in reconstructive skull base surgery. The reconstructive goals in skull base surgery are not only to obtain safe and reliable skull base reconstruction but also to restore the facial appearance postoperatively.
Full text
PDF

Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arden R. L., Mathog R. H., Thomas L. M. Temporalis muscle-galea flap in craniofacial reconstruction. Laryngoscope. 1987 Nov;97(11):1336–1342. doi: 10.1288/00005537-198711000-00017. [DOI] [PubMed] [Google Scholar]
- Eriksson E., Brånemark P. I. Osseointegration from the perspective of the plastic surgeon. Plast Reconstr Surg. 1994 Mar;93(3):626–637. [PubMed] [Google Scholar]
- Horowitz J. H., Persing J. A., Nichter L. S., Morgan R. F., Edgerton M. T. Galeal-pericranial flaps in head and neck reconstruction. Anatomy and application. Am J Surg. 1984 Oct;148(4):489–497. doi: 10.1016/0002-9610(84)90375-1. [DOI] [PubMed] [Google Scholar]
- Izquierdo R., Leonetti J. P., Origitano T. C., al-Mefty O., Anderson D. E., Reichman O. H. Refinements using free-tissue transfer for complex cranial base reconstruction. Plast Reconstr Surg. 1993 Sep;92(4):567–575. [PubMed] [Google Scholar]
- Johns M. E., Winn H. R., McLean W. C., Cantrell R. W. Pericranial flap for the closure of defects of craniofacial resection. Laryngoscope. 1981 Jun;91(6):952–959. doi: 10.1288/00005537-198106000-00013. [DOI] [PubMed] [Google Scholar]
- Jones N. F., Schramm V. L., Sekhar L. N. Reconstruction of the cranial base following tumour resection. Br J Plast Surg. 1987 Mar;40(2):155–162. doi: 10.1016/0007-1226(87)90188-3. [DOI] [PubMed] [Google Scholar]
- Jones N. F., Sekhar L. N., Schramm V. L. Free rectus abdominis muscle flap reconstruction of the middle and posterior cranial base. Plast Reconstr Surg. 1986 Oct;78(4):471–479. doi: 10.1097/00006534-198610000-00005. [DOI] [PubMed] [Google Scholar]
- Schramm V. L., Jr, Myers E. N., Maroon J. C. Anterior skull base surgery for benign and malignant disease. Laryngoscope. 1979 Jul;89(7 Pt 1):1077–1091. [PubMed] [Google Scholar]
- Shah J. P., Galicich J. H. Craniofacial resection for malignant tumors of ethmoid and anterior skull base. Arch Otolaryngol. 1977 Sep;103(9):514–517. doi: 10.1001/archotol.1977.00780260044002. [DOI] [PubMed] [Google Scholar]
- Snyderman C. H., Janecka I. P., Sekhar L. N., Sen C. N., Eibling D. E. Anterior cranial base reconstruction: role of galeal and pericranial flaps. Laryngoscope. 1990 Jun;100(6):607–614. doi: 10.1288/00005537-199006000-00011. [DOI] [PubMed] [Google Scholar]
- Yamada A., Harii K., Ueda K., Asato H. Free rectus abdominis muscle reconstruction of the anterior skull base. Br J Plast Surg. 1992 May-Jun;45(4):302–306. doi: 10.1016/0007-1226(92)90057-5. [DOI] [PubMed] [Google Scholar]
- Yamamoto Y., Minakawa H., Yoshida T., Igawa H., Sugihara T., Ohura T., Nohira K. Role of bone graft in reconstruction of skull base defect: is a bone graft necessary. Skull Base Surg. 1993;3(4):223–229. doi: 10.1055/s-2008-1060587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamamoto Y., Sugihara T., Kuwahara H., Qi F. An anatomic study for the rectus abdominis myocutaneous flap combined with a vascularized rib. Plast Reconstr Surg. 1995 Nov;96(6):1336–1340. doi: 10.1097/00006534-199511000-00015. [DOI] [PubMed] [Google Scholar]