

Abstract
Objective
To explore physicians’ work practices in relation to their long-term use of a computerized physician order entry system (CPOE).
Design
A cross-sectional qualitative study was conducted in four clinical units in two large Australian teaching hospitals. One hospital had used CPOE for over 10 years to order all clinical laboratory and radiology tests and view test results and the other had used the computerized viewing facility of the system for over seven years with tests ordered manually. Data were collected by non-participatory observations of physicians (55 sessions) and 28 interviews.
Measurements
Content analysis of the observation field notes, reflections on observations and interview transcripts were conducted by two researchers independently. A thematic grounded theory approach was used to derive key themes that would explain physicians work practices associated with CPOE use.
Results
Three themes relating to physicians’ established use of CPOE were identified: (1) the effect of the hospital and clinical environment; (2) changes to work practices; and (3) physicians’ management of information. Physicians’ test management work practices using CPOE were related to diversity between: the hospitals; the clinical units’ environment, and the users of the system.
Conclusion
Hospitals need to understand and analyze physicians’ test management work practices prior to and during the implementation of CPOE to accommodate their diverse ways of working with computerized information systems. In the current mixed media environment, physicians’ use of manual and computerized information systems for sourcing and recording information impacts on efficiency and patient safety.
Background
Synergy between the technology, the user and their work is an important factor in the safe and efficient use of clinical information systems. Studies have emphasized the complex and interruptive nature of clinical work, 1–7 and have suggested to be successfully integrated, information technology needs to fit with the workflow of physicians and within the organizational framework of accepted practices, norms and structures.
Computerized physician order entry systems (CPOE) allow physicians to place, receive, monitor and track clinical laboratory, radiology and medication orders along with other orders, such as clinical consultations, electronically. These systems, particularly those which include medication management, have been shown to have benefits in cost containment and quality of care. 8–13 Yet currently, there are few hospitals which have implemented or mandated hospital-wide computerized order management systems. 14–16
Why has CPOE been slow to diffuse throughout healthcare facilities? Researchers have emphasized organizational and clinical work practice issues rather than technical issues as being critical. 17–29 The slow uptake could also relate to perceptions about the extra time taken to place computerized orders, the inflexibility of applications, working through multiple screens, periodic changes in log-on or user password requirements and interruption of workflow. 11, 30–32 Further studies on physicians’ work practices related to the use of CPOE need to be undertaken to understand the poor uptake of these systems.
Recently there have been cautionary claims that CPOE systems may actually facilitate clinical errors, 30 and their effects on patient outcomes remain understudied. 33 Some 14,34 have questioned the current push toward the rapid adoption of computerized order management systems. Ash and her colleagues 14 describe instances, from their experiences in the United States, The Netherlands and Australia, of silent errors that patient care information systems seem to foster. Safety issues therefore, should also drive further studies on physicians’ use of CPOE.
The use of qualitative research methods to evaluate health information systems has been promoted 22,35–41 in order to complement quantitative methods which have limitations when exploring complex matters related to work practices. 36 Although organizational and work practice issues have been cited as affecting physicians’ use of CPOE, there have been limited qualitative studies exploring how these factors are affected. 36,42,43 There have been no reported studies on the effect of physicians’ long-term use of CPOE on their test management work practices. The aim of this study was to explore, using observations and interviews, changes to physicians’ work practices in relation to their long-standing use of a hospital-wide, mandatory, CPOE system.
Methods
Design and Research Settings
A cross-sectional qualitative study was conducted with observations and interviews related to physicians’ use of CPOE to order clinical laboratory and radiology tests and view results in one hospital, and to order tests manually and view results electronically in a second hospital. The study was conducted in four clinical units in two Australian metropolitan public teaching hospitals ∗ within the same city and under the same administrative structure (▶). The organization and management of the two hospitals’ clinical and administrative systems were centralized. The four clinical units were the Emergency Departments (EDs) and hematology wards at each hospital.
Figure 1.
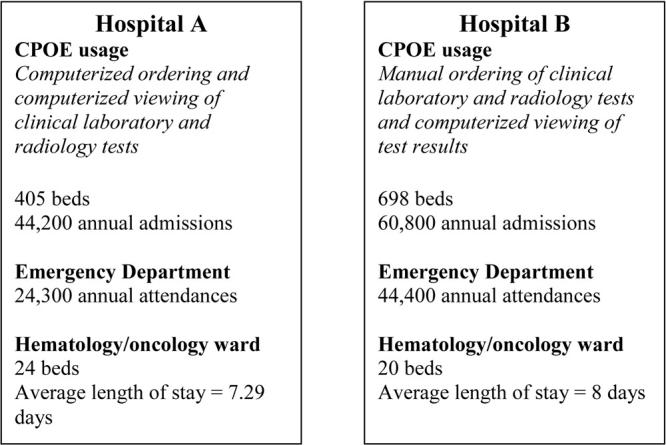
Characteristics of study sites.
Selection and Sampling Logic
The choice of hospitals for the study was based on their long-term use of the same hospital-wide, mandatory CPOE system for all inpatients. The computerized test management system used at Hospital A and Hospital B was Powerchart, which is the test management module of the Cerner clinical information system. Powerchart allows clinicians to view patient demographics, visit/encounter details, scheduled appointments, diagnostic test results (laboratory and radiology), and the test order status. It allows clinicians to place orders for diagnostic tests, consultations, porters and diets. Hospital A used the viewing and ordering functions of Powerchart, whereas Hospital B used the viewing functions only. The clinical sites within the hospitals—the EDs and hematology wards—were suggested by the hospital’s senior management staff due to their high usage of the system and their different needs regarding test management. Since 1991, physicians at Hospital A had used CPOE to order and view clinical laboratory and radiology tests. At the time of the study, Hospital B used CPOE to view test results only with laboratory and radiology test ordering completed manually using paper-based order forms. The computerized viewing of test results at Hospital B had been in place since 1999 and the electronic ordering functions were being phased in. The different implementation stages at the two sites enabled the researchers to observe both computerized and manual test management work practices. At the time of this study neither hospital used the medication management module of the CPOE system.
The participants for the observational aspect of this study were physicians, namely, interns, residents and registrars (i.e., attending physicians). Some senior nurses from the four clinical units were interviewed but were not observed using the system as they had different test ordering entitlements to physicians. Some ED nurses could order the same laboratory and radiology tests as physicians and hematology ward nurses ordered microbiology tests only. Observation days were randomly selected and the observed physicians were a convenience sample of users of the test management system who were on duty during the data collection phase.
Theoretical sampling occurred when we returned to the hospitals to clarify test management work processes. When we found gaps in the data we revisited the hospitals to conduct selective interviews with senior physicians, nurses and others to gain new information that would shed light on the emerging themes. This sampling process allowed us to explore specific issues related to physicians’ test management work processes and their use and integration of information from manual and computerized systems. The theoretical sampling occurred after the initial observations were made and therefore allowed us to explore explanations that arose from the data without assumptions being imposed initially. 44
Data Collection
Two methods of data collection were used in the study: non-participant observations and unstructured field interviews (▶). The non-participant observations, relating to physicians’ test ordering and viewing work practices, were undertaken by two researchers over the four sites (▶). A letter outlining the study, its voluntary nature, the confidentiality of findings and participants, and a consent form, were provided to all participants. A case study protocol 45 was developed which provided a framework for the observations and interviews with general rules to be followed in the field. Pilot observations were undertaken which allowed the researchers to familiarize themselves with the sites and participants.
Figure 2.
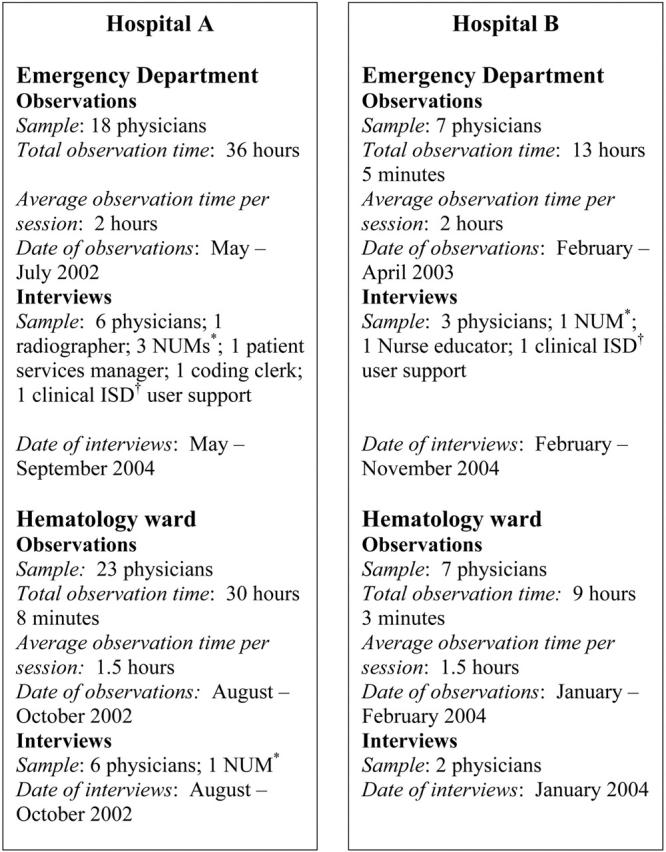
Data collection methods in the four clinical units of the two study hospitals. *Nursing Unit Manager †Information Services Department.
Observations at each site evolved through a series of stages commencing with general observations of physicians working, to more specific observations of individual physicians ordering clinical laboratory and radiology tests and viewing test results. Observations occurred during the hours of 9 am to 5 pm Monday to Friday where the field researchers shadowed physicians in the course of their daily tasks. Internal hospital documents regarding the clinical systems and their usage were collected during the observation visits.
Twenty-eight unstructured interviews with physicians, nurses and information services staff (▶) were undertaken to enable exploration of work processes in more depth. Seventeen interviews were conducted simultaneously with the observations and eleven after the observation period. The post-observation interviews served as member checking of the categories and themes that were emerging from the ongoing analysis of the data.
Field notes from the observations and interviews were transcribed. The researchers then read and reviewed the field notes together and taped their reflections that were also transcribed. Therefore two data sets were created and analyzed: observation and interview notes, and reflections on observations and interviews.
Data Analysis
The two data sets were analyzed using a thematic grounded theory approach 46 to derive themes that would explain the way physicians used the CPOE system. Categories were generated from line by line coding and were included in a memoing document that consisted of notes and reflections on the data that were recorded by the principal researcher (JC) during analysis. This constant comparative method of grounded theory analysis meant that the data were repeatedly studied, analyzed and re-analyzed. The analysis was inductive to allow the categories, themes and relationships to come from the data rather than being imposed prior to data collection.
Rigor of the Qualitative Data
Triangulation was used to improve the validity of findings. 47–51 Investigator and data analysis triangulation was achieved by using two researchers in both the data collection and analysis phases. Data source triangulation occurred as data were collected from physicians, nurses and information services department staff to gain different perspectives on physicians’ use of the test management system. Prolonged engagement or immersion in the field is essential to be satisfied that the data collected are relevant and sufficient to achieve the aim of the study. The researchers were engaged with the study sites from May 2002 to November 2004. Saturation was achieved through 55 separate observations sessions taking a total of 88 hours and 16 minutes and 28 interviews (▶). Member checking of results was achieved by revisiting the study sites after the initial observations and interviews to clarify findings with key participants and undertake more structured interviews with some staff.
Results
Three themes relating to physicians’ work practices associated with the use of the CPOE were identified:
Theme 1: The effect of the hospital and clinical environment
Theme 2: Changes to work practices
Theme 3: Physicians’ management of clinical information
Theme 1: The Effect of the Hospital and Clinical Environment
The hospital and clinical unit environments affected physicians test management work practices. There were differences between the hospitals and the clinical units in physicians’ and nurses’ attitudes to CPOE. These differences were reflected in the different order sets developed at the two hospital EDs and their distinct approaches to nurses ordering tests using CPOE. Order sets can be created in the CPOE system to guide the ordering of tests depending on the patient’s presenting problem. Prior to the implementation of the system nurses from the EDs of both hospitals were not able to order the same laboratory tests as physicians. This changed with implementation and it also coincided with the establishment of the Clinical Initiative Nurse (CIN) whose key role was to initiate treatment to facilitate the processing of patients and reduce ED waiting times. Physicians in the ED of Hospital A developed order sets to be used by nurses only. At the ED in Hospital B a common order set to be used by both junior physicians and nurses was developed. Consequently the order sets between the two hospitals were often different for the same presenting problem. There were perceptions from the nurses in the ED of Hospital A that they were trusted by the physicians. In contrast nurses from the ED at Hospital B believed that order sets were developed to stop over-ordering by interns and to enable physicians to restrict and control which tests nurses could order. The nurses in the ED at Hospital B were also given additional training in test ordering by the physicians that reinforced their perception of the physicians’ control over the process.
There are clinical differences between patients in the ED and hematology wards that affect how tests are ordered and the timing of ordering. In the ED patients generally have urgent health problems and they are assessed, treated and discharged or transferred to the appropriate ward as quickly as possible. It is a busy and sometimes chaotic environment where there are more physicians present on a continual basis than in the hospital ward environment. Activities in the hematology wards in contrast appeared more structured and routine. Patients were admitted specifically for assessment and treatment of their condition and all patients in the ward had a similar clinical profile. These different environments meant that in the EDs, tests were ordered for individual patients by individual physicians and were generally urgent. In the hematology wards, the test ordering process was more team-based and linked to ward rounds. Here, senior physicians during ward rounds reviewed their patients and instructed more junior physicians on which clinical laboratory and radiology tests to order and questioned them on results from previous tests. The hematology physicians in the study sites preferred manual test ordering because it could be completed more easily at the bedside during ward rounds. In the two study hospitals computers were located in the combined physicians/nurses’ stations and not at the bedside and therefore the hematology physicians had to return to that area to place a test order. It was observed that the test ordering process in the hematology wards was generally conducted as a team process. Two physicians, whilst sitting at the computer, would discuss their patients’ test results and decide together which further orders to place. One observation that highlighted the team approach involved two hematology physicians from Hospital A who were observed using the computer together to order tests for patients with one using the mouse and the other the keyboard. In the hematology wards, tests were ordered for groups of patients simultaneously (placing test orders for three days in advance prior to a weekend). Team-work and high levels of verbal communication amongst physicians and between physicians and nurses were also observed in the EDs, but the ordering and viewing of tests on the computer was done alone.
The difference between the two clinical environments was also shown in comments about the differences between the nursing staff in the two areas. There were perceptions that nursing staff working in the EDs were similar in ‘type’ and were different to nurses working elsewhere in the hospital, with one interviewee commenting that, “nurses who work in these areas (ED) are similar… they are all strong.” Another Emergency Department nurse commented, “Emergency Department nurses stay in the ED. New graduates come to the ED and they either like it or they don’t. It is rare that older experienced nurses come to ED—if nurses leave ED they go to a more senior job in a related area or they leave nursing full stop.”
Comments and observations represented by this theme were assigned the following descriptive categories during the coding process: (1) different hospital environments; and (2) different clinical environments. Representative observations or interview quotes are shown in ▶.
Table 1.
Table 1. Theme 1—The Effect of the Hospital and Clinical Environments: Representative Observations and Quotations from Interviews
| Categories | Observation or Quotation |
|---|---|
| Category 1: Different hospital environments | “Care sets were developed to stop over-ordering and because physicians wanted to restrict what nurses could order.” [Hospital B ED ∗ nurse interview] |
| “There is faith in the role of the nurse.”[Hospital A ED ∗ nurse interview] | |
| “Physicians did not want nurses to have same ordering rights as they did.” [Hospital B ED ∗ nurse interview] | |
| “Clinical practice varies from hospital to hospital.” [Hospital A ED ∗ physician interview] | |
| Category 2: Different clinical environments | “Different ordering practices … were due to location (ward, ED ∗ , CCU†) and casemix.” [IT clinical support personnel interview] |
| “Chaotic and busy, things happen quickly.” [Hospital A ED ∗ observation] | |
| “Everything seems routine—bloods taken for all patients at the same time every day.” [Hospital B hematology ward observation] | |
| “The hematology test ordering environment is different to the Emergency Department—they order tests for a number of patients at the one time whereas in ED ∗ they order for one patient at a time.” [Hospital A hematology ward observation] | |
| “I can’t see the PC at the bedside … need wireless or palmtop. ED ∗ is fluid and dynamic.” {Hospital B ED ∗ physician interview] |
∗ Emergency Department.
† Coronary Care Unit.
Theme 2: Changes to Work Practices
Computerized test management work practices differ from ordering diagnostic tests and x-rays using paper order forms and viewing results in hardcopy, paper form. Fields can be made mandatory for a computerized test order whereas manual order forms allow orders to be placed without full completion. The location and number of computers available affect computerized ordering whereas paper order forms are generally readily accessible and available. Physicians can be seated on a patient’s bed completing a manual order however this was not possible for computerized test orders as computers were only located in the physicians/nurses station and not at the bedside.
The changes to work practices theme is linked to the effect of the hospital and clinical environment as discussed under Theme 1. As the test ordering process in the hematology wards was linked to the ward round process, these physicians were generally in favor of ordering at the bedside, whereas ED physicians thought that this could interrupt their examination of the patient. One Emergency Department doctor commented that if physicians used the computer at the bedside and they were not proficient “this could look bad in front of the patient” [Hospital A ED physician].
The ways in which physicians used the test management system to order tests were also observed to be different across the clinical sites. Some physicians selected from the menu the ‘personal list’ of patients and others used the ‘Emergency Department list’ to commence ordering a test. Some used the order sets to guide their selection of which clinical laboratory test to order and others did not. One physician printed out a CT result as it was long and complicated and he thought it would be easier to read the paper version.
There were work practice changes that were specific to the use of the CPOE. The users had developed workarounds to save time. For example, a full stop could be inserted into the ‘clinical history’ field, a mandatory field, rather than type the patient’s full text clinical history. Access to CPOE throughout the hospital meant that physicians could access results and place orders from anywhere within the hospital. Hematology physicians thought this was very convenient and had not been possible with the manual system. Although the CPOE at the study sites did not have decision support functions it did have prompts to alert users to order tests that he/she may not have otherwise considered. A number of physicians commented that this prompt function was useful. Computerized test ordering meant that physicians could sequence work differently as the system delays meant that another task could be undertaken whilst waiting, whereas with manual test ordering one physician commented that it was generally carried out from the beginning to the end, in one sitting.
Users of the test management system expressed concerns about the extra time taken to order tests and the delay in receiving results, and the speed of the system. The perceived extra time taken to order tests was not measured in this study and was recorded as a perception expressed by the users. Time and speed are included in the work practice theme as they impact on how physicians use CPOE. Time delays can be due to the lack of computer proficiency of users, delays in processing tests within the laboratories and slowness of computer response time due to hardware factors.
Computerized information systems can give rise to new ways of working. For example, a new work practice of verifying test results, utilizing the CPOE, was being trialed at Hospital A’s Emergency Department. The Director of the ED indicated that it was a safer way of handling the verification of test results. He stated that the endorsement of test results had never been handled systematically across the hospital and this was an example of computerized test ordering being able to improve work practices. He emphasized that this showed the real value of computers “we need to ask how computerized systems can improve work practices.” [Hospital A ED physician].
Comments and observations represented by this theme were assigned the following descriptive categories during the coding process: (1) work process changes; (2) physicians work differently; (3) system speed; (4) time; and (5) new work processes. Representative observations or quotes from the interviews are shown in ▶.
Table 2.
Table 2. Theme 2—Changes to Work Practices: Representative Observations and Quotations from Interviews
| Categories | Observation or Quotation |
|---|---|
| Category 1: Work process changes | “Once the system is in place it can affect the behaviour of physicians…you sequence work differently if you are waiting for something on the computer you go and do something else.” [Hospital A ED physician interview] |
| “Work is different depending on the physician, the patient and the circumstances.” [Hospital A hematology ward observation] | |
| Category 2: Physicians work differently | “Physicians work differently … some write notes whilst talking to the patient and some write notes after examining the patient … it depends on how much they want to retain in their memory or rely on their memory.” [Hospital A ED physician interview] |
| “Some of the physicians use a personal list of patients and some use the Emergency Department list of patients.” [Hospital A ED observation] | |
| “Physicians work differently and the system should be flexible to allow for these differences.” [Hospital A ED physician interview] | |
| Category 3: System speed | “System speed is the important thing—it is the number one thing in terms of physicians’ compliance.” [Hospital A ED physician interview] |
| Category 4: Time | “Need computers at the bedside for ordering to work … otherwise it takes too much time.” [Hospital A hematology ward observation] |
| “Ordering can be time consuming because of the clinical nature of the patients and the type of orders and the volume of the same orders repeated every few days for one patient.” [Hospital A hematology ward observation] | |
| “Ultimately it slows you down … if I am just a physician seeing patients then it is not better, it is not a better system for freeing up physicians to do clinical stuff.” [Hospital B ED physician interview] | |
| Category 5: New work processes (verification of test results) | “Computerized test verification of results is a better and safer system for handling verification of test results.” [Hospital A ED physician interview] |
Abbreviations: ED = Emergency Department.
Theme 3: Physicians’ Management of Clinical Information
Physicians’ management of clinical information associated with ordering clinical laboratory and radiology tests and viewing test results was observed to be complex. An interesting phenomenon was the use of paper memory aides by hematology ward physicians from both hospitals to record diagnostic test information. These were carried by physicians in their pockets and consisted of patient lists (which were usually printed from the CPOE system, although one physician used a black book which he wrote in) against which they recorded key laboratory test results, transcribed from the CPOE system, and specialist’s instructions given during ward rounds, such as further tests required. The paper memory aides were generally updated daily with a new patient list being printed from the system by the physician. These paper aids were referred to by the junior physicians during ward rounds when the senior specialists asked questions regarding test results for their patients. They were destroyed every few days when a new list was printed. One physician commented that they could also be referred to at home if junior physicians thought they had forgotten something or, if they remembered something that they should have done, they could note it on the paper memory aide to be followed up the next day.
Multiple sources for accessing clinical information were used, both computerized and manual, with resultant duplication of recording of clinical information. Some physicians relied entirely on the CPOE for test ordering and results viewing. Some wrote abnormal test results in the paper medical record, transcribed from the computerized system, and others did not, claiming that it defeated the purpose of the system. In the EDs there was a ‘stand alone’ information system and a whiteboard that were also used to record clinical information. In addition information was accessed from manual documents such as medication handbooks and clinical guidelines. Physicians could therefore record information in the CPOE system, the manual hospital medical record, the Emergency Department information system, the whiteboard and on paper memory aides. They could obtain information from those same sources as well as their colleagues and paper based sources such as the Oxford Handbook of Medicine. Given the multiple media used to record information there were numerous duplications. In the ED at Hospital B one physician wrote a manual x-ray order form, wrote the order in the medical record in two locations and wrote it on the whiteboard. Some abnormal laboratory results were phoned through to the ED at Hospital A as well as being reported electronically and urgent CT scans were ordered over the phone as well as being placed on the computer.
Comments and observations represented by this theme were assigned the following descriptive categories during the coding process: (1) multiple information sources; (2) duplication of information; and (3) paper memory aides. Representative observations or quotes from the interviews are shown in ▶.
Table 3.
Table 3. Theme 3—Physicians’ Management of Clinical Information: Representative Observations and Quotations from Interviews
| Categories | Observation or Quotation |
|---|---|
| Category 1: Multiple information sources | “She writes in the notes of the bed 1 patient. Goes to the whiteboard and rubs out some of the things next to the bed 7 patient … then she goes to see the patient in bed 7 … comes back … gets the bed 7 medication charts … gets MIMS and looks up the medication, continues writing in medication chart … uses Powerchart ∗ to view results … writes in notes … uses HAS for patient 1 and enters the diagnosis … writes a script for bed 1 patient and prints a discharge letter.” [Hospital B ED observation] |
| Category 2: Duplication of information | “Between the medical record, Powerchart ∗ and memory aides there is duplication of information and duplication of effort.” [Hospital A hematology ward observation] |
| “Transcribing test results from Powerchart ∗ into the medical record.” [Hospital B ED observation] | |
| “Nurses check results and document in notes if abnormal result. There is discussion about whether to document in notes—some see it as duplication as everything is supposed to be in Powerchart ∗ whereas I think the abnormal results should be documented.” [Hospital B ED nurse interview] | |
| Category 3: Paper memory aides | “I use the patient list because I can look quickly if a consultant asks me a question, and I can look at home if wanting to check something.” [Hospital A hematology physician interview] |
| “It reminds me of the patients I am looking after and I can make notes during ward rounds.” [Hospital A hematology physician interview] | |
| “Don’t need memory aides in ED as they diagnose, treat and transfer quickly.” [Hospital A ED observation] |
∗ Powerchart is the application name of the test management software.
Abbreviations: HAS = Emergency Department ‘stand alone’ information system; ED = Emergency Department.
Discussion
This study provided a deep understanding of physicians’ established use of CPOE systems. The results indicated that physicians’ work practices are affected in a number of ways. A key finding was the impact of the hospital and clinical unit on test management work practices. There were differences in attitudes to computerized test ordering, how and when tests were ordered and whether ordering was completed as a team activity or not depending on the hospital and clinical unit. These environmental differences need to be acknowledged and accommodated for safe and efficient use of CPOE. Another key finding relates to the hybrid information environment in hospitals and how CPOE fits within this environment. Currently health facilities are in an information system transition phase, where both manual and computerized clinical and administrative systems are being used. This mixed media information environment can give rise to duplications in recording clinical information, missed information and/or a lack of permanent documentation for future care, all of which can impact on patient safety and physicians’ efficiency.
Test Management Work Practices in Different Clinical Environments
No previous study has looked at CPOE use in different clinical environments. Our study showed that different clinical environments between the EDs and the hematology wards affected who ordered clinical laboratory and radiology tests, how they were ordered (individual physicians for one patient or a team of physicians for multiple patients) and where they preferred to order (at the bedside or the nurse station). The environment in the ED creates unique demands on a computerized test ordering system, most particularly the interruptive nature of clinical communication in this setting resulting from the diversity in patient type, presentation and treatments. 4,7,52,53 The complexities of ED environments are reflected in the comment by an Emergency Department physician that “many EDs even on a good day are dysfunctional.” 54 A number of previous studies have emphasized the importance of ‘fit’ between the technology and work practices. 1,3,17,25,55–57 Our study has shown that this ‘fit’ between CPOE and work practices will also vary depending on the clinical environment.
Physicians in our study were aware of the divergent needs that each department may have in relation to their use of CPOE. Other studies have shown the advantages of customizing test management systems to suit the needs of the hospital and/or clinical department. 38,58,59 Taking advantage of the flexibility of information systems to respond to the requirements of the users and the environment is important to enable physicians to see value in clinical information systems for their patient care practices.
There have been few studies that have explored whether differences between hospitals impact on the uptake of point of care clinical information systems. 28,38,43 Ash and her colleagues 38 found that teaching and non-teaching hospital differences which were most likely to impact on the implementation of systems related to the extent of collaboration between staff, staff longevity and organizational missions. The respondents in the non-teaching hospital in that study indicated that they had high levels of interdisciplinary collaboration whereas in the teaching hospital they had separate physicians’ and nurses’ order sets. 38 We found a similar result in our study with different order sets between the two hospital EDs and different roles in test ordering between physicians and nurses. Our study extended the work of Ash and her colleagues, 38 by also exploring variation in the use of CPOE between different clinical units within teaching hospitals.
Our results showed that diversity between hospitals and clinical units affected how physicians and nurses order tests and suggest that these differences need to be taken into account when implementing CPOE systems within those environments. This study has highlighted two key lessons to assist future implementations of CPOE. Firstly, implementation teams must acknowledge the diversity between hospitals and clinical units and take these differences into account in all clinical information system implementation projects. The IT implementation team should explore the requirements of individual clinical units pre-implementation to enable them to prepare. During the implementation there needs to be a focus on clinical unit differences which can be accommodated within the functionality of the clinical information system. Clinical information system developers could be included in this process of modifications to functionality of their systems. Secondly, there needs to be a focus on the users of the systems and their requirement to use the technology to improve rather than duplicate their work practices to optimize patient care. For acceptance and usage of clinical information systems to grow it is important for health professionals to see improvements to the care of their patients rather than simply administrative efficiencies. Therefore opportunities to realize the value of clinical information systems to physicians should be identified, trialed and implemented to maximize their use. Organizational analyses should be undertaken when planning an implementation to acknowledge and enable those differences to be accommodated when designing or modifying the information system and training the users. Implementation of any clinical information system involves continual monitoring and adjustment to meet the changing needs of the users within their organizational and departmental contexts.
The Management of Clinical Information
In our study physicians’ management of information associated with clinical laboratory and radiology test ordering and results viewing was observed to be complex with multiple sources and mediums used for retrieving and recording information. Apart from the concern of duplication in recording information when multiple media are used, there is a risk that something could be missed if information about a patient is not recorded in one agreed location, regardless of whether that location is computerized or manual. This is the basis of the health information management principle of a unit record system. 60,61 In a unit record system all clinical and demographic information regarding one patient from the one facility, whether as an inpatient or outpatient, is stored in the same medium at the same location and in that way health professionals can be reasonably assured that no information regarding the patient’s episodes of care at the facility is missed. Many organizations need to confront this mixed-media environment which is often viewed as being transitory but which in fact can last for long periods of time as organizations convert between paper and computerized systems. The literature examining the impact of this situation is virtually nonexistent yet may potentially have important implications for safety. In addition it may be during this phase that physicians are more likely to develop workarounds with the idea that existing problems will be fixed once the full transition to the computerized system has occurred.
Studies that have compared paper-based and computerized patient records have found that the parallel use of computerized and paper clinical information can lead to inconsistencies in medical documentation. 62,63 In the current composite information media environment, one needs to reconsider the unit record principle to ensure that duplications are minimized and errors due to multiple information storage mediums reduced. Patel and her colleagues 64 found that when comparing paper based and computerized medical records, the two media emphasized the recording of different types of information and use of computerized patient records impacted not only what information was recorded, but how the information was organized in terms of structure and style. This demonstrates how technology and the practice supported by the technology can be transformed and that the implementation of an information system is a process of mutual shaping. 55
The observations in our study regarding the multiple information media and complexity of interactions of physicians with these tools support the sociological perspective of medical work as put forward by Berg. 2 Medical work is complicated and iterative and “does not proceed in clear-cut cycles of data gathering, hypothesis testing, therapy, and evaluation.” 2 In our study, we observed an intricate interplay of different information storage and retrieval media and we noticed that none of the physicians and nurses who we interviewed commented that this made their work messy and complex. They all appeared to work with the heterogeneous set of tools for storing and retrieving information. Gorman and his colleagues described “how experts create and use bundles which are highly selective collections of information—to help solve problems and maintain situation awareness.” 65 He concluded that these bundles were useful in complex environments, to support information management for multiple, diverse, complex, and simultaneous tasks. In our study we observed that physicians found their own way of working with the test management technology and their colleagues in their respective environments. The use of paper memory aides by most junior physicians in the hematology wards showed the need for physicians to have information readily available and also a memory aide if they are managing a large number of patients. It also demonstrated how work is extending beyond the boundaries of the hospital with the memory aides being used at home to note important thoughts down for work the next day.
It is important to interpret these results in light of the study limitations. The research was conducted in two hospitals of a similar category and in only two different types of clinical units and therefore the results may only be generalizable to similar large metropolitan teaching hospitals and similar ED and hematology units. The selection of participants was purposive rather than random however this conforms to qualitative research conventions. 66
Conclusion
This study has shown the long-term effects of the mandatory use of CPOE on physicians’ test management work practices. After a decade of CPOE use changes to the way physicians order clinical diagnostic and radiology tests and view results are dependent upon the hospital and the clinical unit environment. Analyses of physicians’ work practices need to be undertaken prior to implementation of clinical information systems to accommodate physicians’ diverse ways of using information systems. The implementation of computerized point of care clinical information systems move health care facilities further along the continuum from manual to computerized information systems. This creates a hybrid information media environment for recording and accessing clinical and administrative information about patients. This can lead to duplications and missed information about patients with possible risks to patient safety. Further studies need to be undertaken to explore how clinical information systems are being used at the ‘coalface’ to ensure their safe and efficient use.
Footnotes
The authors thank Nerida Creswick BAppSc (HIM) Hons for her assistance in data collection and field work for this study.
Australia has a universal health insurance system similar to those in Canada and the United Kingdom. Public hospitals provide the majority of inpatient care and many privately insured patients are also treated in the public hospital system.
References
- 1.Berg M. Patient care information systems and health care work: a sociotechnical approach Int J Med Inf 1999;55:87-101. [DOI] [PubMed] [Google Scholar]
- 2.Berg M. Medical work and the computer-based patient record: a sociological perspective Methods Inf Med 1998;37:294-301. [PubMed] [Google Scholar]
- 3.Berg M, Langenberg C, Berg IVD, Kwakkernaat J. Considerations for sociotechnical design: experiences with an electronic patient record in a clinical context Int J Med Inf 1998;52:243-251. [DOI] [PubMed] [Google Scholar]
- 4.Coiera E, Jayasuriya RA, Hardy J, Bannan A, Thorpe MEC. Communication loads on clinical staff in the emergency department MJA 2002;176:415-418. [DOI] [PubMed] [Google Scholar]
- 5.Coiera E, Toombs V. Communication behaviours in a hospital setting; an observational study BMJ 1998;316:673-676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gosbee J. Communication among health professionals BMJ 1998;316:642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Spencer R, Logan P. Role-based communication patterns within an emergency department setting HIC 2002;10:53-54. [Google Scholar]
- 8.Overhage M, Tierney W, Zhou A, McDonald C. A randomized trial of “corollary orders” to prevent errors of omission J Am Med Inform Assoc 1997;4:364-375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bates DW, Kuperman GJ, Rittenberg E, et al. A randomized trial of a computer-based intervention to reduce utilization of redundant laboratory tests Am J Med 1999;106:144-150. [DOI] [PubMed] [Google Scholar]
- 10.Committee on Quality of Health Care in America Crossing the quality chasm: a new health system for the 21st century. Washington DC: Institute of Medicine, National Academy Press; 2001.
- 11.Teich JM, Merchia PR, Schmiz JL, Kuperman GJ, Spurr CD, Bates DW. Effect of computerized physician order entry on prescribing practices Arch Intern Med 2000;160:2741-2747. [DOI] [PubMed] [Google Scholar]
- 12.Bates DW, Cohen M, Leape LL, Overhage JM, Shabot MM, Sheridan T. Reducing the frequency of errors in medicine using information technology J Am Med Inform Assoc 2001;8:299-308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dexter PR, Perkins S, Overhage JM, Maharry K, Kohler RB, McDonald CJ. A computerized reminder system to increase the use of preventive care for hospitalized patients N Eng J Med 2001;345:965-970. [DOI] [PubMed] [Google Scholar]
- 14.Ash JS, Berg M, Coiera E. Some unintended consequences of information technology in health care: the nature of patient care information system-related errors J Am Med Inform Assoc 2004;11:104-112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fonkych K, Taylor R. The state and pattern of health information technology adoption. Rand Corporation; 2005. Available at: http://www.rand.org/ .
- 16.Guise DA, Kuhn KA. Health information systems challenges: the Heidelberg conference and the future Int J Med Inf 2003;69:105-114. [DOI] [PubMed] [Google Scholar]
- 17.Massaro TA. Introducing physician order entry at a major academic medical center: impact on organizational culture and behavior Acad Med 1993;68:20-25. [DOI] [PubMed] [Google Scholar]
- 18.Ash J. Organizational factors that influence information technology diffusion in academic health sciences centers J Am Med Inform Assoc 1997;4:102-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ash JS, Gorman PN, Hersh WR, Lavelle M, Poulsen SB. Perceptions of house officers who use physician order entry Proc AMIA Symp 1999:471-475. [PMC free article] [PubMed]
- 20.Ash JS, Lyman J, Carpenter J, Fournier L. A diffusion of innovations model of physician order entry Proc AMIA Symp 2001:22-26. [PMC free article] [PubMed]
- 21.Gorman PN, Lavelle MB, Ash JS. Order creation and communication in healthcare Methods Inf Med 2003;42:376-384. [PubMed] [Google Scholar]
- 22.Ash JS, Sittig DF, Seshadri V, Dykstra RH, Carpenter JD, Stavri PZ. Adding insight: a qualitative cross-site study of physician order entry Medinfo 2004;11:1013-1016. [PubMed] [Google Scholar]
- 23.Lorenzi NM, Riley RT, Blyth AJC, Southon G, Dixon BJ. Antecedents of the people and organizational aspects of medical informatics: a review of the literature J Am Med Inform Assoc 1997;4:79-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kaplan B. Addressing organizational issues into the evaluation of medical systems J Am Med Inform Assoc 1997;4:94-101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ahmad A, Teater P, Bentley TD, et al. Key attributes of a successful physician order entry system implementation in a multi-hospital environment J Am Med Inform Assoc 2002;9:16-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ash JS, Fournier L, Stavri PZ, Dykstra R. Principles for a successful computerized physician order entry implementation Proc AMIA Symp 2003:36-40. [PMC free article] [PubMed]
- 27.Ash JS, Gorman PN, Lavelle M, et al. Perceptions of physician order entry: results of a cross-site qualitative study Methods Inf Med 2003;42:313-323. [PubMed] [Google Scholar]
- 28.Aarts J, Berg M. A tale of two hospitals: a sociotechnical appraisal of the introduction of computerised physician order entry into two Dutch hospitals Medinfo 2004;11:999-1002. [PubMed] [Google Scholar]
- 29.Creswick N, Callen J. What do doctors, senior managers and IT professionals perceive to be the key factors in the use of clinical information systems? HIC, Health Informatics Society of Australia 2002;10:22-23. [Google Scholar]
- 30.Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors JAMA 2005;293:1197-1203. [DOI] [PubMed] [Google Scholar]
- 31.Georgiou A, Westbrook JI, Braithwaite J, Iedema R. Multiple perspectives on the impact of electronic ordering on hospital organizational and communication processes Health Inf Manag 2005;34:130-135. [DOI] [PubMed] [Google Scholar]
- 32.Georgiou A, Westbrook J, Braithwaite J, Iedema R, Dimos A, Germanos T. A context-mechanism-outcome approach to the evaluation of computerised physician order entry systems HIC, Health Informatics Society of Australia 2005;13:1-6. [Google Scholar]
- 33.Garg AX, Adhikari NKJ, McDonald H, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomesA systematic review. J Am Med Inform Assoc 2005;293:1223-1238. [DOI] [PubMed] [Google Scholar]
- 34.Berger RG, Kichak JP. Computerized physician order entry: helpful or harmful?(2004) J Am Med Inform Assoc 2004;11:100-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ammenwerth E, Brender J, Nykanen P, Prokosch HU, Rigby M, Talmon J. Visions and strategies to improve evaluation of health information systemsReflections and lessons based on the HIS-EVAL workshop in Innsbruck. Int J Med Inf 2004;73:479-491. [DOI] [PubMed] [Google Scholar]
- 36.Stoop AP, Berg M. Integrating quantitative and qualitative methods in patient care information system evaluation: guidance for the organisational decision maker Methods Inf Med 2003;42:458-462. [PubMed] [Google Scholar]
- 37.Ammenwerth E, Graber S, Herrmann G, Burkle T, Konig J. Evaluation of health information systems—problems and challenges Int J Med Inf 2003;71:125-135. [DOI] [PubMed] [Google Scholar]
- 38.Ash JS, Gorman PN, Lavelle M, et al. A cross site qualitative study of physician order entry J Am Med Inform Assoc 2003;10:188-200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kaplan B. Evaluating informatics applications – some alternative approaches: theory, social interactionism, and call for methodological pluralism Int J Med Inf 2001;64:39-55. [DOI] [PubMed] [Google Scholar]
- 40.reatbatch D, Murphy E, Dingwall R. Evaluating medical information systems: ethnomethodological and interactionist approaches Health Serv Mngt Res 2001;14:181-191. [DOI] [PubMed] [Google Scholar]
- 41.Kaplan B, Maxwell JA. Qualitative research methods for evaluating computer information systemsIn: Anderson JG, Aydin CE, Jay SJ, editors. Evaluating health care information systems: methods and applications. London: Sage Publications; 1994. pp. 45-68.
- 42.Kaplan B, Duchon D. Combining qualitative and quantitative methods in information systems research: a case study MIS Q 1988:571-586.
- 43.Gosling AS, Westbrook JI, Coiera EW. Variation in the use of online clinical evidence: a qualitative analysis Int J Med Inf 2003;69:1-16. [DOI] [PubMed] [Google Scholar]
- 44.Charmaz K. Grounded theory: objectivist and constructivist methodsIn: Denzin NK, Lincoln YS, editors. Strategies of qualitative inquiry. (2nd Ed.). London: Sage Publications; 2003.
- 45.Yin RK. Case study research: design and methods. 2nd Ed. California: Sage Publications; 1994.
- 46.Glaser BG, Strauss AL. The discovery of grounded theory: strategies for qualitative research. Chicago: Aldine; 1967.
- 47.Guba E, Lincoln. Fourth generation evaluation. Newbury Park: Sage Publications; 1989. pp. 228-243.
- 48.Gifford S. Qualitative research: the soft option? Health Prom J Austr 1996;6:58-61. [Google Scholar]
- 49.Ritchie J. In: Berglund C, editor. Health research. Melbourne: Oxford University Press; 2000. pp. 275-282.
- 50.Mays N, Pope C. Assessing quality in qualitative research BMJ 2000;320:50-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Barbour RS. Checklists for improving rigour in qualitative research: a case of the tail wagging the dog? BMJ 2001;322:1115-1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Teich JM. Information systems support for emergency medicine Acad Emerg Med 1997;5:271-274. [DOI] [PubMed] [Google Scholar]
- 53.Chisholm CD, Edgar K, Collision BA, Nelson DR, Cordell WH. Emergency department workplace interruptions: are emergency physicians “interrupt-driven” and “multitasking”? Acad Emerg Med 2000;7:1239-1243. [DOI] [PubMed] [Google Scholar]
- 54.Taylor TB. Information management in the emergency department Emerg Med Clinics Nth Am 2004;22:241-257. [DOI] [PubMed] [Google Scholar]
- 55.Aarts J, Doorewaard H, Berg M. Understanding implementation: the case of a computerized physician order entry system in a large Dutch university medical center J Am Med Inform Assoc 2004;11:207-216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ash JS, Stavri PZ, Kuperman GJ. A consensus statement on considerations for successful CPOE implementation J Am Med Inform Assoc 2003;10:229-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Berg M, Toussaint P. The mantra of modeling and the forgotten powers of paper: a sociotechnical view on the development of process-oriented ICT in healthcare Int J Med Inf 2003;69:223-234. [DOI] [PubMed] [Google Scholar]
- 58.Payne TH, Hoey PJ, Nichol P, Lovis C. Preparation and use of preconstructed orders, order sets, and order menus in a computerized provider order entry system J Am Med Inform Assoc 2003;10:322-329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Schuster DM, Hall SE, Couse CB, Swayngim DS, Kohatsu KY. Involving users in the implementation of an imaging order entry system J Am Med Inform Assoc 2003;10:315-321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Huffman EK. Health information management. Illinois: Physicians’ Record Company; 1994.
- 61.Abdelhak M. Health information: management of a strategic resource. (2nd ed.). Philadelphia: WB Saunders Company; 2001.
- 62.Stausberg J, Koch D, Ingenerf J, Betzler M. Comparing paper-based with electronic patient records: lessons learned during a study on diagnosis and procedure codes J Am Med Inform Assoc 2003;10:470-477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Mikkelsen G, Aasly J. Concordance of information in parallel electronic and paper based patient record Int J Med Inf 2000;63:123-131. [DOI] [PubMed] [Google Scholar]
- 64.Patel VL, Kushniruk AW, Yang S, Yale JF. Impact of a computer-based patient record system on data collection, knowledge organization, and reasoning J Am Med Inform Assoc 2000;7:569-585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Gorman P, Ash J, Lavelle M, et al. Bundles in the wild: managing information to solve problems and maintain situation awareness Lib Trends 2000;49:266-283. [Google Scholar]
- 66.Sittig DF, Krall M, Kaalaas-Sittig J, Ash JS. Emotional aspects of computer-based physician order entry: a qualitative study J Am Med Inform Assoc 2005;12:561-567. [DOI] [PMC free article] [PubMed] [Google Scholar]