

Abstract
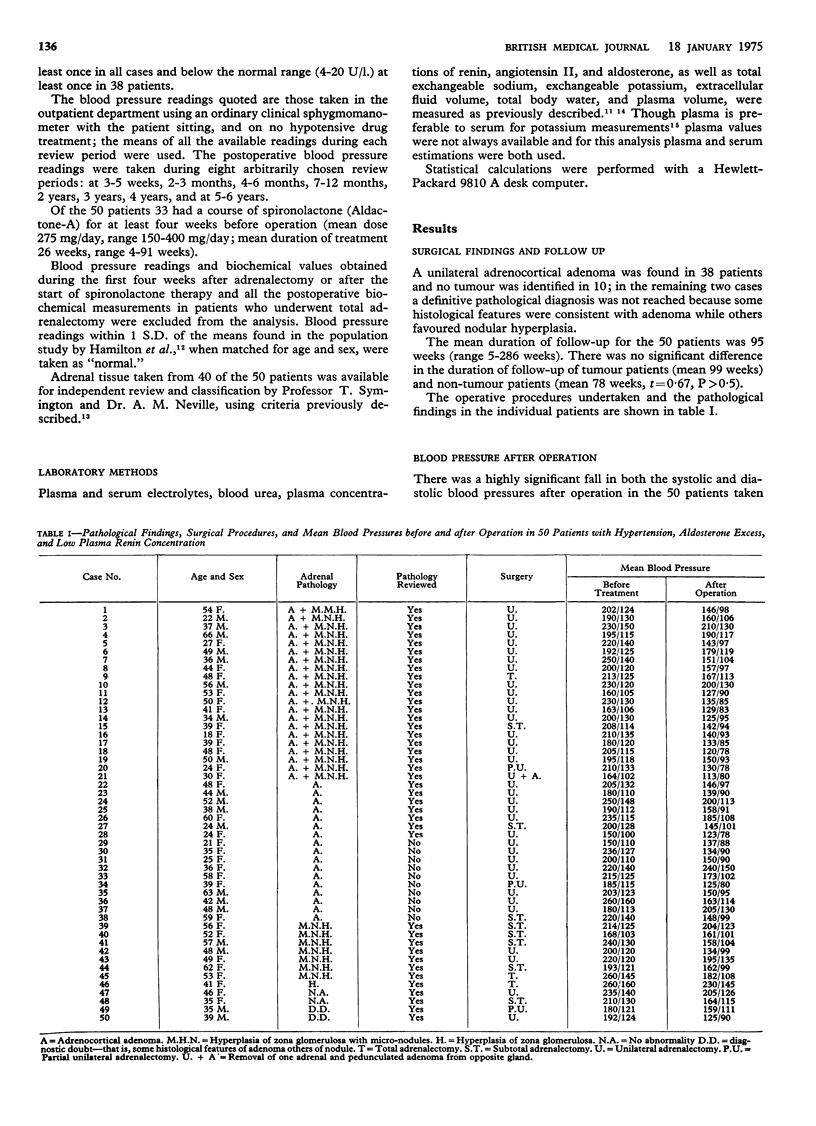
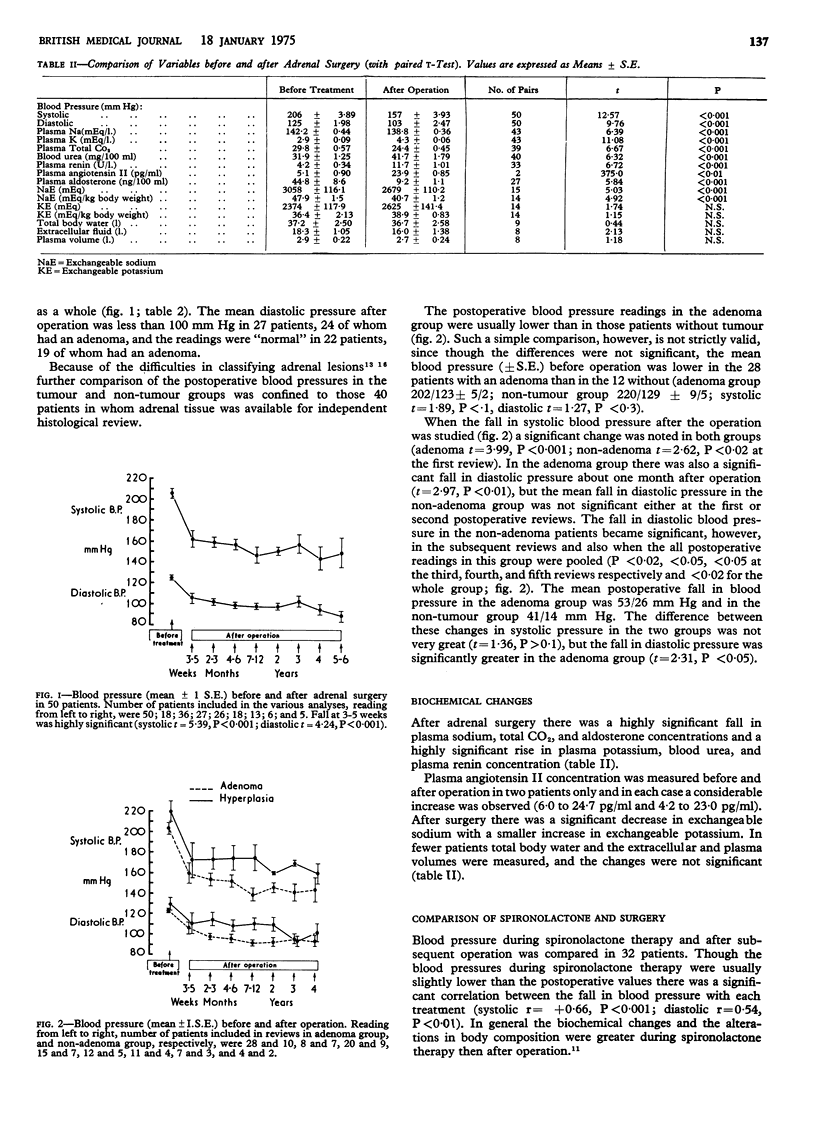
Fifty patients with hypertension, aldosterone excess, and low plasma renin concentration underwent adrenal surgery. There was a highly significant fall in mean systolic and diastolic pressures after the operation. The mean postoperative diastolic pressure fell to strictly normal levels, however, in only 19 out of 38 patients from whom an adrenocortical adenoma was removed and in only two out of 10 non-tumour patients. There was a significant correlation between the fall in blood pressure during spironolactone treatment and after adrenal surgery though levels were generally slightly lower during the former therapy. It is suggested that removal of an aldosterone-producing adenoma is the treatment of choice provided a good preoperative hypotensive response to spironolactone occurs, while the treatment of choice for non-tumour patients is often long-term spironolactone.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aitchison J., Brown J. J., Ferriss J. B., Fraser R., Kay A. W., Lever A. F., Neville A. M., Symington T., Robertson J. I. Quadric analysis in the preoperative distinction between patients with and without adrenocortical tumors in hypertension with aldosterone excess and low plasma renin. Am Heart J. 1971 Nov;82(5):660–671. doi: 10.1016/0002-8703(71)90336-x. [DOI] [PubMed] [Google Scholar]
- Barr R. D., McCulloch P. B., Mehta S., Kendall A. G. Acute leukaemia in Kenya. Scott Med J. 1972 Oct;17(10):330–333. doi: 10.1177/003693307201701004. [DOI] [PubMed] [Google Scholar]
- Brown J. J., Chinn R. H., Davies D. L., Fraser R., Lever A. F., Rae R. J., Robertson J. I. Falsely high plasma potassium values in patients with hyperaldosteronism. Br Med J. 1970 Apr 4;2(5700):18–20. doi: 10.1136/bmj.2.5700.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CONN J. W., KNOPF R. F., NESBIT R. M. CLINICAL CHARACTERISTICS OF PRIMARY ALDOSTERONISM FROM AN ANALYSIS OF 145 CASES. Am J Surg. 1964 Jan;107:159–172. doi: 10.1016/0002-9610(64)90252-1. [DOI] [PubMed] [Google Scholar]
- Conn J. W., Morita R., Cohen E. L., Beierwaltes W. H., McDonald W. J., Herwig K. R. Primary aldosteronism. Photoscanning of tumors after administration of 131 I-19-iodocholesterol. Arch Intern Med. 1972 Mar;129(3):417–425. doi: 10.1001/archinte.129.3.417. [DOI] [PubMed] [Google Scholar]
- Conn J. W. The evolution of primary aldosteronism: 1954-1967. Harvey Lect. 1966;62:257–291. [PubMed] [Google Scholar]
- Davies D. L., Robertson J. W. Simultaneous measurement of total exchangeable potassium and sodium using 43 K and 24 Na. Metabolism. 1973 Feb;22(2):133–137. doi: 10.1016/0026-0495(73)90263-1. [DOI] [PubMed] [Google Scholar]
- Ferriss J. B., Brown J. J., Fraser R., Kay A. W., Neville A. M., O'Muircheartaigh I. G., Robertson J. I., Symington T., Lever A. F. Hypertension with aldosterone excess and low plasma-renin: preoperative distinction between patients with and without adrenocortical tumour. Lancet. 1970 Nov 14;2(7681):995–1000. doi: 10.1016/s0140-6736(70)92811-4. [DOI] [PubMed] [Google Scholar]
- George J. M., Wright L., Bell N. H., Bartter F. C. The syndrome of primary aldosteronism. Am J Med. 1970 Mar;48(3):343–356. doi: 10.1016/0002-9343(70)90065-3. [DOI] [PubMed] [Google Scholar]
- Kahn P. C., Kelleher M. D., Egdahl B. H., Melby J. C. Adrenal arteriography and venography in primary aldosteronism. Radiology. 1971 Oct;101(1):71–78. doi: 10.1148/101.1.71. [DOI] [PubMed] [Google Scholar]
- Katz F. H. Primary aldosteronism with suppressed plasma renin activity due to bilateral nodular adrenocortical hyperplasia. Ann Intern Med. 1967 Nov;67(5):1035–1042. doi: 10.7326/0003-4819-67-5-1035. [DOI] [PubMed] [Google Scholar]
- Kawasaki T., Omae T., Tanaka K., Matsunage M., Emoto K. Remission or recurrent hyperaldosteronism resulting from subtotal adrenalectomy of adenomatous hyperplastic adrenal glands. J Clin Endocrinol Metab. 1971 Sep;33(3):474–480. doi: 10.1210/jcem-33-3-474. [DOI] [PubMed] [Google Scholar]
- Ledingham J. G., Laragh J. H., Sommers S. C. Secondary aldosteronism and reduced plasma renin in hypertensive disease. Trans Assoc Am Physicians. 1967;80:168–182. [PubMed] [Google Scholar]
- Melby J. C., Spark R. F., Dale S. L., Egdahl R. H., Kahn P. C. Diagnosis and localization of aldosterone-producing adenomas by adrenal-vein cateterization. N Engl J Med. 1967 Nov 16;277(20):1050–1056. doi: 10.1056/NEJM196711162772002. [DOI] [PubMed] [Google Scholar]
- Neville A. M., Symington T. Pathology of primary aldosteronism. Cancer. 1966 Dec;19(12):1854–1868. doi: 10.1002/1097-0142(196612)19:12<1854::aid-cncr2820191213>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- Rhamy R. K., McCoy R. M., Scott H. W., Jr, Fishman L. M., Michelakis A. M., Liddle G. W. Primary aldosteronism: experience with current diagnostic criteria and surgical treatment in fourteen patients. Ann Surg. 1968 May;167(5):718–727. doi: 10.1097/00000658-196805000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spark R. F., Melby J. C. Aldosteronism in hypertension. The spironolactone response test. Ann Intern Med. 1968 Oct;69(4):685–691. doi: 10.7326/0003-4819-69-4-685. [DOI] [PubMed] [Google Scholar]