

Abstract
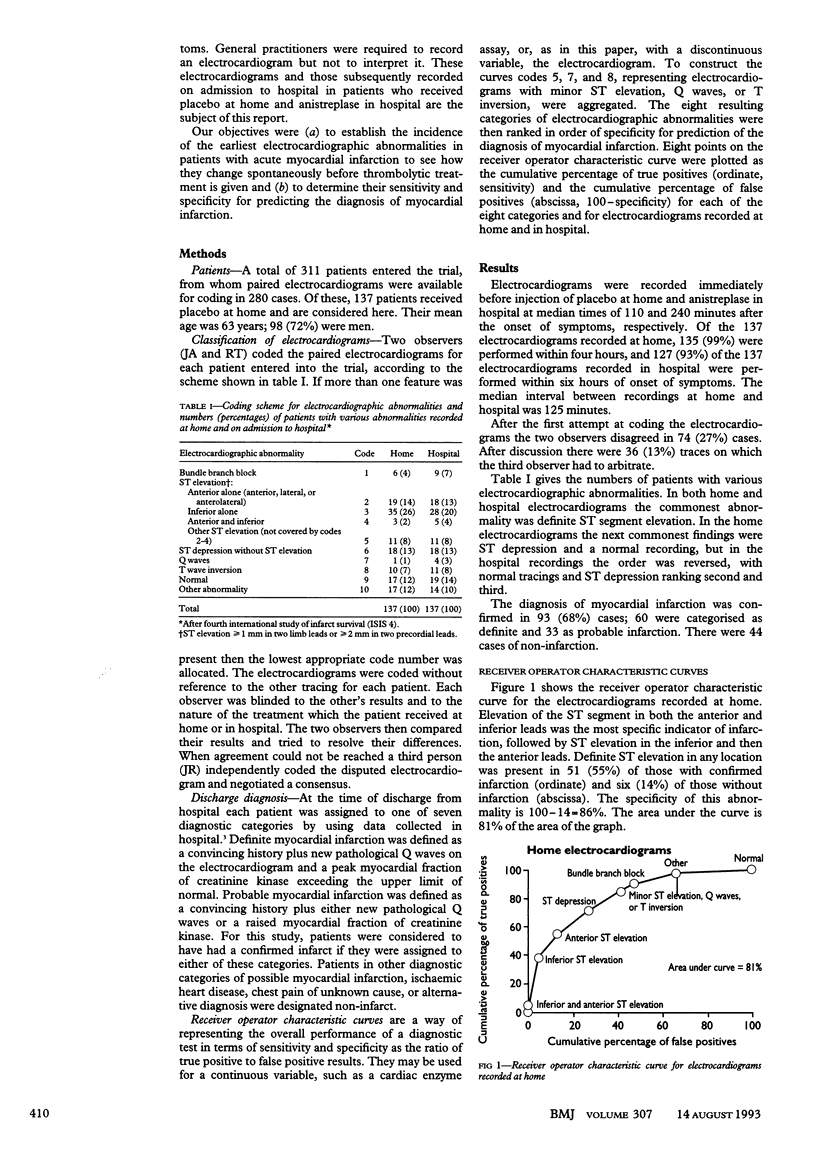
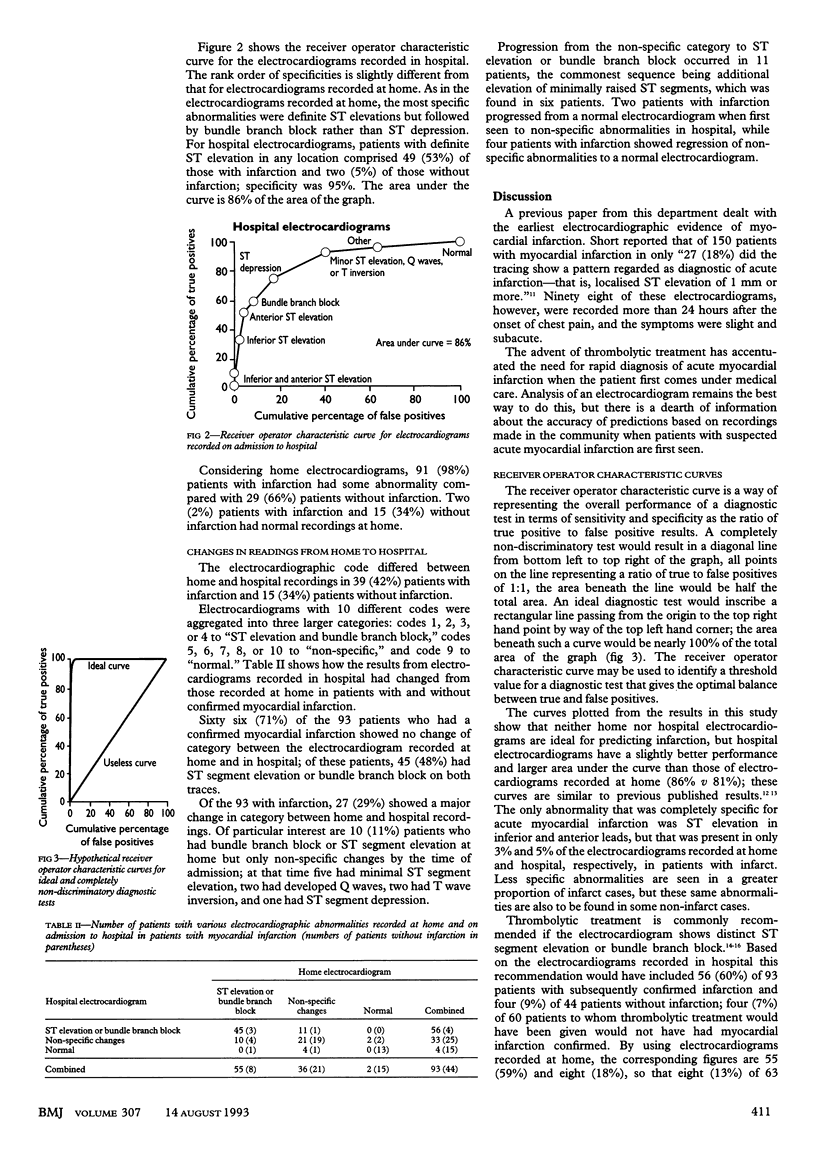
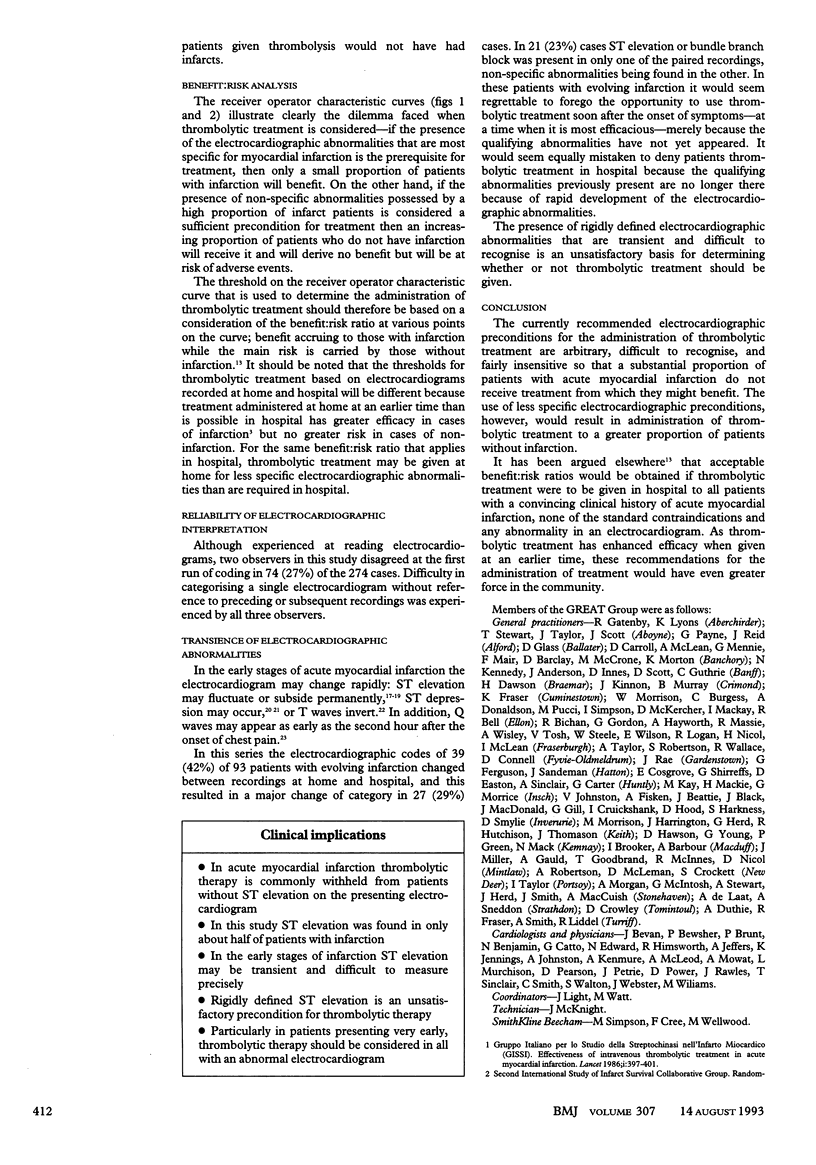
OBJECTIVES--To determine the incidence of the earliest electrocardiographic changes in patients with suspected myocardial infarction and their sensitivity and specificity for predicting the final diagnosis of acute myocardial infarction. DESIGN--Retrospective study of paired electrocardiograms recorded at home and on admission to hospital. SETTING--29 rural practices in Grampian and teaching hospitals in Aberdeen. PATIENTS--137 patients participating in the early anistreplase trial in the Grampian region, who received placebo at home and for whom paired electrocardiograms were available. MAIN OUTCOME MEASURES--Classified electrocardiographic abnormalities and diagnosis at discharge. RESULTS--Electrocardiograms were recorded immediately before injection of placebo at home and anistreplase in hospital at median times of 110 and 240 minutes after the onset of symptoms. Definite or probable myocardial infarction was later confirmed in 93 (68%) patients. Of these, 66 (71%) had the same findings on both electrocardiograms of either ST elevation, bundle branch block, or a non-specific abnormality, while 27 (29%) showed a major change of classification between home and hospital recordings; 21 (23%) had ST elevation or bundle branch block on only one of the paired recordings. Although ST elevation was the commonest abnormality in the 93 patients with myocardial infarction, in only 51 was it recorded at home (sensitivity 55%) and in 49 on admission (sensitivity 53%). Of 57 patients with ST elevation at home, six did not have infarction (specificity 86%), while of 51 with ST elevation on admission, two did not have infarction (specificity 95%). CONCLUSIONS--Elevation of the ST segment is a transient electrocardiographic abnormality that has high specificity but low sensitivity for predicting the diagnosis of acute myocardial infarction; it is an unsatisfactory precondition for giving thrombolytic treatment to patients with suspected acute myocardial infarction.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Baughman K. L., Maroko P. R., Vatner S. F. Effects of coronary artery reperfusion on myocardial infarct size and survival in conscious dogs. Circulation. 1981 Feb;63(2):317–323. doi: 10.1161/01.cir.63.2.317. [DOI] [PubMed] [Google Scholar]
- Bergmann S. R., Lerch R. A., Fox K. A., Ludbrook P. A., Welch M. J., Ter-Pogossian M. M., Sobel B. E. Temporal dependence of beneficial effects of coronary thrombolysis characterized by positron tomography. Am J Med. 1982 Oct;73(4):573–581. doi: 10.1016/0002-9343(82)90338-2. [DOI] [PubMed] [Google Scholar]
- Brush J. E., Jr, Brand D. A., Acampora D., Chalmer B., Wackers F. J. Use of the initial electrocardiogram to predict in-hospital complications of acute myocardial infarction. N Engl J Med. 1985 May 2;312(18):1137–1141. doi: 10.1056/NEJM198505023121801. [DOI] [PubMed] [Google Scholar]
- Essen R., Merx W., Effert S. Spontaneous course of ST-segment elevation in acute anterior myocardial infarction. Circulation. 1979 Jan;59(1):105–112. doi: 10.1161/01.cir.59.1.105. [DOI] [PubMed] [Google Scholar]
- Gibson R. S., Crampton R. S., Watson D. D., Taylor G. J., Carabello B. A., Holt N. D., Beller G. A. Precordial ST-segment depression during acute inferior myocardial infarction: clinical, scintigraphic and angiographic correlations. Circulation. 1982 Oct;66(4):732–741. doi: 10.1161/01.cir.66.4.732. [DOI] [PubMed] [Google Scholar]
- Klainman E., Sclarovsky S., Lewin R. F., Topaz O., Farbstein H., Pinchas A., Fohoriles L., Agmon J. Natural course of electrocardiographic components and stages in the first twelve hours of acute myocardial infarction. J Electrocardiol. 1987 Apr;20(2):98–109. doi: 10.1016/s0022-0736(87)80098-5. [DOI] [PubMed] [Google Scholar]
- Lee T. H., Rouan G. W., Weisberg M. C., Brand D. A., Cook E. F., Acampora D., Goldman L. Sensitivity of routine clinical criteria for diagnosing myocardial infarction within 24 hours of hospitalization. Ann Intern Med. 1987 Feb;106(2):181–186. doi: 10.7326/0003-4819-106-2-181. [DOI] [PubMed] [Google Scholar]
- Quyyumi A. A., Crake T., Rubens M. B., Levy R. D., Rickards A. F., Fox K. M. Importance of "reciprocal" electrocardiographic changes during occlusion of left anterior descending coronary artery. Studies during percutaneous transluminal coronary angioplasty. Lancet. 1986 Feb 15;1(8477):347–350. doi: 10.1016/s0140-6736(86)92317-2. [DOI] [PubMed] [Google Scholar]
- Reid D. S., Pelides L. J., Shillingford J. P. Surface mapping of RS-T segment in acute myocardial infarction. Br Heart J. 1971 May;33(3):370–374. doi: 10.1136/hrt.33.3.370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rouan G. W., Lee T. H., Cook E. F., Brand D. A., Weisberg M. C., Goldman L. Clinical characteristics and outcome of acute myocardial infarction in patients with initially normal or nonspecific electrocardiograms (a report from the Multicenter Chest Pain Study). Am J Cardiol. 1989 Nov 15;64(18):1087–1092. doi: 10.1016/0002-9149(89)90857-6. [DOI] [PubMed] [Google Scholar]
- Rude R. E., Poole W. K., Muller J. E., Turi Z., Rutherford J., Parker C., Roberts R., Raabe D. S., Jr, Gold H. K., Stone P. H. Electrocardiographic and clinical criteria for recognition of acute myocardial infarction based on analysis of 3,697 patients. Am J Cardiol. 1983 Nov 1;52(8):936–942. doi: 10.1016/0002-9149(83)90508-8. [DOI] [PubMed] [Google Scholar]
- Schweitzer P. The electrocardiographic diagnosis of acute myocardial infarction in the thrombolytic era. Am Heart J. 1990 Mar;119(3 Pt 1):642–654. doi: 10.1016/s0002-8703(05)80288-1. [DOI] [PubMed] [Google Scholar]
- Selwyn A. P., Fox K., Welman E., Shillingford J. P. Natural history and evaluation of Q waves during acute myocardial infarction. Br Heart J. 1978 Apr;40(4):383–387. doi: 10.1136/hrt.40.4.383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Short D. The earliest electrocardiographic evidence of myocardial infarction. Br Heart J. 1970 Jan;32(1):6–15. doi: 10.1136/hrt.32.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Timmis A. D. Early diagnosis of acute myocardial infarction. BMJ. 1990 Oct 27;301(6758):941–942. doi: 10.1136/bmj.301.6758.941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yusuf S., Pearson M., Sterry H., Parish S., Ramsdale D., Rossi P., Sleight P. The entry ECG in the early diagnosis and prognostic stratification of patients with suspected acute myocardial infarction. Eur Heart J. 1984 Sep;5(9):690–696. doi: 10.1093/oxfordjournals.eurheartj.a061728. [DOI] [PubMed] [Google Scholar]
- Zmyslinski R. W., Akiyama T., Biddle T. L., Shah P. M. Natural course of the S-T segment and QRS complex in patients with acute anterior myocardial infarction. Am J Cardiol. 1979 Jan;43(1):29–34. doi: 10.1016/0002-9149(79)90040-7. [DOI] [PubMed] [Google Scholar]