

Abstract
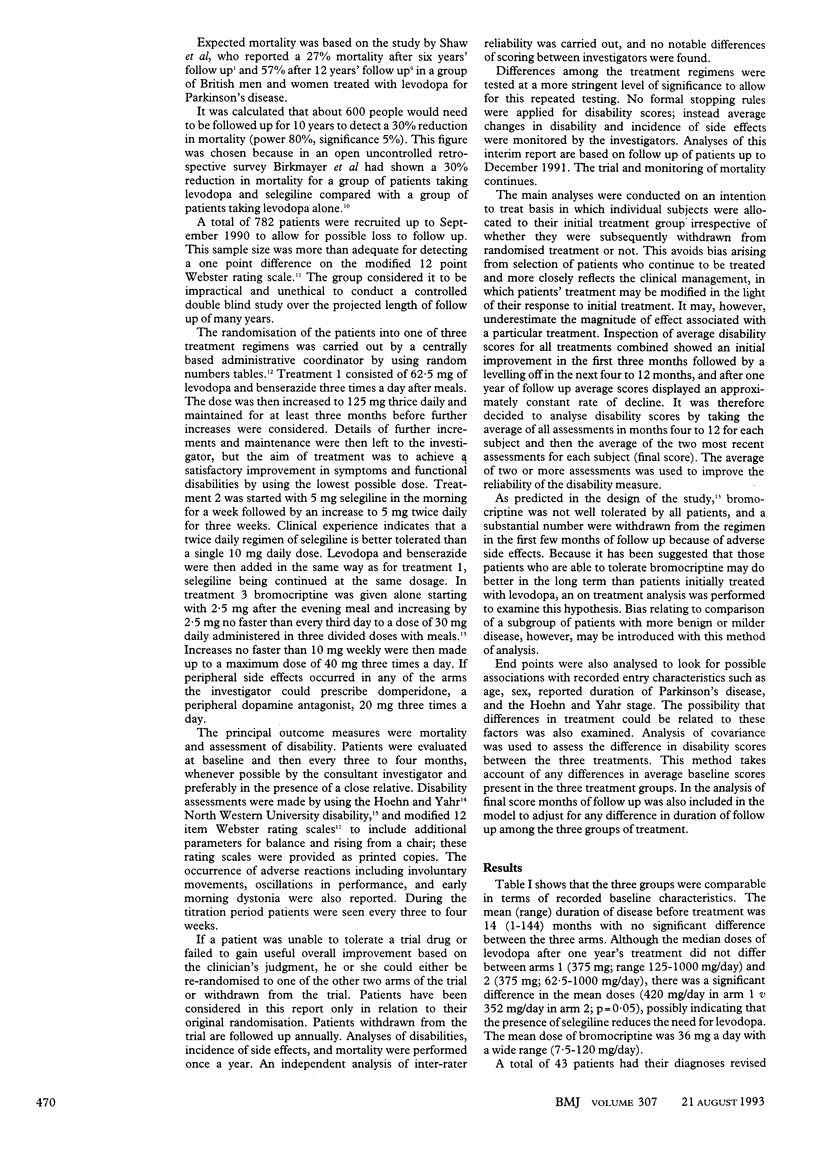
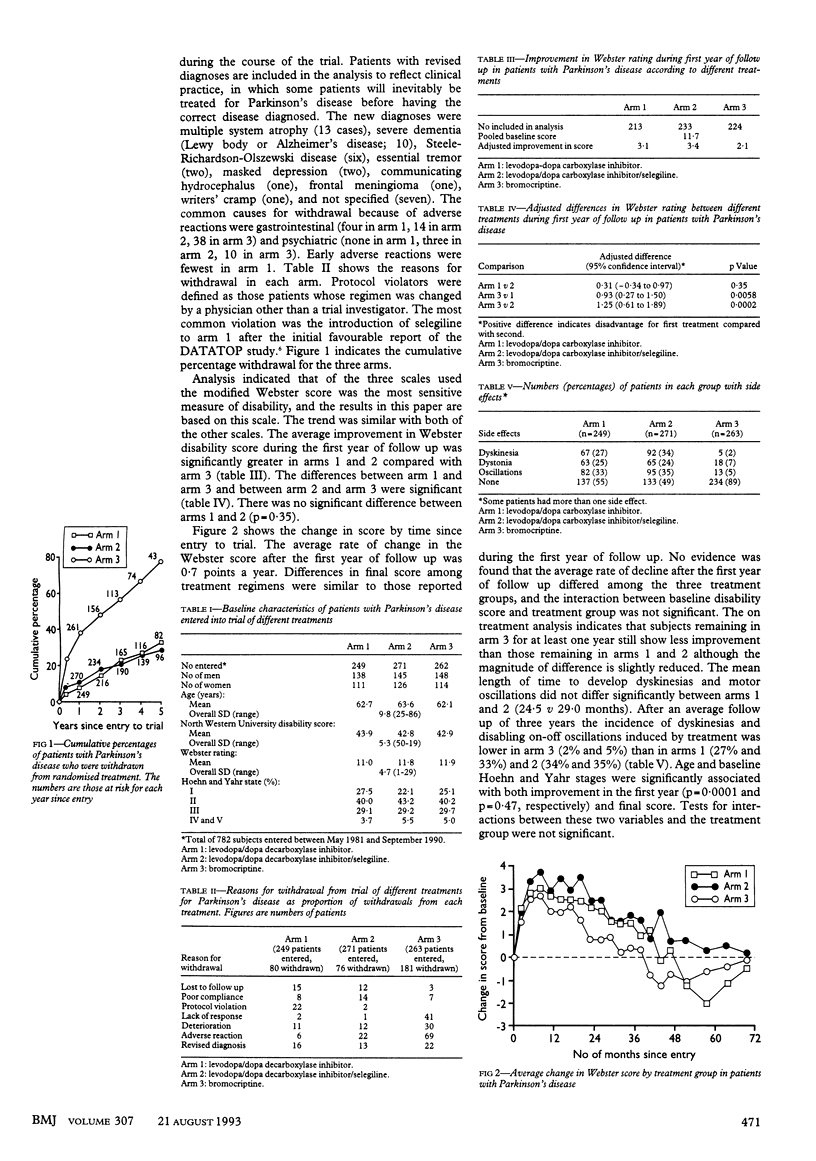
OBJECTIVE--To determine the optimum treatment for early Parkinson's disease. DESIGN--An open, long term, prospective randomised trial conducted by the Parkinson's Disease Research Group of the United Kingdom. SETTING--93 hospitals throughout the United Kingdom. SUBJECTS--782 patients with early Parkinson's disease who were not receiving dopaminergic treatment. INTERVENTIONS--Patients allocated to treatment with levodopa/dopa decarboxylase inhibitor alone (arm 1), levodopa/decarboxylase inhibitor/selegiline in combination (arm 2), or bromocriptine (arm 3). MAIN OUTCOME MEASURES--Disability assessment as judged by improvement on Hoehn and Yahr, modified Webster, and North Western University disability scales. Adverse event profile and mortality ratios. RESULTS--Interim results indicate that all three treatment regimens led to improvement in baseline disabilities after 12 months' treatment and that deterioration in control was apparent by three years. No significant differences were found between the results of treatment in arm 1 and arm 2, but both were significantly more effective than bromocriptine (arm 3) and had fewer early adverse reactions. The adjusted difference (95% confidence interval) in Webster rating for arm 3 v 1 was 0.93 points (0.27 to 1.50; p = 0.0058) and for arm 3 v 2 was 1.25 points (0.61 to 1.89; p = 0.0002). The incidence of dyskinesias and motor oscillations, however, was significantly lower in arm 3 (2% and 5%, respectively) than in arm 1 (27% and 33%, respectively) and arm 2 (34% and 35%, respectively). CONCLUSIONS--As there were no marked differences in functional improvement between the three groups the choice of treatment in the early stages of Parkinson's disease may not be critical.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Birkmayer W., Knoll J., Riederer P., Youdim M. B., Hars V., Marton J. Increased life expectancy resulting from addition of L-deprenyl to Madopar treatment in Parkinson's disease: a longterm study. J Neural Transm. 1985;64(2):113–127. doi: 10.1007/BF01245973. [DOI] [PubMed] [Google Scholar]
- CANTER G. J., DE LA TORRE R., MIER M. A method for evaluating disability in patients with Parkinson's disease. J Nerv Ment Dis. 1961 Aug;133:143–147. doi: 10.1097/00005053-196108000-00010. [DOI] [PubMed] [Google Scholar]
- Cohen G. The pathobiology of Parkinson's disease: biochemical aspects of dopamine neuron senescence. J Neural Transm Suppl. 1983;19:89–103. [PubMed] [Google Scholar]
- Curtis L., Lees A. J., Stern G. M., Marmot M. G. Effect of L-dopa on course of Parkinson's disease. Lancet. 1984 Jul 28;2(8396):211–212. doi: 10.1016/s0140-6736(84)90493-8. [DOI] [PubMed] [Google Scholar]
- Fahn S., Calne D. B. Considerations in the management of parkinsonism. Neurology. 1978 Jan;28(1):5–7. doi: 10.1212/wnl.28.1.5. [DOI] [PubMed] [Google Scholar]
- Gibb W. R., Lees A. J. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease. J Neurol Neurosurg Psychiatry. 1988 Jun;51(6):745–752. doi: 10.1136/jnnp.51.6.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoehn M. M., Yahr M. D. Parkinsonism: onset, progression and mortality. Neurology. 1967 May;17(5):427–442. doi: 10.1212/wnl.17.5.427. [DOI] [PubMed] [Google Scholar]
- Lees A. J., Stern G. M. Sustained bromocriptine therapy in previously untreated patients with Parkinson's disease. J Neurol Neurosurg Psychiatry. 1981 Nov;44(11):1020–1023. doi: 10.1136/jnnp.44.11.1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markham C. H., Diamond S. G. Long-term follow-up of early dopa treatment in Parkinson's disease. Ann Neurol. 1986 Apr;19(4):365–372. doi: 10.1002/ana.410190410. [DOI] [PubMed] [Google Scholar]
- Shaw K. M., Lees A. J., Stern G. M. The impact of treatment with levodopa on Parkinson's disease. Q J Med. 1980;49(195):283–293. [PubMed] [Google Scholar]
- Webster D. D. Critical analysis of the disability in Parkinson's disease. Mod Treat. 1968 Mar;5(2):257–282. [PubMed] [Google Scholar]