

Abstract
Heterogeneity in the longitudinal course of depressive symptoms was studied using general growth mixture modeling for young men in the Oregon Youth Study (N = 206), from ages 15 to 24 years. Four trajectory classes were identified: the very low, the moderate-decreasing, the high-decreasing, and the high-persistent classes. The 3 lowest classes differed primarily quantitatively with the initial level or mean level across time being the major determinant of class differences, whereas the high-persistent class appeared qualitatively different in terms of long-term developmental trends and variation. Findings from univariate and multivariate analyses revealed specific effects of childhood parental, contextual, and individual risk factors on the class membership as well as on the growth within each trajectory class.
The Course of Depressive Symptoms in Men from Early Adolescence to Young Adulthood: Identifying Latent Trajectories and Early Predictors
The history of the study of psychopathology consists of efforts to identify distinct types of abnormal behavior (e.g., the DSM diagnostic system). In particular, it has long been believed that there are distinctive subtypes of depression that show differing developmental course characteristics (e.g., age of onset, number of episodes in lifetime) and etiological risk factors (e.g., Chen, Eaton, Gallo, & Nestadt, 2000; Kendler et al., 1996; Sullivan, Kessler, & Kendler, 1998). Studies have identified several subtypes of symptoms, such as anhedonic, suicidal, psychomotor, and severe depressive, that differ in terms of etiology and prognosis (e.g., comorbidity with anxiety disorders, prodrome length, and number of lifetime episodes) (Chen et al.; Kendler et al.; Sullivan et al.). Typological approaches are of importance from a clinical perspective because increased understanding of the existence, characteristics, and predictors of subtypes and course is essential for the development of effective diagnostic systems and prevention and treatment programs.
Whereas these early studies certainly helped to characterize the heterogeneous nature of depressive disorders, little is known yet about subgroups of individuals who develop depressive symptoms over time. An inherent problem in the literature is that studies are typically based on a one-time diagnostic interview with adult samples. Subtypes of depression are viewed mainly as a state rather than a process that unfolded over the prior life course. Consequently, studies with such a static approach do not address possible developmental heterogeneity among individuals in the longitudinal patterns of symptoms. Critical questions for prevention concern how depressive symptoms unfold over time and who is likely to continue to have high levels of symptoms and eventually develop clinical levels of depression (e.g., major depression). These issues have important implications for refining diagnostic practices and developing effective treatment programs, because if differing longitudinal patterns of symptoms are determined by distinct underlying causes, then prevention and treatment programs should reflect the differences.
To identify valid subgroups of individuals who follow distinct longitudinal courses and to examine the etiologic mechanisms related to each group, it is necessary to approach the issue with a developmental perspective. The latent class approach within a developmental framework allows us to view depressive symptoms as evolving processes and to address intraindividual changes over time (Bushway, Thornberry, & Krohn, 2003). This provides us an informative avenue for examination of how depressive symptoms unfold over time for individuals and, consequently, to help identify possible multiple pathways to diverse subtypes of depressive disorders. In addition, two important components of prediction can be examined simultaneously in this latent class approach: First, whether distinct risk factors are predictive of class membership and, second, whether different risk factors are associated with changes of depressive symptoms over time for different classes of people. In other words, predictors of membership in latent classes can be examined in addition to predictors of growth within classes. Predictors may be associated with membership but not growth and vice versa, and predictors may have rather specific effects in distinguishing certain classes or in predicting to growth or change in perhaps only one class. Thus, this approach is crucial in identifying developmental factors associated with the course of depressive symptoms for high-risk groups. It is particularly important to investigate childhood and adolescent depressive trajectories that have strong continuities with adult depressive conditions and to examine determinants of the course of such classes.
In sum, from a developmental psychopathological perspective, it is critical to map out diverse patterns and courses of depressive symptoms over time to predict individuals who are most likely to continue to have the problems in adulthood and to identify factors that differentiate the subgroups of individuals, as well as factors that predict change within the subgroups. To our knowledge, no studies have addressed both issues with long-term prospective data. The present study identified distinct subgroups of young men who follow similar longitudinal trajectories of depressive symptoms across a 10-year period, from early adolescence (age 14–15 years) through young adulthood (ages 23–24 years), using the general growth mixture modeling approach (GGMM). This study also examined specific childhood risk factors, namely parental, contextual, and individual difficulties from childhood, as predictors of the subgroup membership and change within each subgroup.
Heterogeneity of Trajectories of Depressive Symptoms Across Adolescence and Young Adulthood
Although the patterns and mechanisms of continuity and discontinuity are not fully understood, due in part to the lack of research on depressive trajectories among men (Hammen & Rudolph, 1996), it is generally accepted that preadolescent boys are more likely to be depressed than are preadolescent girls (e.g., Anderson, Williams, McGee, & Silva, 1987). However, at adolescence, girls overall show an increase in depressive symptoms, whereas boys tend to experience fairly stable or slightly decreasing levels of symptoms (e.g., Garber, Keiley, & Martin, 2002; Garrison, Jackson, Marsteller, McKeown, & Addy, 1990; Ge, Lorenz, Conger, Elder, & Simons, 1994; Ge, Conger, & Elder, 2001; Kim, Capaldi, & Stoolmiller, 2003). For the current sample, using a latent growth curve approach, Kim et al. (2003) found that the mean level of depressive symptoms in young men slightly decreased from early adolescence (ages 14–15 years) through young adulthood (ages 23–24 years). Using multicohort longitudinal data, Ge and colleagues (Ge et al., 1994) also found that boys’ trajectories tended to be relatively flat over time, whereas girls’ trajectories showed a sharp increase between the ages of 12 and 15 years. Interestingly, these studies also suggested significant variations in the average levels of depressive symptoms across time in young men. Kim et al. (2003) found strong evidence of individual variability in initial status and growth rates among young men. Similarly, Ge et al. (2001) found significant variability in the growth factors (initial levels, linear and quadratic effects) among adolescent boys from Grades 7 through 12. Such variations indicate that there might be diverse depressive trajectories, depending on a variety of risk factors. Certain subgroups within the population may have a strong continuity to adult depressive symptoms, whereas other subgroups may show a trajectory of decreasing or increasing depressive symptoms to adulthood. There is also indirect evidence that is suggestive of diverse patterns of depressive trajectories. In studies of the young-adult outcomes of early adolescent depressive symptoms, outcomes differed depending on the presence of co-occurring conduct problems (e.g., Harrington, Fudge, Rutter, & Pickles, 1991). Capaldi and Stoolmiller (1999) found that the co-occurrence of depressive symptoms with conduct disorder in early adolescence predicted the poorest adjustment in multiple areas of young adult functioning.
Taken together, these findings strongly suggest that clusters of individuals follow similar patterns over the years and that related mechanisms and outcomes may differ depending on the patterns of each trajectory. Largely unknown from these studies are (a) how many subgroups of depressive trajectories there are in the population and (b) whether these diverse trajectory groups either qualitatively or quantitatively differ.
The first purpose of the present study was to identify distinct subgroups of young men who follow similar longitudinal trajectories of depressive symptoms from early adolescence through young adulthood and to examine the topography of each trajectory group. In this study, different depressive trajectories were identified based on the level of symptom severity assessed with a continuous measure rather than based on the presence of particular symptoms or the diagnosis of depression. Drawing upon previous studies, we proposed that there would be heterogeneity in the course of depressive symptoms over time associated with the nature of early experiences and subsequent circumstances. Because there are no studies on depressive trajectories, it is difficult to propose how many or what types of trajectories may exist. However, research on developmental taxonomic theories in problem behaviors (e.g., delinquency) suggest the possibility that adolescents are likely to differ in their growth and progress in psychopathology as they age (Chung, Hill, Hawkins, Gilchrist, & Nagin, 2002; Moffitt, Caspi, Harrington, & Milne, 2002; Nagin, 1999); for some, depressive symptoms may be limited to adolescence, whereas for others, the symptoms are predicted to be recurring or chronic and to extend into adulthood.
We expected that there would be at least four distinct trajectory groups, namely persistently high level, early onset-decreasing, late onset, and a low (or never) depressed group. There is some evidence that highly depressed children and adolescents are more likely to stay on a depressed trajectory because an early episode of depressive affect triggers a propensity toward chronically high levels of depressive symptoms (Nolen-Hoesksema, Girgus, & Seligman, 1992). Accordingly, we hypothesized that a persistently high group of individuals would be characterized by frequently recurring depressive symptoms over time and would have the highest prevalence rates of depressive disorders (e.g., major depression). In addition, following the findings that the majority of adolescent boys tend to have slightly decreased levels of depressive symptoms over time, we expected that another group of individuals would experience moderate levels of depressive symptoms in early adolescence, but then show decreasing levels of depressive symptoms through late adolescence and young adulthood. Studies have also indicated that some adolescents experience many stressful events as they go through multiple developmental changes (e.g., psychosocial, physical, and biological changes) and that stress is significantly associated with elevated levels of depressive symptoms (Ge et al., 2001; Ge et al., 1994). Consequently, we predicted that an adolescent onset group of individuals would experience an increase in depressive symptoms during adolescence and remained elevated through young adulthood. Lastly, several population-based studies identified a group of individuals with either no or a very few number of depressive symptoms (e.g., Chen et al., 2000; Kendler et al., 1996); therefore, we expected that there would be one group with consistently very low levels of depressive symptoms over time.
Early Risk Factors for Trajectories of Depressive Symptoms
The possibility of distinct trajectory subgroups raises the issue of diverse associated mechanisms. It is reasonable to assume that some factors are more closely related to a specific subgroup, but may have limited associations with some other groups. Although previous studies on the heterogeneity of depression did not examine developmental predictors of different trajectories, findings do suggest that distinct depressive trajectories may be associated with different factors (i.e., trajectory specific) rather than being influenced by a single common factor. Risk factors associated with juvenile-onset major depression have been found to differ from those for adult-onset major depression. Kessler and Magee (1993) found that family violence, parental psychopathology, and the early death of a parent were associated with increased risk for juvenile-onset of depression but not adult-onset depression. In addition, within the juvenile-onset group, children with prepubertal onset tended to have higher rates of criminality and family discord and lower rates of depressive disorder among relatives, compared to the postpubertal onset group. Jaffee et al. (2002) also found that the juvenile-onset group was associated with the highest levels of childhood risk factors (e.g., prenatal difficulties, motor skill deficits, and parental psychopathology) compared with the adult onset or never depressed groups. However, as these studies were all based on the static approach (data collected at one point in time), the factors that would distinguish developmental trajectory memberships remain unknown, as do predictors of changes (i.e., initial status and growth) within each trajectory group.
The second purpose of the present study was to examine the effects of parental, contextual, and individual risk factors from childhood on trajectory memberships and on the longitudinal course within each trajectory. The development of depressive symptoms was viewed as a response to the experience of stressors due to environmental and individual difficulties (Hammen & Rudolph, 1996). Individual difficulties due to the child’s own problem behaviors (e.g., antisocial behavior and academic achievement) and environmental stressors (e.g., multiple parental transitions and low family income) are known as significant risk factors for the development of depressive symptoms among children (e.g., Downey & Coyne, 1990). In the present study, parental depressive symptoms, antisocial behavior, family income, and parental transitions were examined as parental and contextual risk factors, and individual difficulties such as childhood academic achievement, antisocial behavior, and negative life events were examined as individual risk factors. Parental depressive symptoms and parental antisocial behavior may affect an adolescent’s depressive symptoms either directly through genetic transmission, or indirectly through poor parenting, increased vulnerability to stress, or through learning (e.g., Cicchetti & Toth, 1998). The youth’s academic problems and antisocial behavior indicate developmental failures and problems that generate stress, which are significantly related to the development of depressive symptoms (Capaldi, 1991, 1992). In addition, repeated experiences of negative life events in childhood may attenuate resilience and consequently relate to increased risk of depressive symptoms later in life (Brown, 1993). Finally, the young men’s childhood depressive symptoms were included to examine the possible influence of early depressive symptoms on the later development of depressive symptoms.
It was hypothesized that parental and contextual risk factors in childhood would be likely to contribute to distinguishing the trajectory memberships, due to an association with the initial levels, as the early individual risk factors are known to be influenced by the parental and contextual factors (although the causality was not tested in this study). Therefore, it was expected that membership in the high-persistent group, which would have higher prevalence rates of clinical depressive disorders (e.g., major depression, bipolar affective disorder), would be associated with higher levels of parental antisocial behavior and depressive symptoms, greater numbers of parental transitions, and lower levels of family income. It was also expected that the young men’s early individual risk factors would exert a stronger influence on within group changes over time. Thus, men’s childhood antisocial behavior, depressive symptoms, academic achievement, and the negative life events would be more strongly associated with changes within each trajectory subgroup. This conceptualization is based on the failure model that assumes poor psychosocial skills (e.g., poor academic skills and aggressive behaviors) lead to repeated failure and rejection in social relations, which generates stress and subsequently places the children at higher risk for depressive symptoms (Capaldi, 1991, 1992).
Analysis Plan
The present study used a GGMM (Muthén & Shedden, 1999) approach to (a) identify distinct subgroups of longitudinal trajectories of depressive symptoms; (b) examine how the probability of membership in each trajectory subgroup was distinguished by parental, contextual, and young men’s individual characteristics in late childhood; and (c) examine how the same set of risk factors affected within-subgroup change in depressive symptoms. The statistical framework for hypothesis testing in GGMM is relatively new, although the basic idea of identifying distinctive subgroups has a long tradition in psychopathology. Unlike conventional growth curve modeling, which assumes that individual differences in trajectories are well described by continuous variability of trajectory properties (i.e., intercepts and slopes for linear growth models) in the population, GGMM assumes that individuals tend to cluster into distinct subgroups, each with a different mean trajectory (see Nagin, 1999 and Muthén & Muthén, 2000 for further description) and perhaps with differences in dispersion about the mean. All models in this study were estimated using Mplus (2.13 and 3.0) (Muthén & Muthén, 1998–2004).
Analyses were threefold. First, latent trajectories of depressive symptoms from early adolescence (ages 14–15 years) through young adulthood (ages 23–24 years) were identified using GGMM. The validity of the trajectory classes was tested by examining the prevalence rates of clinical levels of depressive disorders across the classes using the data from a diagnostic interview assessed at ages 25–26 years. Second, univariate analyses were conducted predicting class membership, initial status or change within a class, or both. Tests of predictors of class membership required estimating multinomial logistic regressions, which in turn required designating one of the latent groups as a reference group and predicting the probability of membership in a given group versus the reference group. To predict the most substantive problems with depressive symptoms, the class that showed the highest level of depressive symptoms was used as the reference group. Latent class by risk factor interactions on initial status and growth within a class were also tested. Third, the univariate results were used to guide the multivariate modeling to determine the most compact set of risk factors.
Methods
Sample and Procedure
This study utilized data from the Oregon Youth Study (OYS), an intensive multimethod and multiagent longitudinal study of 206 boys and their parents. Participants were recruited in 2 consecutive school years (Cohorts I and II in 1983–84 and 1984–85, respectively) through fourth-grade classes (ages 9–10 years) in higher crime areas of a medium-sized metropolitan region in the Pacific Northwest. Schools in areas with the highest rates of police-reported delinquent episodes by juveniles were randomly selected for recruitment into the study, and all of the boys in all of the fourth-grade classrooms in the selected schools were eligible for participation in the study, as long as the family spoke English (only one or two families were ineligible on this criteria). Of the 277 eligible families, 206 agreed to participate in the initial wave of data collection, and 196 youths (95.1%) still remained as part of the panel 17 years later (3 of the young men died). The sample was predominantly White (90%) and lower and working class (75%). At Wave 1 (W1), the average age of the youth was 10.1 years and the average ages of mothers and fathers were 33.7 and 36.2 years, respectively. A more detailed description of the sample and recruitment procedures is described in Capaldi and Patterson (1987).
The young men and their parents participated in assessments every year. Assessments included structured interviews, questionnaires, phone interviews (W1 and W3 only), home observations (W1 and W3 only), and videotaped problem-solving interaction tasks (W1, W3, W5, W7, and W9 only). In addition, school data (e.g., teacher-report questionnaires and school achievement test records data), court, and Department of Motor Vehicle records were collected annually. For the present study, predictors were taken from W1, W3, and W5, when full-scale assessments were conducted. Three exceptions were parents’ antisocial behavior, young men’s childhood depressive symptoms, and negative life events. Parent’s antisocial behavior was assessed only at W1 and W2, and the childhood depressive symptoms were assessed in Waves 2 (ages 10–11 years) through 5 (ages 13–14 years). Negative life events were assessed only in W4 and W5. In order to increase the reliability of the measures, each predictor was developed by taking a mean of multiple waves’ scores. Young men’s reports of depressive symptoms were taken from W6 (Grade 9, ages 14–15 years) through W15 (ages 23–24 years).
Measures
To take full advantage of the multimethod and multiagent approach, we developed a construct to represent each predictor. The development of constructs was guided by the general construct building strategy that has been used in the OYS (Patterson & Bank, 1986). First, indicators had to have an acceptable level of internal consistency (i.e., an alpha of at least .60), and items included in each indicator had to have an item to total correlation greater than .20; secondly, an indicator had to converge with other indicators designed to assess the same construct (i.e., the factor loading for a one-factor solution had to be .30 or higher). Sample items and internal consistency values for each indicator are described in Table 1.
Table 1.
Psychometric Properties of Measures
| Construct and measures | Respondent | Number of items | Sample Item | Internal consistency |
|---|---|---|---|---|
| Young men’s depressive symptoms CES-D (W6 ~ W 15) (Radloff, 1977) | Youth | 20 | I did not feel like eating
I was bothered by things that usually don’t bother me |
.85 – .91 |
| Young men’s depressive symptoms in late childhood, CDRS (W2 ~ W5) (Birleson, 1981) | Youth | 18 | I feel like crying
I feel like running away |
.71 – .79 |
| Young men’s antisocial behaviors in late childhood | Teacher | 18 | Defiant, talks back to staff/Lying or cheating | .85 |
| W1 (Grade 4) | Peer | 9 | Kids who fight a lot with other kids | .92 |
| Youth | 13 | In the last 24 hours, did you argue with an adult? | .62 | |
| W3 (Grade 6) | Teacher | 19 | Argues a lot/Steals | .88 |
| Youth | 42 | How often do you cheat on school tests? | .81 | |
| Observer | 20 | Hostile, arrogant, noncompliant attitude toward mother | .82 | |
| W5 (Grade 8) | Teacher | 20 | Threaten people/Doesn’t feel guilt | .94 |
| Youth | 12 | In the last 3 days, did you tell a lie? | .71 | |
| Young men’s academic achievement in late childhood | Parents | 6 | Is your child in a special class? | .73 (M), .78 (F) |
| W1 (Grade 4) | Teacher | 8 | Has he ever repeated a grade? | .91 |
| Record | WRAT
Scholastic Test Scores |
|||
| W3 (Grade 6) | Parents | 4 | Reading performance | .89 (M), .91 (F) |
| Teachers | 4 | Spelling performance | .96 | |
| Record | WRAT | |||
| Record | Scholastic Test Scores | |||
| W5 (Grade 8) | Parents | 4 | Same as W3 | .86(M), .85 (F) |
| Teachers | 4 | Same as W3 | .94 | |
| Record | Scholastic Test Scores | |||
| Young men’s negative life events in late childhood | ||||
| W4 (Grade 7) & W5 (Grade 8) | Youth | 37 | I was suspended from school
A close friend of mine died |
.54 – .71 |
| Father’s depressive symptoms CES-D (W1, 3, & 5) (Radloff, 1977) | Father | 20 | I felt that everything I did was an effort
I thought my life had been a failure |
.76 – .88 |
| Mother’s depressive symptoms CES-D (W1, 3, & 5) (Radloff, 1977) | Mother | 20 | I had trouble keeping my mind on what I was doing
I had crying spells |
.87 – .92 |
| Father’s antisocial behavior | Record | Number of arrests/Number of license suspension | .52 | |
| Father | MMPI (hypomania/psychopathic deviate) | |||
| Mother’s antisocial behavior | Record | Number of arrests/Number of license suspension | ||
| Mother | MMPI (hypomania/psychopathic deviate) | .47 |
Depressive symptoms in adolescence and young adulthood
The Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977) was used to assess depressive symptoms every year from W6 to W15. The CES-D is a 20-item self-report scale that was designed to measure depressive symptomatology among adults in the general population and has been validated in many previous studies with adolescent samples (e.g., Garrison et al., 1990). Respondents were asked to report how they felt during the past week on a 4-point scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). The means for the youths’ depressive symptoms ranged from 7.14 (SD = 6.16) to 11.33 (SD = 8.09) over the 10 years. Correlations of depressive symptoms across years ranged from .23 to .60 and tended to be largest for adjacent years and to attenuate across longer time periods – a typical pattern for associations of psychopathology over time. Using a cutoff point of 16,1 60.5% (n = 125) out of 206 men experienced significantly high levels of depressive symptoms at least once during the 10-year period. Among the men above the cut off, at least once, 60.8% (n = 76) experienced one or more occasions of recurrence of high symptom levels over the period, suggesting one third of the OYS men experienced two or more episodes of high levels of depressive symptoms from adolescence through young adulthood.
Depressive symptoms in late childhood
The young men’s depressive symptoms in late childhood were assessed yearly from Waves 2 through 5 using the Child Depression Rating Scale (CDRS, Birleson, 1981). The CDRS is an 18-item scale that was designed to assess the symptomatology of depressive disorders in childhood. Respondents were asked to indicate whether each statement applied to them during the past week on a three-point scale ranging from 1 (most of the time) to 3 (hardly ever). Some of the items were reverse coded so that higher scores of the combined items indicated higher levels of depressive symptoms. The mean for the young men’s depressive symptoms in childhood ranged from 25.85 (SD = 4.76) to 26.30 (SD = 4.68). A mean of childhood depressive symptom scores over the four waves was computed.
Antisocial behavior in late childhood
The young men’s antisocial behavior in late childhood was taken from assessments at W1, W3, and W5 (ages 9–10 through 13–14 years). The antisocial construct was developed with items from the Teacher Report From of the Child Behavior Checklist Teacher (CBC-TRF; Achenbach & Edelbrock, 1983), telephone interviews with the youth, youth self-report interview, peer nomination questionnaires, home observational data, and interviewer impression. Each measure was standardized and then a mean score of combined indicators of antisocial behavior was computed. Parent reports of young men’s childhood antisocial behavior were not included to avoid possible confounded effects with parental reports of their own psychopathology (i.e., depressive symptoms and antisocial behavior).
Academic achievement in late childhood
The construct of young men’s academic achievement was developed with items from the parent report on the CBC, the CBC-TRF; Achenbach & Edelbrock, 1983), and data from school records including performance on national achievement tests and grade point average for the year.
Negative life events in late childhood
The perceived negative impact of stressful life events were assessed with the Junior High Life Experiences Survey (JHLES; Swearingen & Cohen, 1985) at W4 and W5. Respondents were asked to rate how good or bad each event was for them on a 7-point scale ranging from a very bad change to a very good change. Items were reverse coded so that higher scores indicate greater perceived negative impact from the stressful events. Scores across the two waves were combined and averaged.
Parental antisocial behavior
The construct of parents’ antisocial behavior included three indicators: number of arrests; number of driver’s license suspensions; and a summary score of two subscales from the MMPI, namely the Hypomania and Psychopathic Deviate scales. Parents who scored above a t-score of 70 on either MMPI scale were given a score of 1; if they scored above 70 on both scales, a score of 2 was assigned; otherwise the score was 0. The arrest and Department of Motor Vehicles records were collected only at W1, and the MMPI was assessed at W2.
Parental depressive symptoms
The CES-D was also used to assess parents’ depressive symptoms at W1, W3, and W5. Parents independently reported their levels of depressive symptoms. The average score over the three waves was 11.27 (SD = 7.18) for mothers and 9.10 (SD = 5.69) for fathers.
Parental transitions
The number of changes in parental figures from the young men’s conception prior to W5 (age 13–14 years) was coded as 0, 1, 2, and 3 or more. No parental transition was coded as 0; a first-time separation (e.g., either single mother or father families) was coded as 1; a first time repartnering was coded as 2; and further separations and repartnerings were coded as 3. Seventy three (35.4%) young men were from two biological parents families, 31 (15%) were from first-time, single-parent families, 61 (29.6%) from first-time stepparent families, and 39 (18.9%) from families with multiple parental transitions.
Family income
Both parents’ reports on income were averaged at each wave and then averaged across time. Parents provided an estimate of annual household income, including child support and any other financial aid. The response categories ranged from 1 (less than $4,999) to 8 (higher than $40,000) and were converted into a set of dollar categories by assigning the midpoint of the interval (see Duncan, Brooks-Gunn, & Klebanov, 1994). The first and the last categories were assigned to $3,500 and $52,000, respectively. Mean family annual income level over the study period was $19,232 (SD = $11,605.21).
Lifetime diagnosis of depression
Diagnoses of major depression, dysthymia, and manic and bipolar disorders were determined by using the Composite International Diagnostic Interview Version 2.1 (CIDI; World Health Organization, 1997), which was administered at W17 (ages 25–26 years). The CIDI is a fully standardized interview based on the definitions and criteria of the tenth revision of the International Classification of Diseases (ICD-10; World Health Organization, 1992, 1993) and the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994). Participants answered the structured questions using a reporting period of lifetime. Twenty eight young men (14.1%) were diagnosed with either major depression (n = 27) or dysthymia (n = 1) and four (2%) men were diagnosed with bipolar I manic disorder.
The CIDI has been proved to be valid and reliable in a variety of cultures and setting, with high interrater reliabilities. Wittchen and colleagues reported that the percentage agreements for all diagnoses were over 90%, and overall kappa values were also above .90. For out study, interviewers were trained in a 2-week intensive session, and each interviewer completed at least two practice sessions under close supervision before working with the OYS men.
Missing data in the young men’s depressive symptoms from Waves 6 to 15 were minimal (i.e., the number of participants ranged from 200 to 203 during the study period), only 41 (about 2%) of the 2060 data points were missing, with 184 young men having complete data (10 repeated assessments). Of the 22 young men with partial data, 2 were missing the first 7 assessments, but the other 20 had 7 or more of the 10 assessments. Missing data in the predictors (assessed at Waves 1, 3, and 5) were also minimal for the OYS men; for parental and contextual predictors, only 9 of 1442 (0.6%) and only 4 of 618 (0.6%), respectively, of the data points were missing. Missing data were more prevalent in the parent variables, largely due to the lack of a parent figure in the home. Models were estimated using the full information maximum likelihood (FIML) estimator in Mplus, which allows the inclusion of participants with partial data on the trajectory variable (CES-D), but not subjects with missing predictor data. Thus, the sample size given in the tables varies somewhat across models depending on which background covariates are included.
Results
Distributions of Depressive Symptoms over Time
As a first step, the distributions of the young men’s depressive symptoms were examined for evidence consistent with a mixture of distributions. As found in Kim et al. (2003), at each wave (a) there was a mild floor effect such that 8–11% of the sample was at the minimum score of zero, (b) the distributions exhibited mild positive skewness, and (c) there were a small number of outliers. Such skewness, outliers, and a floor effect are consistent with a mixture of normal distributions (latent classes) that differ at least in mean level and possibly also dispersion and prevalence in the population.
Examination of individual growth curves over the 10 years indicated systematic heteroscedasticity, or a marked tendency for the year-to-year variability to be higher for those with overall higher mean levels of depressive symptoms across the 10-year period. A set of plots demonstrating all the above and other analyses for this study are available from the first author upon request. In summary, basic univariate and bivariate statistics and growth curve plots all strongly indicated conditions that depart from the standard linear growth curve structure and are consistent with population heterogeneity due to latent classes that differ at least in mean level and possibly covariance structure.
Estimation of the Growth Mixture Model: The Four Identified Trajectory Groups
The first step in analysis involved a basic linear growth model in which, for each individual, the 10 repeated assessments of depressive symptoms over time were assumed to be adequately described by a straight line characterized by an intercept (initial status at age 14–15 years) and slope (change in depressive symptoms per year). Deviations from the straight line are assumed to be due to time-specific influences, which include the usual sources of measurement error but also may reflect episodic depressive symptoms. An episode of depression could influence the severity of the next episode, or episodes of depression could possibly last across two measurement periods and not be adequately captured by the slope parameter. Thus, the specific effect of depressive symptoms in one time period on the next time period was tested by including regression paths from the time-specific influence at time t to the observed depressive symptoms measure at time t + 1 (i.e., autoregressive effects) (for more details, see Kim et al., 2003). In addition to parameters for the mean levels of the intercept and slope and the autoregressive effects, the model had the following free parameters: three for the intercept and slope standard deviations and their correlation and one for the time-specific standard deviation. Each latent class in the growth mixture model required these seven growth parameters to describe growth, plus one population prevalence parameter. Thus, each additional class added eight parameters to the overall model.
To identify the optimal number of latent classes, the Bayesian Information Criteria (BIC), which balances goodness of fit with parsimony, was used (Nagin, 1999).2 Initially as classes are added that improve the model fit, the BIC decreases. As recommended, classes were added until the BIC started increasing, and then the model that minimized the BIC was chosen. The BIC decreased steadily for one through four-class solutions (13387.14, 12943.66, 12916.25, and 12913.16, respectively) but increased for the five-class model (12938.63), indicating that the four-class model is optimal.3, 4
In a latent growth mixture model, each individual receives an estimated probability for belonging in each of the classes (posterior probabilities). Bandeen-Roche and colleagues (Bandeen-Roche, Miglioretti, Zeger, & Rathouz, 1997) advocated checking model adequacy by assigning individuals to pseudoclasses, a best estimate of an individual’s true latent class membership, using the posterior probabilities and a simple randomization scheme (Bandeen-Roche et at.). The average class probabilities by pseudoclass for the final four-class model ranged from .85 to .96, whereas the probability of incorrect class assignment was very low, ranging from 0 to .11, indicating that class discrimination is very good.
Mean trajectories (solid lines) and fitted trajectories (dashed lines) are shown in Figure 1, and parameter estimates for the model are shown in Table 2. The fitted mean linear trajectories matched the overall linear trends of the mean class trajectories reasonably well. The departures, although fairly substantial for Classes 3 and 4, did not suggest any systematic lack of fit from a linear pattern. Classes 2 and 3 have modest downward trends, but Classes 1 and 4 have flat trends. The very low group (Class 1, n = 12) consisted of young men who had only a few depressive symptoms from early adolescence through young adulthood. Individuals in the moderate-decreasing group (Class 2, n = 70) showed moderate levels of symptoms during early adolescence, but significantly decreasing levels over time. The high-decreasing group (Class 3, n = 74) showed fairly high levels of symptoms during adolescence, but significantly decreasing levels across time. Finally, the high-persistent group (Class 4, n = 50) consisted of young men who experienced high levels of recurrent depressive symptoms, and the average level of symptoms remained high throughout the study years.
Figure 1.

Mean class trajectories (solid lines) and fitted mean trajectories (dashed lines) for depressive symptoms.
Table 2.
Estimates for the Trimmed Four-Class Model
| Very low (n = 12) | Moderate-decreasing (n = 70) | High-decreasing (n = 74) | High-persistent (n = 50) | |
|---|---|---|---|---|
| Intercept factor mean | 1.60 | 6.22 | 11.00 | 15.70 |
| Slope factor mean | .01 | −2.70 | −3.61 | −.37 |
| Intercept factor standard deviation | 0 | 2.37 | 3.86 | 3.07 |
| Slope factor standard deviation | 1.74 | 2.32 | 6.37 | 0 |
| Intercept-slope factor correlation | 0 | −.83 | −.89 | 0 |
| Time-specific standard deviation | 1.40 | 3.24 | 5.88 | 8.91 |
| Auto-regressive specific effect | 0 | 0 | 0 | 1.20 |
| Class proportion | .06 | .35 | .35 | .24 |
Note. All parameters were significant at p < .05 except slope factor means for the ‘very low’ and ‘high-persistent’ group. Trimmed parameters fixed at zero are indicated by zero with no decimal point.
None of the men in the very low group experienced clinically high levels of depressive symptoms (cut off of 16 or above), and seven men in the moderate-decreasing group experienced the high symptom levels only once during the 10-year period. On the other hand, 91.9% (n = 68) out of 74 men in the high-decreasing group experienced the high symptom levels at least once from adolescence through young adulthood, and more than one half of those men (n = 36) experienced two or more episodes of such high levels of symptoms during the period. All of the 50 men in the high-persistent group experienced the high symptom levels at least once, and 80% of them (n = 40) had recurrent high symptoms during the study years.
Boxplots of the depressive symptoms distributions by class revealed striking latent class differences not evident in the mean trajectories (Figure 2). The variability within each class appeared fairly constant across time points, but was associated with class membership, such that the very low group had the least variability, followed in order by the moderate-decreasing group, the high-decreasing group, and the high-persistent group. Thus, by allowing for different levels of variation in growth curve factors and time-specific variation across classes, the growth mixture approach was successful in modeling the systematic positive relation between the mean level and variability of depressive symptoms (heterscedasticity) noted above.
Figure 2.
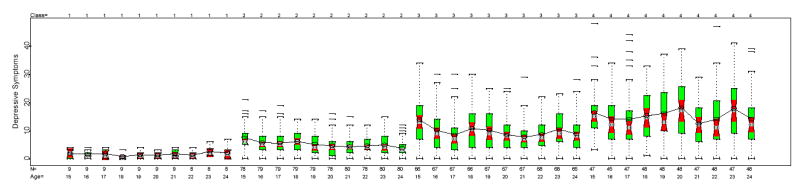
Boxplots of depressive symptoms distributions by latent class.
Means are indicated by an open circle and are connected by a solid line within each class. The median is indicated by the white band in the middle of the boxplot. The notched region around the median is an approximate 95% confidence interval.
Table 2 shows estimated parameter values for all four classes. The three lowest classes differed primarily quantitatively with initial level or mean level across time being the major determinant of class differences. The higher the class initial starting point or mean level, the greater the downward trend over time and the greater the magnitude of long-term variation (intercept and slope) and time-specific variation. The highest class, however, appeared qualitatively different from the other three classes in that it started highest, but did not decline over time, and showed no variation in long-term linear trends. In addition, it had the highest level of time-specific variation. The high-persistent group also had a small, positive autoregressive effect that was absent from the other three classes. The effect only accounted for 2% of the total variance in depressive symptoms across time, however, with the intercept or average level accounting for 10% and the current specific effect for 88%. Thus, the majority of variation in the high-persistent group was accounted for by episodic effects.
Prevalence of Depression Diagnoses by Trajectory Groups
As a way to validate the trajectory classification, life-time diagnoses of depression assessed at ages 25–26 years were examined for each latent class. No one in the very low group and only 5.7% of the individuals in the moderate-decreasing group were diagnosed with depressive disorders. On the other hand, 20% of the individuals in the high-decreasing group and 29.2% of the individuals in the high-persistent group were diagnosed with depressive disorders. These differences were highly significant, χ2 = 14.57, df = 3, p < .002. Thus, the probability of lifetime diagnosis of depressive disorder was highly related to the latent class membership.
Univariate Predictors of Latent Class Membership and Initial Status and Change Within Class
Next, the effects of parental, contextual, and individual risk factors from childhood on the trajectory memberships and on the longitudinal course within each trajectory were examined. An extensive set of plots aimed at checking the linearity of class and within class regressions is available from the first author upon request. Separate analyses on maternal (n = 197) and paternal (n = 147) depressive symptoms on all models tested indicated their main effects were similar. Therefore, for the sake of parsimony, a mean score of maternal and paternal depressive symptoms was computed and used for further analyses, with one exception. An interaction between maternal and paternal effects in predicting class membership was expected (see Kim et al., 2003), and these are presented later in separate analyses. In contrast, separate analyses on maternal (n = 189) and paternal (n = 130) antisocial behavior indicated that only paternal antisocial behavior was significant. Because there were no a priori hypotheses concerning the interaction of maternal and paternal scores (also no significant interaction effect was found in previous work; see Kim et al., 2003), only the paternal score was further considered. Table 3 presents latent class means and standard deviations of the childhood risk factors included in the further analyses, and the global three degree of freedom chi-square test statistic for the class regression model (explained below) for each risk factor.
Table 3.
Means and Standard Deviations for Childhood Risk Factors Across Four Trajectory Classes
| Very low group | Moderate-decreasing group | High-decreasing group | High-persistent group | X2(3) | |
|---|---|---|---|---|---|
| Contextual factors | |||||
| Parental transitions | .67 (.99) | 1.10 (1.17) | 1.42 (1.12) | 1.67 (1.10) | 11.72** |
| Family income | 28921 (15804) | 21316 (11829) | 17634 (10484) | 15679 (10114) | 10.94* |
| Paternal antisocial behavior | 7.27 (2.95) | 8.39 (5.42) | 9.62 (5.61) | 10.20 (6.43) | 2.73 |
| Parental depressive symptoms | 8.39 (2.95) | 10.08 (5.23) | 10.38 (6.02) | 12.96 (7.40) | 16.94*** |
| Young men’s individual factors from childhood | |||||
| Antisocial behavior | −.36 (.85) | −.07 (.85) | −.11 (.77) | .35 (.97) | 10.53* |
| Academic achievement | .44 (.94) | .10 (.79) | −.03 (.78) | −.22 (.78) | 8.79* |
| Depressive symptoms | 22.73 (1.26) | 25.13 (3.29) | 26.78 (3.66) | 27.10 (3.18) | 35.20*** |
| Negative life events | 1.75 (2.38) | 3.36 (3.56) | 4.16 (3.75) | 6.09 (3.69) | 27.33*** |
p < .001.
p < .01.
p < .05.
Next, a series of nested chi-square tests was run separately for each risk factor that would help determine whether the given risk factor predominantly predicted class membership, growth within classes, both, or neither. First, three models were tested for each predictor, namely a class regression model, a within class model, and a full model. The class regression model examined associations between each predictor and class membership in a three degree of freedom chi-square test without including effects of the predictor on within class growth. A significant chi-square indicates that the predictor significantly discriminates between at least two classes. The within class regression model examined the association between each predictor and intercept and slope within each latent class in an eight degree of freedom test without including effects of the predictor on class membership. A significant chi-square indicates that the predictor significantly predicts intercept or slope in at least one class. The full model with 11 degrees of freedom simultaneously tested both types of effects. The comparison between the full model and the class regression model provides an eight degree of freedom nested chi-square test of the within class regressions over and above the class regressions. Likewise, comparing the full model to the model with only within class regressions provides a three degree of freedom nested chi-square test of the class regressions over and above the within class regression. No results from the global chi-square tests are shown because of space limitations, but the complete table is available from the first author upon request.
First, findings indicated, taking into account effects on class membership, that all risk factors, except parental transitions and family income, were significantly associated with growth within class. Second, taking into account within class growth, parental transitions, family income, childhood academic achievement, childhood depressive symptoms, and negative life events were significantly associated with class membership. In addition, parental depressive symptoms were marginally associated with class membership. Paternal and young men’s antisocial behavior did not predict class membership when within class growth was accounted. These findings indicate that childhood academic achievement, depressive symptoms, negative life events, and parental depressive symptoms have genuine effects on class discrimination and within class growth.
Because our main interest was in qualitative differences among the groups, the ability of a given predictor to (a) uniquely discriminate the high-persistent class from the other three classes and (b) predict growth better in some classes than others was tested. If either of these conditions holds, analysis of predictor effects provides additional evidence for qualitative differences among the groups beyond that obtained from just analyzing the trajectories (see discussion above in reference to Table 2). Class 4 was the reference class for the multinomial logistic regressions, thus a given predictor uniquely discriminated Class 4 from the other three classes if the constrained model with the three class regression coefficients forced to be equal fitted as well as the more general model where the three class regressions were freely estimated. Predictor by latent class interactions are indicated when the more general model with all predictor to intercept and predictor to slope effects freely estimated fits better than the more constrained model that forces each effect to be equal across all the latent classes.
Findings from the global chi-square tests (not shown but available upon request) indicated that only childhood depressive symptoms and family income (albeit marginally significantly) discriminated among the three lowest trajectory classes, whereas parental transitions, parents’ depressive symptoms, childhood academic achievement, and negative life events significantly discriminated the high chronic class from the other three classes. Findings from the tests to examine differential within class effects on growth indicated that only the effects of childhood academic achievement were significantly different across classes. On the other hand, paternal antisocial behavior, parents’ depressive symptoms, childhood antisocial behavior, childhood depressive symptoms, and negative life events predicted within class growth similarly across all classes.
Based on these global chi-square tests, a final univariate model was estimated for each predictor. These results are Shown in Table 4 and include prediction to class membership, intercepts, and slopes. With few exceptions, the specification of each univariate model took into account the results of the global tests, so for example, if the class regressions were all equal for a given predictor, that specification was included in the final univariate model for that predictor. The only exceptions to this general approach were for the class regressions of family income and the within class regressions for paternal antisocial behavior and childhood depressive symptoms where a somewhat more liberal approach was taken. Even though the chi-squares for these three predictors were only marginally significant, fewer constraints were used in the final models because the p levels were less than .10 (p = .054, p = .087, and p = .059, respectively). Thus for these three predictors, the indicated results should be interpreted cautiously.
As described above, parental transitions uniquely discriminated the high-persistent group from the other three trajectory classes. The estimated class regression effect shown in Table 4 is negative, indicating that the more transitions, the higher the probability of membership in the high-persistent group and the lower the probability of membership in the other three groups. Family income discriminated only the very low group from the high-persistent group. The estimated effect was positive, indicating that the higher the income, the higher the probability of membership in the very low group and the lower the probability of membership in the high-persistent group.
Table 4.
Parameter Estimates for Final Univariate Models
| Class | Parental transitions | Family income | Paternal antisocial behavior | Parental depressive symptoms | Childhood antisocial behavior | Childhood academic achievement | Childhood depressive symptoms | Negative life events | |
|---|---|---|---|---|---|---|---|---|---|
| Prediction to class | 1 vs. 4 | −.47b | .09a | 0 | −.10b | 0 | .50a | −1.56c | −.20c |
| 2 vs. 4 | −.47b | .04 | 0 | −.10b | 0 | .50a | −.68 | −.20c | |
| 3 vs. 4 | −.47b | .02 | 0 | −.10b | 0 | .50a | −.06 | −.20c | |
| Prediction to initial status | 1 | 0 | 0 | .65 | .17c | .86b | −.21 | 1.81c | .27c |
| 2 | 0 | 0 | 1.96c | .17c | .86b | −2.14c | 1.81c | .27c | |
| 3 | 0 | 0 | 1.96c | .17c | .86b | −2.14c | 1.81c | .27c | |
| 4 | 0 | 0 | 1.96c | .17c | .86b | −.21 | 1.81c | .27c | |
| Prediction to slope | 1 | 0 | 0 | .11 | −.10 | −.66 | .29 | 3.21c | −.21a |
| 2 | 0 | 0 | −1.44a | −.10 | −.66 | 2.22c | −2.09c | −.21a | |
| 3 | 0 | 0 | −1.44a | −.10 | −.66 | 2.22c | −2.09c | −.21a | |
| 4 | 0 | 0 | −1.44a | −.10 | −.66 | .29 | −2.09c | −.21a | |
| Likelihood | −6326.54 | −6343.45 | −3936.08 | −6332.29 | −6370.89 | −6363.41 | −6339.92 | −6315.97 | |
| Free parameters | 25 | 27 | 26 | 27 | 26 | 29 | 30 | 27 | |
| BIC | 12786.02 | 12830.63 | 8008.45 | 12808.30 | 12880.31 | 12881.32 | 12839.67 | 12775.53 | |
| N = 204 | N = 205 | N = 130 | N = 205 | N = 206 | N = 206 | N = 206 | N = 204 |
Note. < .05.
< .01.
< .001.
Paternal antisocial behavior and young men’s childhood antisocial behavior predicted only within class growth. The effects of paternal antisocial behavior were somewhat different in the very low group versus the other three groups. For the moderate-decreasing, high-decreasing, and high-persistent groups, paternal antisocial behavior was significantly and positively related to intercept and significantly and negatively related to slope. Thus, it predicted a higher level of depressive symptoms at ages 14–15 years, but also recovery over time within the three elevated groups. Neither effect was significant for the very low symptoms group. Childhood antisocial behavior was significantly and positively related to initial status, but nonsignificantly related to slope for each group.
Four variables predicted class membership and within class growth, namely parents’ depressive symptoms, childhood academic achievement, childhood depressive symptoms, and negative life events. Each of these, except childhood depressive symptoms, uniquely discriminated the high-persistent group from the other three, with parents’ depressive symptoms and negative life events predicting a greater likelihood of being in the high-persistent class and childhood academic achievement predicting a lower likelihood. Childhood depressive symptoms, however, only discriminated the very low group from the high-persistent group, with the effect being in the expected direction. The within class effects on growth were equal across the classes for parents’ depressive symptoms and negative life events. Parents’ depressive symptoms had a significant effect on initial level of symptoms in the expected direction, but no significant effect for slope. Negative life events also had a positive significant association with initial symptom levels, but a significant negative impact on slope. Thus, the negative effects of these factors on depressive symptoms in early adolescence tended to ameliorate over time. Childhood depressive symptoms had a significant association with symptom levels at ages 14–15 years across the classes, but the effects on slope varied across classes (being significant and positive in the very low symptoms group and significant and negative in the other three classes). This indicates that the young men in the lowest symptom class who had higher levels of depressive symptoms in childhood were the most at risk for growth over time in symptoms, whereas young men in the three elevated classes showed some improvement over time. Childhood academic achievement had significant effects in the moderate-decreasing group and high-decreasing group, predicting to lower initial symptom levels and to growth or increase over time in symptom levels. Effects for the very low group and the high-persistent group were nonsignificant.
In prior work (Kim et al., 2003), a synergistic interaction was found, such that there was a significantly stronger association between maternal depressive symptoms and the initial and across time levels of depressive symptoms in families where the father was above the sample median (eight on the CES-D) for depressive symptoms, compared with families where the father was at or below the sample median. The same effect was checked in predicting class membership in the growth mixture models. A similar pattern was found, but it was limited to discriminating Class 1 from Class 4, and it was not strong enough to be significant at the .05 level (p = .13).
Multivariate Prediction Models
In order to identify a more compact set of risk factors for predicting latent class membership and initial status and change within latent class, a series of multivariate predictor models was fitted using the 202 subjects who had complete data on all the predictors except for paternal antisocial behavior. Prediction of latent class was conducted first. All predictors that had significant effects on class membership from the univariate analyses were entered, using the same pattern of equality constraints. A simple backwards elimination procedure was used to arrive at the most parsimonious set of predictors of class membership. In the multivariate model, parents’ depressive symptoms and negative life events uniquely discriminated the high-persistent group from the other classes (χ2 = 7.85, df = 1, p < .01 and χ2 = 6.82, df = 1, p < .01, respectively), and childhood depressive symptoms discriminated the very low and moderate-decreasing groups from the high-persistent group (z = −4.73, p < .001, z = −2.19, p = .03, respectively), but failed to discriminate the high-decreasing group from the high-persistent group (z = 0.36, p = .72).
Once the compact set of class predictors was identified, their effects on initial status and change within class were tested, and the effects of the other predictors that had significant within class regressions in the univariate analyses were added (childhood antisocial behavior and academic achievement). For all predictors, the same pattern of equality constraints as in the univariate analyses was used. Only two variables had unique significant within class effects. Negative life events had a significant positive effect on the intercept and a nonsignificant negative effect on the slope in all classes (z = 3.35, p < .001 and z = −1.32, p = .19, respectively). Childhood depressive symptoms had a significant positive effect on initial status in all classes (z = 4.21, p < .001), a marginally significant positive effect on slope in the very low class (z = 1.90, p = .057), and a significant negative effect on slope in the remaining three classes (z = −4.02, p < .001).
The multivariate analyses differed from the univariate models in two main respects. First, the within class effects of childhood antisocial behavior and academic achievement were eliminated by the within class effects of childhood depressive symptoms and negative life events. Although mediation was not formally tested, it appeared as though these effects were mediated by childhood depressive symptoms and negative life events. Second, childhood depression did not discriminate Class 2 from 4 in the univariate model, but did in the multivariate model. The effect was close to being significant in the univariate models (z = −1.60, p = .11), but failed to make the standard .05, cutoff and marginally significant in the multivariate models (z = −2.19, p = .03). It does appear, however, that including the other predictors somewhat sharpened the effects of childhood depression on class discrimination.
Discussion
In this study, a model with four latent linear growth trajectory classes best captured heterogeneity in the 10-year course of young men’s depressive symptoms from early adolescence to the mid 20’s. The four classes were labeled based on the fitted mean growth curve within each group as (a) high-persistent, (b) high-decreasing, (c) moderate-decreasing, and (d) very low. Consistent with our hypothesis, this finding indicates that there may be heterogeneous subgroups of young men who follow unique trajectories of depressive symptoms from early adolescence through young adulthood. Differences among the three lowest classes in trajectory parameters seemed largely quantitative rather than qualitative. As the level of depressive symptoms over time increased across these groups, the young men showed more variability in levels of depressive symptoms, both within and across time, and more tendency for the levels of symptoms to decrease (i.e., improve). The high-persistent group, however, departed from this pattern. Although the high-persistent class did have the highest time-specific variability, the young men in this class maintained their symptom levels over time, showed no significant variability around slope (i.e., direction of change over time), and showed no association between initial level and change over time. In addition, in the high-persistent class there was a small autoregressive effect indicating some effect of depressive symptoms in the prior period on current levels of symptoms. These findings suggest that the lowest three classes differ from each other in degrees of depressive symptoms and show some recovery from early adolescent symptom levels over time. In contrast, the high-persistent class differed in a qualitative way from the other three classes; not only did they show a higher average level of depressive symptoms, but the high average level was stable over time.
A marked positive relation was found between the mean level and the variability of the depressive symptoms that departs from the standard growth curve model. It could be this feature that was largely responsible for the superior fit of the four-class model, despite the lack of qualitative differences among the three lower classes. It is also possible that psychometric properties of the CES-D partially accounted for the fact that a four-class model fit better than three- or two-class models, as floor effects, skewness, and outliers are departures from normality that can create classes (Bauer & Curran, 2003; Muthén, 2003). However, they were not extreme in these data. Thus, particularly given that the episodic nature of depressive symptoms is well known, the patterns found are likely to be characteristic of longitudinal differences in experiences of depressive symptoms over time, rather than a psychometric artifact of the data.
The probability of a lifetime diagnosis of depression was strongly related to latent class membership, and the high-persistent group had the highest rate. The persistently high average level of depressive symptoms for the high-persistent group and the high time-specific variance, which indicates an episodic pattern for the individuals in the group, suggests an underdiagnosis of lifetime cases at ages 25–26 years. Although it is possible that there can be relatively high symptom severity without meeting the diagnostic criteria, this could also either be due to issues with the DSM-IV diagnostic system or the CIDI interview. It is likely that at least part of the discrepancy is due to poor retrospective recall. It has been suggested that lay-administered diagnostic interviews such as the DIS or CIDI tend to underestimate prevalence rates (Eaton, Neufeld, Chen, & Cai, 2000; Murphy, Monson, Laird, Sobol, & Leighton, 2000). It is also possible that others in the group may meet diagnostic criteria for a depressive disorder in the future. The high-decreasing group also had a relatively high rate of diagnosis of depressive disorders, suggesting that they also deserve attention regarding prevention. Although they did decrease in symptoms levels over time, they were still at an elevated level of depressive symptoms at age 24 years, relative to the two lower groups.5 Future studies should look into the timing of onset of the diagnoses for these two elevated trajectory classes and try to map out course characteristics of symptoms before and after the onset.
One of the unexpected findings was the small proportion of the sample in the very low group (only 5.8%) and the relatively high proportion in the high-persistent group (24.2%). Typically, men are thought to have low rates of depressive symptoms compared to women, but these findings suggest that there is a substantial subgroup of young men who suffer from high rates of recurring symptoms. It could be that the prevalence of high and persistent symptoms is higher for at-risk men than for an unselected group. This is likely given that several family risk factors were associated with membership in the high-persistent trajectory group.
Another somewhat unexpected finding was that there was no adolescent onset trajectory class. This may be partly because the model was estimated over 10 years to the mid 20s rather than just over the adolescent period. In addition, variation around the intercept and slope was allowed within groups; thus, some boys with increasing patterns of symptoms were accommodated within the groups. Studies have suggested that adolescents are at greater risk for depressive symptoms as they experience multiple developmental challenges (e.g., Petersen, Sirigiani, & Kennedy, 1991). However, adolescent onset of depressive symptoms appears to be more prevalent for adolescent girls than for boys (e.g., Cyranowski, Frank, Young, & Shear, 2000), perhaps because girls are either more likely to be exposed to stressful environments or are more sensitive to such stressors (Compas & Wagner, 1991; Ge et al., 1994). It is also possible that there is a subgroup of men who develop depressive symptoms in their late 20’s or early 30’s, and the present study did not extend to this age period. As there are only a few long-term research studies that have followed men into adulthood, it is difficult to know just when men are particularly vulnerable to the development of depressive symptoms. This issue definitely warrants further investigation.
Consistent with the general hypothesis, it was found that some early risk factors predicted only class membership, some predicted only growth within class, and some predicted both. However, the hypothesis that contextual and parental risk factors would predict class membership and individual risk factors would predict change within class over time was only partially supported. Parental transitions and family income predicted only class membership and not growth within classes. Young men’s childhood antisocial behavior and paternal antisocial behavior predicted only growth within classes. Academic achievement, parental depressive symptoms, childhood depressive symptoms, and negative life events predicted class membership and growth within classes. It is possible that paternal antisocial behavior and parents’ depressive symptoms are closely related to interpersonal contexts within which parents’ psychopathology influences their children through poor parenting and poor interactional skills. In addition, poor academic skills, early onset of depressive symptoms, and the experience of multiple negative life events in childhood appear to exert strong influence on the longitudinal course of depressive symptoms for all of the trajectory groups.
In general, risk factors from childhood predicted initial status positively and slope negatively, indicating that the young men showed some recovery over time from the effects of these risk factors, perhaps either due to distance in time from the risk factor (e.g., negative life events), an improvement in the level of the risk factors, or due to decreased exposure to the risk factor. For example, it is normative for youth to spend less time with parents as they mature; thus, parental risk factors may become less influential. Risk factors in childhood may also become less salient with age. Boys who experienced depressive symptoms due to poor academic achievement may later experience success in a manual job that does not require those skills. The only significant exception to the pattern of prediction from risk factors to higher levels of initial status and to some recovery over time was that childhood depressive symptoms predicted some increase over time for the very low class.
An important finding of the study is that four of the significant predictors of depressive trajectory membership uniquely discriminated the high-persistent group from the other three groups, including parental transitions, childhood academic achievement problems, parents’ depressive symptoms, and negative life events. On the other hand, family income and childhood depressive symptoms primarily discriminated the very low from the high-persistent group. Most notably, these two predictors failed to discriminate the moderate-decreasing and the high-decreasing group from the high-persistent group. Thus, the class prediction results strongly support a qualitative distinction between the high-persistent group and the other three trajectory groups. The findings also suggest that the very low class may be qualitatively different from the other classes, although the small size of the very low group, the modest significance levels of the effects, and the lack of qualitative differences in the trajectories themselves make this a tentative finding. These findings strongly suggest that mechanisms related to the development of such symptoms should be understood with respect to different lifetime trajectories.
Results for the multivariate prediction models indicated that only three predictors uniquely contributed to class discrimination, namely parents’ depressive symptoms, negative life events, and childhood depressive symptoms. The former two uniquely discriminated the high-persistent class from the other three classes, but the latter discriminated the high-persistent from the very low class and the moderate-decreasing class only. The latter two factors also predicted initial status or change within classes. The effects of childhood depressive symptoms on slope interacted with latent class, such that it positively and significantly predicted growth for the low group but negatively and significantly predicted growth in the other three classes. Although many studies have consistently indicated strong associations of these factors with the continuity of depressive symptoms in young adulthood (Harrington, Rutter, & Fombonne,1996), most of the studies were based on a variable-centered approach and consequently were unable to address differential vulnerability to risk factors for individuals with different depressive trajectories. The unique aspect of the present study is that findings showed more specific prediction effects associated with the development of depressive symptoms in young men.
The nature of the mechanism through which parents’ depressive symptoms, men’s childhood depressive symptoms, and negative life events operate to predict trajectory membership and longitudinal changes within each trajectory remain unclear. Parental depressive symptoms are known as significant risk factors for their children’s longer-term vulnerability to high levels of similar symptoms (e.g., Downey & Coyne, 1990). However, to what extent this effect is due to direct genetic effects, to direct learning, or to some mediated effect, such as through a poor parent-child relationship, cannot be answered from our study. Replication and extension of the findings of the present study to samples representative of populations with differing characteristics is necessary. Given the nature of the present sample (i.e., at-risk for antisocial behavior), generalizability of the findings might be limited. Using the CES-D, Garrison et al. (1990) reported mean levels of 11.66 through 13.98 for White male high school students. The overall mean levels of the present sample over the 10 years (from 7.71. to 11.33) are somewhat lower than that of Garrison et al’s. However, few studies have examined depressive symptoms of adolescent males through young adulthood, therefore, it is difficult to evaluate the present findings with respect to other studies in terms of relative levels of depressive symptoms over an extended time. Furthermore, it is likely that the number and pattern of depressive trajectories identified in the study were limited because of the relatively small sample size, although Sampson, Laub, and Eggleston (2004) found that estimates of the number of classes tended to stabilize at an N of around 200. Future studies should try to extend to culturally and ethnically diverse samples as well as to women. In addition, the depressive trajectory in the present study started at ages 14-15 years and did not include childhood, an important period for the development of depressive symptoms. Extension to younger ages would provide a more complete picture of the developmental course of men’s depressive symptoms. Future studies are also encouraged to use a variety of different measures of depressive symptoms.
The present study did not test any specific theory regarding the associations of stress to depressive symptoms. However, findings from our study can be used to refine the extant theories. It is possible to test different diathesis-stress models for different subgroups. Some of the diatheses could be unique to some groups, some could be common across two or more subgroups, and the same could be true for the stressors. Such an effort can also help clinicians to identify individuals at different levels of risk and accordingly to develop treatment programs. Lastly, the study did not include any time-varying covariates, such as negative life events or social support. Certainly early risk factors cannot fully explain the longitudinal course of men’s depressive symptoms. It is possible that the youths’ subsequent experiences during adolescence and young adulthood are uniquely related to trajectory membership and growth within each group. Proximal time-varying factors would enhance our understandings of the developmental courses of depressive symptoms.
It is possible that some of the parental influences on the men’s depressive symptoms could have been underestimated because of the way the parental predictors were constructed in this study. Indicators for parents’ depressive symptoms were taken from a self-reported measure of depressive symptoms (e.g., CES-D) assessed at three waves rather than from lifetime diagnostic interviews. Therefore, the actual level of parental depressive symptoms and its association with the men’s depressive symptoms may have been underestimated.
Despite these limitations, this study is the first, to our knowledge, to study diverse longitudinal trajectories of depressive symptoms and to examine childhood risk factors predicting the class membership as well as within class development. Harrington and colleagues (Harrington et al., 1996) called for a need to examine whether there are subgroups of individuals that have particularly strong continuities into adulthood. However, because of the lack of efforts to differentiate distinctive depressive trajectories, particularly for men, little is known about prototypical subgroups of individuals with similar trajectories. The present study represents a potentially important first step toward identification of subgroups of individuals who follow similar trajectories of depressive symptoms. The fact that there are multiple depressive trajectory subgroups and that different factors are related to the trajectory membership and growth within each class calls for the need to further refine our theories as well as treatment programs. Researchers and clinicians should be aware of the possibility that individuals with depressive symptoms are developmentally heterogeneous. Ignoring this issue could obscure important differences among individuals, which then can render ineffective design of prevention or intervention programs. It is our belief that findings from the study provide interesting insight for future study that can improve the current knowledge on the long-term depressive trajectories. An important next step includes the examination of differential outcomes for each trajectory.
Footnotes
Garrison, Addy, Jackson, McKeown, and Waller (1991) have suggested that a cutoff point of 12 on the CES-D can be used as the best predictive value when it is used as a screen for major depression among adolescent boys in community samples. However, we chose a rather more conservative cutoff point of 16.
Estimation of mixture models are affected by the presence of local solutions, which appear to computer search algorithms to be the best solution (i.e., maximized likelihood), when other solutions may exist that have higher likelihoods. To prevent this, the start values were perturbed randomly to initiate the search from 100 different locations of the parameter space.
The Lo, Mendell, and Rubin (2001) procedure indicated significant improvements with the added class for the two- versus one-class model (p < .0001), the three- versus two-class model (p = .0218), and the four- versus three-class model (p = .0155). However, due to numerical problems in the five-class model, this procedure could not be used to compare the fully parameterized four- and five-class models. The five-class model was simplified by removing two nonsignificant growth factor variances and the associated covariances, and this model readily converged. The BIC and Lo et al. procedure, however, indicated the simplified five-class model was not significantly better than the four-class model. Thus, the four-class solution was selected.
For parsimony, the four-class model was then trimmed in two steps. First, by removal of nonsignificant variance and covariance components from each class and, second, by removal of nonsignificant autoregressive parameters. None of the remaining estimated parameters went from being nonsignificant to significant (at p < .05) or vice versa as a result of trimming.
The mean curve represents the average group trajectory when within class variability is allowed. Individual’s true trajectories may deviate from the average. When within class variability is not allowed, then the mean curve represents the “true” curve for each individual in the group. Because we allowed within class variability as the evidence seemed to indicate it was important, the interpretation varies according to whether within class variability is allowed in a particular class or not. In the specific case of the high-persistent group, we allowed within class variation on the single growth curve factor that represented their average level across time. Thus, not all individuals had the same “true” average level over time; some were higher and some were lower, and the average curve is the average of all the individuals in the class. Time-specific influences represent both measurement error and real depressive symptoms that are peculiar to a particular point in time. So the mean curve is the true developmental curve, whereby developmental we mean long-term change over time, subject to the caveats given above.
Support for the Oregon Youth Study was provided by Grant R37 MH 37940 from the Prevention, Early Intervention, and Epidemiology Branch, National Institute of Mental Health (NIMH), U.S. Public Health Service (PHS). Support for the Couples Study was provided by Grant HD 46364 from the National Institute of Child Health and Human Development (NICHD) and National Institute on Drug Abuse (NIDA), National Institutes of Health (NIH),U.S. PHS. Support for the Three Generational Study was provided by Grant DA 015485 from NIDA and NICHD, U.S. PHS. Support was also provided by Grant P30 MH 46690 Prevention, Early Intervention, and Epidemiology Branch, NIMH, U.S. PHS. We thank Jane Wilson, Rhody Hinks, and the data collection staff for their commitment to high quality data and Sally Schwader for editorial assistance.
References
- Achenbach TM, Edelbrock SS. Burlington: Department of Psychology, University of Vermont.; 1983. Manual for the Child Behavior Checklist and the revised Child Behavior Profile. [Google Scholar]
- American Psychiatric Association. 4th ed. Washington, DC: Author; 1994. Diagnostic and statistical manual of mental disorders. [Google Scholar]
- Anderson JC, Williams S, McGee R, Silva PA. DSM-III disorders in preadolescent children: Prevalence in a large sample from the general population. Archives of General Psychiatry. 1987;44:69–77. doi: 10.1001/archpsyc.1987.01800130081010. [DOI] [PubMed] [Google Scholar]
- Bandeen-Roche K, Miglioretti DL, Zeger SL, Rathouz PJ. Latent variable regression for multiple discrete outcomes. Journal of the American Statistical Association. 1997;92:1375–1386. [Google Scholar]
- Bauer DJ, Curran PJ. Overextraction of latent trajectory classes: Much ado about nothing? Reply to Rindskopf (2003), Muthén (2003), and Cudeck and Henly (2003) Psychological Methods. 2003;8:384–393. doi: 10.1037/1082-989X.8.3.338. [DOI] [PubMed] [Google Scholar]
- Birleson P. The validity of depressive disorder in childhood and the development of a self-rating scale: A research report. Journal of Child Psychology and Psychiatry. 1981;22:73–88. doi: 10.1111/j.1469-7610.1981.tb00533.x. [DOI] [PubMed] [Google Scholar]
- Brown GW. The role of life events in the aetiology of depressive and anxiety disorders. In: SC Stanford, P Salmon., editors. Stress: From synapse to syndrome. San Diego, CA: Academic Press; 1993. pp. 23–50. [Google Scholar]
- Bushway SD, Thornberry TP, Krohn MD. Desistance as a developmental process: A comparison of static and dynamic approaches. Journal of Quantitative Criminology. 2003;19:129–153. [Google Scholar]
- Capaldi DM. The co-occurrence of conduct problems and depressive symptoms in early adolescent boys: I. Familial factors and general adjustment at Grade 6. Development and Psychopathology. 1991;3:277–300. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi DM. The co-occurrence of conduct problems and depressive symptoms in early adolescent boys: II. A 2-year follow-up at Grade 8. Development and Psychopathology. 1992;4:125–144. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi DM, Patterson GR. An approach to the problem of recruitment and retention rates for longitudinal research. Behavioral Assessment. 1987;9:169–177. [Google Scholar]
- Capaldi DM, Stoolmiller M. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: III. Prediction to young-adult adjustment. Development and Psychopathology. 1999;11:59–84. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Chen L, Eaton WW, Gallo JJ, Nestadt G. Understanding the heterogeneity of depression through the triad of symptoms, course, and risk factors: A longitudinal, population-based study. Journal of Affective Disorders. 2000;59:1–11. doi: 10.1016/s0165-0327(99)00132-9. [DOI] [PubMed] [Google Scholar]
- Chung IJ, Hill KG, Hawkins JD, Gilchrist LD, Nagin DS. Childhood predictors of offense trajectories. Journal of Research in Crime and Delinquency. 2002;39:60–90. [Google Scholar]
- Cicchetti D, Toth SL. The development of depression in children and adolescents. American Psychologist. 1998;53:221–241. doi: 10.1037//0003-066x.53.2.221. [DOI] [PubMed] [Google Scholar]
- Compas BE, Wagner BM. Psychosocial stress during adolescence: Intrapersonal and interpersonal processes. In: Colten ME, Gore S, editors. Adolescent stress: Causes and consequences. Social institutions and social change. New York: Aldine de Gruyter; 1991. pp. 67–85. [Google Scholar]
- Cyranowski JM, Frank E, Young E, Shear K. Adolescent onset of the gender difference in lifetime rates of major depression: A theoretical model. Archives of General Psychiatry. 2000;57:21–27. doi: 10.1001/archpsyc.57.1.21. [DOI] [PubMed] [Google Scholar]
- Downey G, Coyne JC. Children of depressed parents: An integrative review. Psychological Bulletin. 1990;108:50–76. doi: 10.1037/0033-2909.108.1.50. [DOI] [PubMed] [Google Scholar]
- Duncan GJ, Brooks-Gunn J, Klebanov PK. Economic deprivation and early childhood development. Special Issue: Children and poverty. Child Development. 1994;65:296–318. [PubMed] [Google Scholar]
- Eaton WW, Neufeld K, Chen LS, Cai G. A comparison of self-report and clinical diagnostic interviews for depression. Archives of General Psychiatry. 2000;57:217–222. doi: 10.1001/archpsyc.57.3.217. [DOI] [PubMed] [Google Scholar]
- Garber J, Keiley MK, Martin NC. Developmental trajectories of adolescents’ depressive symptoms: Predictors of change. Journal of Consulting and Clinical Psychology. 2002;70:79–95. doi: 10.1037//0022-006x.70.1.79. [DOI] [PubMed] [Google Scholar]
- Garrison CZ, Addy CL, Jackson KL, McKeown RE, Waller JL. The CES-D as a screen for depression and other psychiatric disorder in adolescents. Journal of American Academy of Child and Adolescent Psychiatry. 1991;30:636–641. doi: 10.1097/00004583-199107000-00017. [DOI] [PubMed] [Google Scholar]
- Garrison CZ, Jackson KL, Marsteller F, McKeown R, Addy C. A longitudinal study of depressive symptoms in young adolescents. Journal of American Academy of Child and Adolescent Psychiatry. 1990;29:581–585. doi: 10.1097/00004583-199007000-00011. [DOI] [PubMed] [Google Scholar]
- Ge X, Conger RD, Elder GH., Jr Pubertal transition, stressful life events and the emergence of gender differences in adolescent depressive symptoms. Developmental Psychology. 2001;37:404–417. doi: 10.1037//0012-1649.37.3.404. [DOI] [PubMed] [Google Scholar]
- Ge X, Lorenz FO, Conger R, Elder GH, Jr, Simons R. Trajectories of stressful life events of depressive symptoms during adolescence. Developmental Psychology. 1994;30:467–483. [Google Scholar]
- Hammen C, Rudolph KD. Childhood depression. In: EJ Mash, RA Barkley., editors. Child psychopathology. New York: Guilford Press; 1996. pp. 153–195. [Google Scholar]
- Harrington R, Fudge H, Rutter M, Pickles A. Adult outcomes of childhood and adolescent depression: II. Links with antisocial disorders. Journal of the American Academy of Child and Adolescent Psychiatry. 1991;30:434–439. doi: 10.1097/00004583-199105000-00013. [DOI] [PubMed] [Google Scholar]
- Harrington R, Rutter M, Fombonne E. Developmental pathways in depression: Multiple meanings, antecedents, and endpoints. Development and Psychopathology. 1996;8:601–616. [Google Scholar]
- Jaffee SR, Moffitt TE, Caspi A, Fombonne E, Poulton R, Martin J. Differences in early childhood risk factors for juvenile-onset and adult-onset depression. Archives of General Psychiatry. 2002;59:215–222. doi: 10.1001/archpsyc.59.3.215. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Eaves LJ, Walters EE, Neale MC, Heath AC, Kessler RD. The identification and validation of distinct depressive syndromes in a population-based sample of female twins. Archives of General Psychiatry. 1996;53:391–399. doi: 10.1001/archpsyc.1996.01830050025004. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Magee WJ. Childhood adversities and adult depression: Basic patterns of association in a US national survey. Psychological Medicine. 1993;23:679–690. doi: 10.1017/s0033291700025460. [DOI] [PubMed] [Google Scholar]
- Kim HK, Capaldi DM, Stoolmiller M. Depressive symptoms across adolescence and young adulthood in men: Prediction from parental and contextual risk factors. Development and Psychopathology. 2003;15:469–495. doi: 10.1017/s0954579403000257. [DOI] [PubMed] [Google Scholar]
- Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Moffitt TE, Caspi A, Harrington H, Milne B. Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26 years. Development and Psychopathology. 2002;14:179–207. doi: 10.1017/s0954579402001104. [DOI] [PubMed] [Google Scholar]
- Murphy JM, Monson RR, Laird NM, Sobol AM, Leighton AH. A comparison of diagnostic interviews for depression in the Stirling County Study. Archives of General Psychiatry. 2000;57:230–236. doi: 10.1001/archpsyc.57.3.230. [DOI] [PubMed] [Google Scholar]
- Muthén BO. Statistical and substantive checking in growth mixture modeling: Comment on Bauer and Curran (2003) Psychological Methods. 2003;8:369–377. doi: 10.1037/1082-989X.8.3.369. [DOI] [PubMed] [Google Scholar]
- Muthén BO, Muthén LK. Integrating person-centered and variable-centered analysis: Growth mixture modeling with latent trajectory classes. Alcoholism: Clinical and Experimental Research. 2000;24:882–891. [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 3rd ed. Los Angeles: Muthén & Muthén; 1998–2004. [Google Scholar]
- Muthén BO, Shedden K. Finite mixture modeling with mixture outcomes using the EM algorithm. Biometrics. 1999;55:463–469. doi: 10.1111/j.0006-341x.1999.00463.x. [DOI] [PubMed] [Google Scholar]
- Nagin D. Analyzing developmental trajectories: A semiparametric, group-based approach. Psychological Methods. 1999;4:139–157. doi: 10.1037/1082-989x.6.1.18. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoesksema S, Girgus JS, Seligman ME. Predictors and consequences of childhood depressive symptoms: A 5-year longitudinal study. Journal of Abnormal Psychology. 1992;101:405–422. doi: 10.1037//0021-843x.101.3.405. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Bank L. Bootstrapping your way in the nomological thicket. Behavioral Assessment. 1986;8:49–73. [Google Scholar]
- Petersen AC, Sirigiani PA, Kennedy RE. Adolescent depression: Why more girls? Journal of Youth and Adolescence. 1991;20:247–271. doi: 10.1007/BF01537611. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Sampson RJ, Laub JH, Eggleston EP. On the robustness and validity of groups. Journal of Quantitative Criminology. 2004;1:37–42. [Google Scholar]
- Sullivan PF, Kessler RC, Kendler KS. Latent class analysis of lifetime depressive symptoms in the National Comorbidity Survey. American Journal of Psychiatry. 1998;155:1398–1406. doi: 10.1176/ajp.155.10.1398. [DOI] [PubMed] [Google Scholar]
- Swearingen EM, Cohen LH. Measurements of adolescent’s life events: The Junior High Life Experience Survey. American Journal of Community Psychology. 1985;13:69–85. doi: 10.1007/BF00923260. [DOI] [PubMed] [Google Scholar]
- Wittchen HU, Robins LN, Cottler LB, Sartorius N, Burke JD, Regier DA. Cross-cultural feasibility, reliability and sources of variance of the Composite International Diagnostic Interview (CIDI) British Journal of Psychiatry. 1991;159:645–653. doi: 10.1192/bjp.159.5.645. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Geneva, Switzerland: Author; 1992. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. [Google Scholar]
- World Health Organization. Geneva, Switzerland: Author; 1993. The ICD-10 classification of mental and behavioural disorders: Diagnostic criteria for research. [Google Scholar]
- World Health Organization. Geneva, Switzerland: Author; 1997. Composite International Diagnostic Interview (CIDI). Core version 2.1. [Google Scholar]