

Abstract
Obstructing lesions of the trachea and larynx which cause a predominantly inspiratory obstruction can be satisfactorily diagnosed by measuring both F.I.V.1 and F.E.V.1. Chronic airways obstruction involving intrathoracic airways produces a much lower F.E.V.1/F.I.V.1 percentage than normal, whereas obstruction to larynx and trachea causes a raised F.E.V.1/F.I.V.1 percentage. If flow-volume measurements are not available the F.E.V.1/F.I.V.1 percentage should provide a simple and useful method for diagnosis of upper airways obstruction.
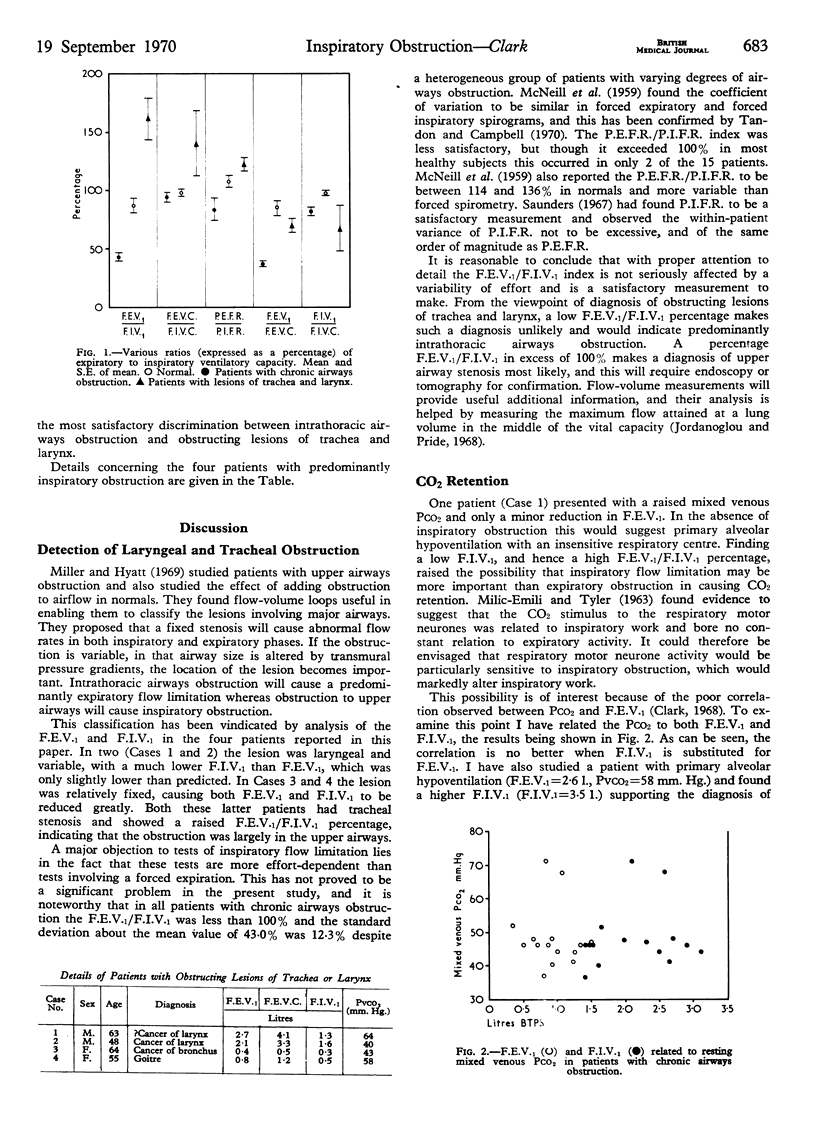
In one of the patients reported a predominantly inspiratory obstruction caused CO2 retention. In patients with airways obstruction the correlation between Pco2 and F.I.V.1 was found to be the same as between Pco2 and F.E.V.1. This suggests that respiratory failure can be caused by either inspiratory or expiratory airways obstruction and that neither is of greater importance in producing CO2 retention.
Full text
PDF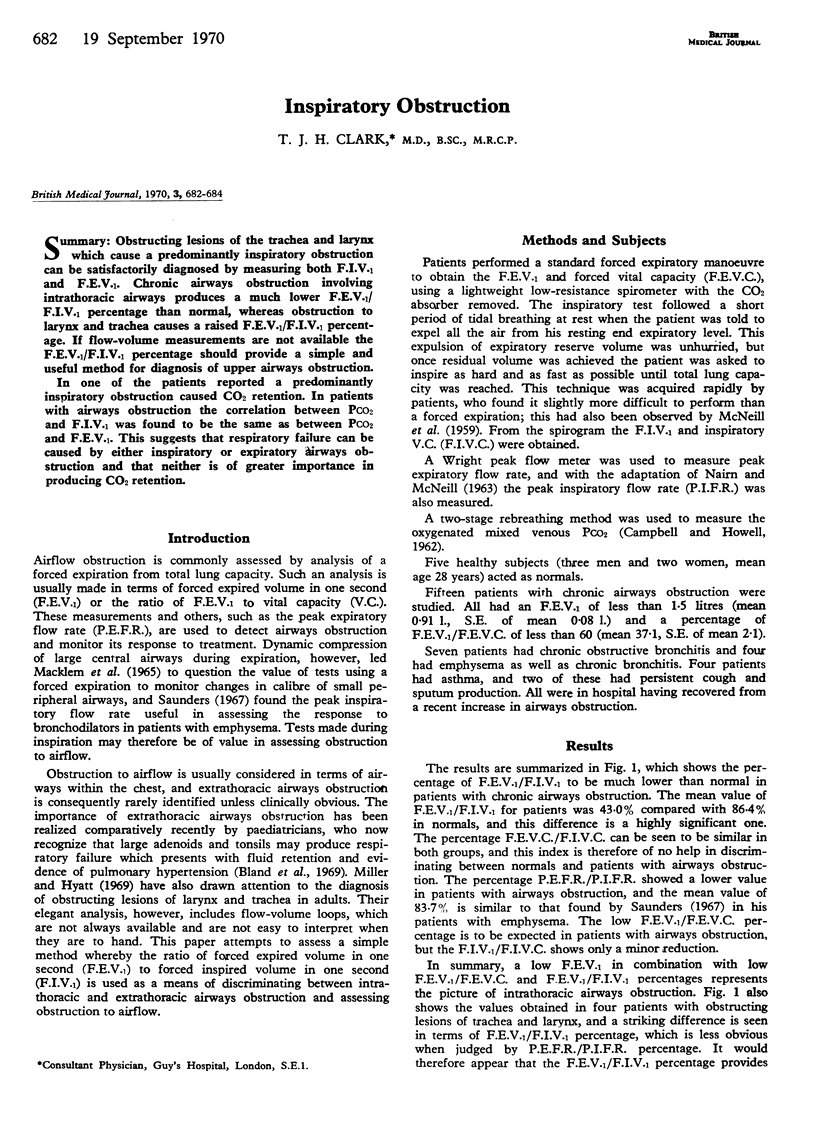
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bland J. W., Jr, Edwards F. K. Pulmonary hypertension and congestive heart failure in children with chronic upper airway obstruction. New concepts of etiologic factors. Am J Cardiol. 1969 Jun;23(6):830–837. doi: 10.1016/0002-9149(69)90378-6. [DOI] [PubMed] [Google Scholar]
- CAMPBELL E. J., HOWELL J. B. Rebreathing method for measurement of mixed venous PCO2. Br Med J. 1962 Sep 8;2(5305):630–633. doi: 10.1136/bmj.2.5305.630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jordanoglou J., Pride N. B. A comparison of maximum inspiratory and expiratory flow in health and in lung disease. Thorax. 1968 Jan;23(1):38–45. doi: 10.1136/thx.23.1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MACKLEM P. T., FRASER R. G., BROWN W. G. BRONCHIAL PRESSURE MEASUREMENTS IN EMPHYSEMA AND BRONCHITIS. J Clin Invest. 1965 Jun;44:897–905. doi: 10.1172/JCI105206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller R. D., Hyatt R. E. Obstructing lesions of the larynx and trachea: clinical and physiologic characteristics. Mayo Clin Proc. 1969 Mar;44(3):145–161. [PubMed] [Google Scholar]
- NAIRN J. R., McNEILL R. S. Adaptation of the Wright peak flow meter to measure inspiratory flow. Br Med J. 1963 May 18;1(5341):1321–1323. doi: 10.1136/bmj.1.5341.1321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saunders K. B. Bronchodilator response patterns in patients with chronic airways obstruction: use of peak inspiratory flow rate. Br Med J. 1967 May 13;2(5549):399–402. doi: 10.1136/bmj.2.5549.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tandon M. K., Campbell A. H. Variability of relaxed expiratory volume and forced inspiratory volume. Thorax. 1970 Mar;25(2):178–179. doi: 10.1136/thx.25.2.178. [DOI] [PMC free article] [PubMed] [Google Scholar]