

Caucasian Communities
Age-related macular disease (AMD) accounts for about 50% of registered blindness in England and Wales, and this high prevalence is likely to exist in all economically developed Caucasian communities. A recent analysis indicates that the prevalence appears to be increasing at a rate not fully explained by the increasing age of the population, and, as a cause of visual loss, AMD is as common now as diabetes and glaucoma during working life.1 Despite the early expectations, it is now evident that the present techniques of laser treatment will not have a major impact on blindness due to AMD.2 Other forms of treatment are under trial, such as ionising radiation and photodynamic therapy, but they may not be vastly more successful than photocoagulation. This means that our knowledge of the behaviour and pathogenesis of the disorder must be re-examined in the hope that alternative approaches to management can be identified.
Twin and sibling studies provide good evidence of genetic predisposition in AMD, and it is believed that the predisposition becomes manifest in the presence of appropriate environmental influences. It is likely that more than one gene is involved although the number is probably small. In these respects AMD is similar to other complex traits. It follows that ageing at the macula would vary qualitatively within a community, occurring in those with the most severe genetic predisposition and environmental pressures. The high prevalence of clinically detectable age-related maculopathy (ARM) in those over the age of 65 years implies that the causative genes are common in industrial societies.
Non-Caucasian Communities
In the past AMD was rarely recognised in Japan. However, disability due to macular disease in middle or late life,3 and hospital referrals with this disorder, suggest that AMD has become common in the last two decades, at least in urban communities. A similar trend is appearing in other parts of Eastern Asia. There is also a strikingly high prevalence of macular disease in elderly Inuit in Greenland.
The phenotype (clinical appearance) of AMD appears to vary in different communities. In Japan the impression is that poly-poidal choroidopathy is common, whereas, in Caucasians, the growth of new vessels is the most prevalent complication. In the Inuit population the characteristic process is atrophy. In both Inuit and Japanese the visual loss occurs without there being preexisting recognisable age changes at the level of Bruch's membrane, such as soft drusen. In neither has genetic predisposition been sought so far, although the increasing incidence implies environmental factors are important.
Future Research
Cross sectional studies in populations with different genetic backgrounds but similar environment, and populations with similar genetic background with different environments, would serve to prove that both influences are important.
Future research seeking the abnormal genes is likely to be rewarding. The techniques of linkage dysequilibrium and sibling pair analysis have been well worked out, and have met with success in other complex disorders such as multiple sclerosis, diabetes, bipolar illness and schizophrenia. Both investigative techniques benefit from knowledge of candidate genes. Candidate genes may be found by recognition of associated characteristics, such as loss of iris colour,4 or identification of genes causing disorders with phenotypic similarities to AMD such as Sorsby fundus dystrophy and Doyne macular dystrophy, together with knowledge of the disease processes.
In Caucasians visual loss results from choroidal neovascularization, detachment of the retinal pigment epithelium (RPE) or geographic atrophy. It is widely believed that these occur in response to accumulation of debris in Bruch's membrane, which is recognised clinically as drusen and pigmentary changes referred to as age-related maculopathy (ARM). It is believed that the debris in Bruch's membrane is derived from the RPE, which discharges cytoplasmic material throughout life into the inner portion of Bruch's membrane in order to achieve cytoplasmic renewal. It is likely that the material is cleared through the choriocapillaris. Some information exists concerning age changes in the RPE, Bruch's membrane and choroid from laboratory studies of donor eyes. However, the inter-relationship between age change in the different tissues is not established. Clinical and laboratory studies imply that the quantity, distribution and chemical composition of the debris determine both the magnitude of risk, and the type of lesion causing visual loss. From these observations it is possible to speculate on the potential genetic influences that may modulate ageing. Increased outer segment turnover may explain the high levels of RPE autofluorescence in diseases due to mutations in the RDS gene. A similar effect may occur if there is reduced activity of RPE degradative enzymes, or free radical damage to the substrate of degradation. Age change in Bruch's membrane such as cross linkage of collagen would predictably accelerate accumulation of debris. The mechanisms whereby material is cleared from Bruch's membrane may also be under genetic influence. Considerable variation of age changes exists from one donor to another of a similar age, reflecting the complexity of genetic and environmental influences.
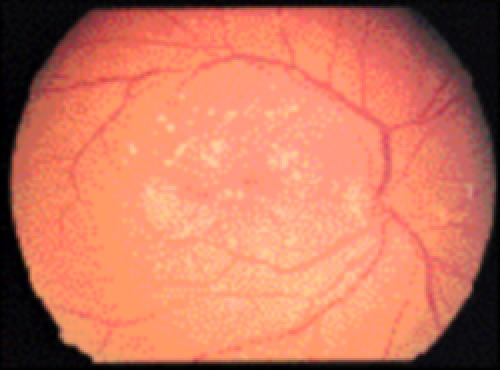
Drusen and macular disease
Photo: Clare Gilbert
Thus, there are potentially many candidate genes influencing ageing at the macula. Whether or not a single gene determines risk in an individual or family is unknown, although the reputed high gene frequency in the population implies that a single gene should not be assumed.
Of the environmental influences smoking has most consistently been associated with increased risk, but surprisingly not all studies have demonstrated this. Dietary intake of carotenoids, other micronutrients and hypertension have also been implicated. However, none of these readily explain the apparent increase in prevalence of disease with change of life style, suggesting that the most important factors have not yet been identified.
In non-Caucasians relatively little information is available on AMD. There is a need to determine whether or not there is genetic predisposition. The natural history of disease has not been documented. In addition, those structural changes predisposing to visual loss are unknown. They have not been documented in any detail clinically, and there is little histopathological documentation of ageing at the posterior pole. It is important that studies of AMD in Caucasian societies should now be repeated in Eastern Asia.
What benefits would there be from this new information? Defining the genetic influences would point to the relevant pathogenic mechanisms involved, and identify those at high risk of visual loss. If the environmental pressures conferring risk were known, public health measures could be taken. New therapeutic measures may come to light, and those most likely to benefit from such measures would be identified. The high prevalence of the disease in Caucasian communities, and the apparent rise in the prevalence in communities previously not considered to be at risk, highlight the urgency for an increasing level of research. Over the last 5 years there has been steadily increasing research activity investigating the pathogenesis of AMD, and the hope is that this continues.
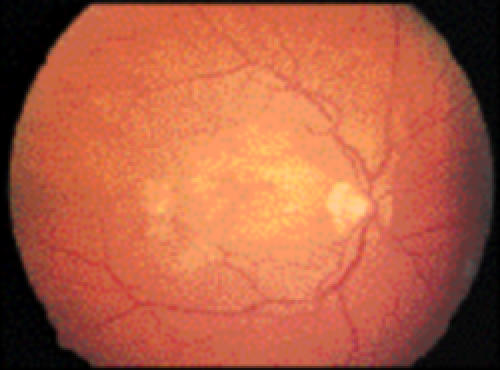
Early subretinal neovascular membrane in a Caucasian eye
Photo: Clare Gilbert
References
- 1.Evans J, Wormald R. Is the incidence of registrable age-related macular degeneration increasing? Br J Ophthalmol. 1996;80:9–14. doi: 10.1136/bjo.80.1.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Macular Photocoagulation Group Argon laser photocoagulation for neovascular maculopathy: three year results for randomized clinical trials. Arch Ophthalmol. 1986;224:493–501. [PubMed] [Google Scholar]
- 3.Yuzawa M, Hagita K, Egawa T, Minato H, Matsui M. Macular lesions predisposing to senile disciform macular degeneration. Jpn J Ophthalmol. 1991;35:87–95. [PubMed] [Google Scholar]
- 4.Holz FG, Piguet B, Minassian DC, Bird AC, Weale RA. Decreasing stromal iris pigmentation as a risk factor for age-related macular degeneration. Am J Ophthalmol. 1994;117:19–23. doi: 10.1016/s0002-9394(14)73010-7. [DOI] [PubMed] [Google Scholar]