

Aim
To describe Cataract Surgical Coverage (CSC) as an indicator to measure the impact of cataract intervention programmes.
Methods and Materials
Cataract Surgical Coverage, both for ‘eyes’ as well as ‘persons’, was calculated from community based surveys conducted in 19 rural districts in the south-west and one urban district in the north-west of India.
Results
Cataract Surgical Coverage (VA<3/60) ranged from 42% to 68% (for persons) and from 22% to 45% (for eyes) in 19 districts of Karnataka State. The coverage for males was higher than for females. In Ahmedabad the coverage was high with 93% for persons and 83% for eyes.
Discussion
Together with prevalence data, Cataract Surgical Coverage can provide important information on the impact of cataract intervention programmes. Regular assessment of prevalence and coverage indicators through focused community surveys will reveal trends. Coverage indicators are also important as input data for mathematical models to predict future trends in cataract blindness.
Introduction
Cataract is a public health problem in many developing countries, including India. Traditionally, the cataract intervention programme is evaluated by the number of cataract operations performed per year. In India this has increased from 1.2 million in 1989 to 2.7 million operations in 1996.1 However impressive this increase may be, the figure does not indicate the extent to which the problem of cataract blindness has been reduced.
Two indicators are used to measure impact. First, it can be measured by a change in prevalence of cataract blindness, obtained through community based surveys. Since blindness surveys are costly and lengthy exercises, these are not conducted regularly. In India, a national study was done in the period 1971–74 and a National Survey on Blindness in 1986–89. The variation in prevalence of blindness and visual impairment due to cataract over this period indicates the impact surgical services have had on the magnitude of the problem.

Advanced cataract, left eye, in Sri Lanka
Photo:Victoria Sheffield
The second indicator to measure impact is Cataract Surgical Coverage (CSC).2,3 This community based parameter compares the proportion who have received surgery (aphakic) to the total, who still need or have had surgery (aphakic + operable cataract) in a certain area. It indicates to what extent the services have covered the needs. It measures the effectiveness of the cataract intervention programme in providing surgical services and, as such, it is an output indicator and does not measure the quality of cataract intervention.
This article presents Cataract Surgical Coverage data obtained through specially designed rapid assessments from two areas in India.
Methods and Materials
We have conducted a simple community based rapid assessment at district level in India, using a systematic random cluster sampling technique. These assessments focused on persons of 50 years and older only. The National Survey on Blindness, India, indicated that of all age-related cataract blindness, 95% occurs in the age group of 50 years and older. Using data obtained from persons of 50 years and older only may slightly underestimate the actual coverage.

Before cataract surgery in Somalia
Photo: Murray McGavin
The survey methodology and detailed results of the first study have been reported elsewhere.4,5 In 1995, these rapid assessments were conducted in 19 districts of Karnataka State in the south west of India, covering a total of 21,950 persons, and in 1997 in the predominantly urban district of Ahmedabad in Gujarat, covering 1962 persons.6 The main indicators collected through these rapid assessments are the prevalence of bilateral and unilateral blindness or (severe) visual impairment due to cataract and the prevalence of bilateral and unilateral aphakia. From these two statistics the Cataract Surgical Coverage (CSC) can be calculated.

After eye camp cataract surgery in India
Photo: Murray McGavin
Eligibility for cataract surgery also depends upon visual acuity and varies between institutions and surgeons. It may be better to use the term ‘operable cataract’ and define the level of visual acuity as follows:
- VA<3/60: cataract blind eye or patient
- VA<6/60: severely visually impaired operable cataract eye or patient
- VA<6/18: visually impaired operable cataract eye or patient
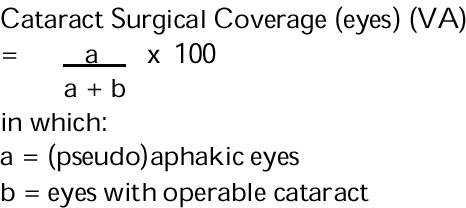
The Cataract Surgical Coverage can be measured in two ways, as shown in Figs. 1 and 2:
Fig. 1.
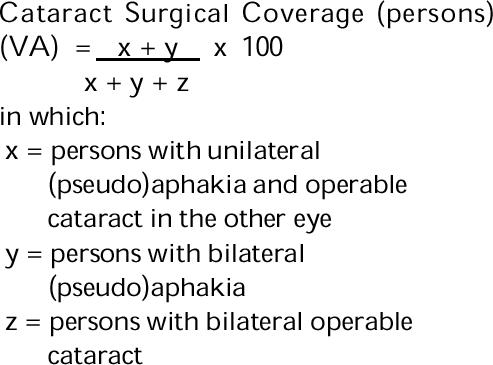
Fig. 2.
In the equation in Fig. 1, we include bilateral operable cataract which can be defined as either VA<3/60, VA<6/60 or VA<6/18, bilateral aphakia and unilateral aphakia with an operable cataract in the other eye. (Persons with unilateral aphakia, in whom the other eye does not have an operable cataract, are excluded from the equation. Such persons do not have bilateral blindness or (severe) visual impairment due to cataract and are therefore not included in the denominator.)
In most cases, it is not possible to assess in retrospect whether patients with (pseudo)aphakia were actually blind (VA<3/60), severely visually impaired (VA<6/60) or visually impaired at the time of surgery. For that reason it is important to calculate the cataract surgical coverage for all three levels of visual acuity.
The equation in Fig. 2 gives an indication of the proportion of eyes with operable cataract that have had surgery in the community at a given point in time.
The Cataract Surgical Coverage can be calculated directly from the sample data, or from the projected district data, after adjusting the sample data for age and sex. Software has been developed for these rapid assessments. It gives CSC(persons) and CSC(eyes) for VA<3/60, VA<6/60 or VA<6/18, for total population and males/females separately.
Results
Data from the rapid assessments on the prevalence of cataract blindness and Cataract Surgical Coverage from Karnataka State are given in Table 1 and Table 2.
Table 1.
Cataract Surgical Coverage from Sample Data on Operable Cataract and Aphakia in 19 Districts in Karnataka (1995)
| Category | Condition | VA<3/60 | VA<6/60 | VA<6/18 | ||
|---|---|---|---|---|---|---|
| ∗b is defined as all eyes with cataract causing an acuity of less than 3/60, 6/60 or 6/18. | ||||||
| ∗∗a is defined as all eyes which are aphakic or (pseudo)aphakic, regardless of acuity. | ||||||
| z | No. persons with bilateral operable cataract | 1,157 | 2,143 | 4,345 | ||
| y | No. persons bilaterally (pseudo)aphakic | 558 | 558 | 558 | ||
| x | No. persons one eye aphakic + one eye operable cataract | 755 | 877 | 988 | ||
| b∗ | No. operable cataract eyes∗ | 4,481 | 6,844 | 11,511 | ||
| a∗∗ | No. (pseudo)aphakic eyes∗∗ | 2,401 | 2,401 | 2,401 | ||
| % | first eyes: | 76.8% | (a-y)/a | |||
| % | second eyes: | 23.2% | y/a | |||
| Cataract Surgical Coverage (eyes) | a/(a+b) | 34.9% | 26.0% | 17.3% | ||
| Cataract Surgical Coverage (persons) | (x+y)/(x+y+z) | 53.2% | 40.1% | 26.2% | ||
Table 2.
Prevalence of Bilateral Cataract Blindness and Cataract Surgical Coverage (VA<3/60) in Eyes and Persons of 50 Years and Older
| District | Prevalence bilateral cataract blindness in persons 50+ | Cataract surgical coverage in eyes of persons 50+ | Cataract surgical coverage in persons 50+ | ||||||
|---|---|---|---|---|---|---|---|---|---|
| males | females | persons | males | females | persons | males | females | persons | |
| Bangalore-R | 3.22% | 5.59% | 4.33% | 36% | 28% | 32% | 55% | 43% | 47% |
| Belgaum | 2.61% | 5.00% | 3.79% | 42% | 39% | 40% | 65% | 57% | 60% |
| Bellary | 4.77% | 7.19% | 6.00% | 27% | 27% | 27% | 42% | 43% | 43% |
| Bidar | 2.69% | 5.73% | 4.17% | 36% | 28% | 31% | 65% | 47% | 52% |
| Bijapur | 4.14% | 8.85% | 6.56% | 39% | 27% | 31% | 57% | 47% | 50% |
| Chickmagalur | 1.48% | 5.40% | 3.37% | 51% | 35% | 42% | 81% | 55% | 67% |
| Chitradurga | 3.94% | 8.24% | 5.97% | 34% | 26% | 29% | 54% | 41% | 46% |
| Dak. Kannad | 1.27% | 7.65% | 4.59% | 50% | 27% | 34% | 80% | 34% | 47% |
| Dharwad | 3.77% | 6.53% | 5.15% | 42% | 38% | 40% | 64% | 55% | 58% |
| Gulbarga | 3.71% | 6.99% | 5.37% | 48% | 26% | 33% | 64% | 44% | 50% |
| Hassan | 2.10% | 3.40% | 2.74% | 51% | 40% | 44% | 66% | 64% | 64% |
| Kodagu | 1.88% | 1.25% | 1.58% | 40% | 47% | 45% | 57% | 75% | 68% |
| Kolar | 5.10% | 6.36% | 5.70% | 24% | 20% | 22% | 47% | 38% | 42% |
| Mandya | 3.40% | 6.00% | 4.65% | 47% | 44% | 45% | 66% | 58% | 61% |
| Mysore | 2.00% | 6.35% | 4.05% | 46% | 31% | 36% | 70% | 47% | 55% |
| Raichur | 4.35% | 6.72% | 5.58% | 24% | 29% | 28% | 46% | 50% | 49% |
| Shimoga | 3.12% | 5.24% | 4.12% | 44% | 35% | 39% | 66% | 56% | 60% |
| Tumkur | 5.70% | 9.01% | 7.24% | 44% | 33% | 37% | 56% | 49% | 51% |
| Uttar Kannad | 3.42% | 4.60% | 4.00% | 41% | 44% | 43% | 50% | 60% | 57% |
| Karnataka | 3.39% | 6.51% | 4.93% | 40% | 32% | 35% | 60% | 49% | 53% |
The number of persons with bilateral operable cataract increases from 1,157 to 3,345, depending upon the level of visual acuity, while the number of persons with bilateral aphakia remains the same. Similarly, the number of operable cataract eyes increases from 4,481 for VA<3/60 to 11,511 for VA<6/18, while the number of aphakic eyes remains the same.
At VA<3/60, 34.9% of all cataract blind eyes and 53.2% of all bilateral cataract blind persons have been operated upon, assuming that only people with cataract and a VA<3/60 were eligible. As expected, the coverage indicators for VA<6/60 and VA<6/18 are lower: 40.1% and 26.2% for persons and 26% and 17.3% for eyes respectively. Nearly 77% of all operations were performed in the first eye, and 23% in the second eye.

Eye camp surgery in India: post-operative inpatients
Photo: Murray McGavin
Table 2 gives the prevalence of bilateral cataract blindness, CSC(eyes) and CSC(persons) for each district and also by gender. One might expect that a district with a high surgical coverage would have a low prevalence. However, that is not always the case. Mandya District, for example, has a prevalence rate three times higher than Kodagu District, while the coverage indicators for persons and eyes are nearly the same. It can also be seen, from Table 2, that the prevalence of cataract blindness for females is nearly twice as high as for males. The differences in coverage are less marked.
Table 3 gives the results of the rapid assessment in Ahmedabad. Here the situation is different. There are many more persons with bilateral (pseudo)aphakia than with bilateral blindness, or severe visual impairment due to cataract. The number of (pseudo)aphakic eyes is 5 times higher than the number of cataract blind eyes. For operable cataract eyes (VA<6/60) it is more than twice as high and for VA<6/18 there are slightly more aphakic eyes than eyes with operable cataract. The Cataract Surgical Coverage is 92.9% for blind persons (VA<3/60) and 83.1% for eyes, assuming that only people with cataract and a VA<3/60 had been operated on. The Coverage of <6/60 is 84.5% for persons and 71.5% for eyes.
Table 3.
Cataract Surgical Coverage from Sample Data on Operable Cataract and Aphakia in Ahmedabad District (1997)
| Category | Condition | VA<3/60 | VA<6/60 | VA<6/18 | ||
|---|---|---|---|---|---|---|
| ∗b is defined as all eyes with cataract causing an acuity of less than 3/60, 6/60 or 6/18. | ||||||
| ∗∗a is defined as all eyes which are aphakic or (pseudo)aphakic, regardless of acuity. | ||||||
| z | No. persons with bilateral operable cataract | 26 | 69 | 206 | ||
| y | No. persons bilaterally (pseudo)aphakic | 292 | 292 | 292 | ||
| x | No. persons one eye aphakic + one eye operable cataract | 47 | 83 | 139 | ||
| b∗ | No. operable cataract eyes∗ | 158 | 310 | 689 | ||
| a∗∗ | No. (pseudo)aphakic eyes∗∗ | 776 | 776 | 776 | ||
| % | first eyes | 62.4% | (a-y)/a | |||
| % | second eyes: | 37.6% | y/a | |||
| Cataract Surgical Coverage (eyes) | a/(a+b) | 83.1% | 71.5% | 53.0% | ||
| Cataract Surgical Coverage (persons) | (x+y)/(x+y+z) | 92.9% | 84.5% | 76.7% | ||
The coverage of visually impaired cataract (VA<6/18) is higher in Ahmedabad than in Karnataka, indicating that surgical intervention is being undertaken at an early stage of visual loss. More second eyes (37.6%) have been operated in Ahmedabad than Karnataka.
The problem of cataract blindness seems to be under control in Ahmedabad and the capacity to provide surgical services is sufficient to cater for the needs of most people in the district. Nevertheless, we still found 26 persons who were bilaterally blind (VA<3/60) from cataract in the sample. These patients were asked in the survey why they had not been operated on so far. Six patients mentioned ‘medical contra-indications’ and seven ‘no felt need’; the remaining patients a variety of other reasons. This may be the ‘hard core’ of the cataract problem - the patients who cannot or do not want to have surgery.
Discussion
Prevalence of cataract blindness along with Cataract Surgical Coverage can give important information about the impact of a cataract intervention programme. The surgical coverage for persons indicates to which extent people, disabled by bilateral operable cataract, had surgery in one or both eyes. It relates directly to the prevalence of bilateral cataract blindness.
Cataract surgical coverage for eyes also includes people with operable cataract in one eye and a normal other eye. It relates more to the total surgical workload for the ophthalmologists.
Both indicators only provide quantitative data. Visual outcome is not taken into account and can be calculated separately from the same data.
Indicators obtained through population based surveys are influenced by events over a previous period of several years. The effects of recent changes in strategy are likely to be diluted by effects from the period before the change in strategy. Prevalence and coverage data should be collected at regular intervals, say every 3–5 years, to reveal trends. Rapid assessments, conducted by local staff, using simple, standardised survey methodology and software for data analysis, can be undertaken.
As can be seen from Karnataka, usually a lower prevalence of cataract blindness is linked with a higher coverage. The factors that determine this relation are the proportion of first eyes being operated on and the proportion of operations on eyes not yet blind.
It is not always possible to assess in retrospect whether a person with one or two aphakic eyes was actually blind (VA<3/60), severely visually impaired (VA<6/60) or visually impaired (VA<6/18) at the time of surgery. The proportion of operations on non-cataract blind patients is difficult to assess. In Karnataka state, the results show that only 5% of all surgeries were with intraocular lens implantation.5 Most cataract surgeries were done on patients or eyes with a VA<3/60 and hence, the cataract surgical coverage for this level will be fairly correct.
In Ahmedabad district, however, many more people with a VA better than 3/60 were also operated upon. In such situations, it will be more accurate to use the cataract surgical coverage at level <6/60 or even <6/18.
It is possible to assess the visual acuity of all (pseudo) aphakic eyes in the sample to assess outcome, and look at the reasons for failure. If patient records are available, the proportion of first eyes and second eyes can be calculated and this can give an impression of utilisation of resources.
By comparing pre-operative vision with post-operative vision the Success Rate and the Sight Restoration Rate can be calculated. This indicates the proportion of all cataract operations which change a blind person into a sighted person.7 Such outcome indicators reveal the quality of cataract surgery and visual rehabilitation.
Cataract blindness is a dynamic entity, determined by demographic changes in the population, incidence of cataract blindness, and quality and quantity of the surgical services provided. These dynamics are difficult to capture in time bound static indicators. One should not look at coverage data in isolation but use them in combination with other parameters.
What is really needed is a mathematical simulation model that can capture these dynamics and can predict future trends in cataract blindness.8 The indicators described above can assist in developing such a model.
Contributor Information
Hans Limburg, Chief Adviser DANPCB, A1/148 Safdarjung Enclave, New Delhi 110029, India.
Allen Foster, Senior Lecturer, International Centre for Eye Health, 11–43 Bath Street, London EC1V 9EL, UK.
References
- 1.Central Ophthalmic Cell, Ministry of Health & Family Welfare, Government of India: Annual Results Cataract Performance
- 2.The Epidemiology of Blindness in Nepal - Report of the 1981 Nepal Blindness Survey. The Seva Foundation. 1988 [Google Scholar]
- 3.Foster A. A simple method for evaluating surgical cataract services in prevention of blindness programmes. J Comm Eye Health. 1992;10:2–5. [Google Scholar]
- 4.Limburg H, Kumar R, Indrayan A, Sundaram KR. Rapid Assessment of Prevalence of Cataract Blindness at District Level. Int J Epidemiol. 1997;26:1049–54. doi: 10.1093/ije/26.5.1049. [DOI] [PubMed] [Google Scholar]
- 5.Limburg H, Kumar R. Follow-up study of blindness attributed to cataract in Karnataka state of India – results from district level rapid assessments (submitted for publication) [DOI] [PubMed]
- 6.Limburg H, Vasavada A, Muzumdar G, Khan MY, Vaidyanathan K. Rapid assessment of cataract blindness in an urban setting – results from a survey in Ahmedabad District, Gujarat (submitted for publication)
- 7.imburg H, Kumar R, Bachani D. Monitoring and evaluating cataract intervention in India. Br J Ophthalmol. 1996;80:951–5. doi: 10.1136/bjo.80.11.951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Limburg H, Kumar R, Bachani D. Forecasting cataract blindness - and planning to combat it. World Health Forum. 1996;17:15–20. [PubMed] [Google Scholar]